Purpose
To evaluate the effects of the Boston Ocular Surface Prosthesis (Boston Foundation for Sight, Needham, Massachusetts, USA) on visual acuity (VA) and visual functioning in patients with severe corneal ectasia, irregular astigmatism, or ocular surface disease.
Design
Prospective, interventional case series.
Methods
The study examined the effects of this prosthesis on VA and visual functioning in consecutive patients with corneal ectasia, irregular astigmatism, or ocular surface disease who had failed conventional therapies and were seen at the Boston Foundation for Sight between January 1 and June 30, 2006. Outcomes were best-corrected VA using Snellen charts and visual functioning using the National Eye Institute Visual Functioning Questionnaire (NEI VFQ-25) at 6 months. Clinical data were abstracted from medical records.
Results
Of the 101 patients, 80 were fitted with a prosthesis in one or both eyes, and follow-up Visual Functioning Questionnaire data were obtained in 69 eyes. Best-corrected VA improved by a change in mean logarithm of the minimal angle of resolution (logMAR) units of −0.39 (converted from Snellen) with a change of −0.54 logMAR units in patients with ectasia or astigmatism and −0.22 logMAR units in patients with ocular surface disease. Mean composite visual functioning scores increased from 57.0 to 77.8 ( P < .0001). Improvements in composite Visual Functioning Questionnaire scores were similar in patients with ectasia or ocular surface disease; but vision-related subscores improved more in patients with ectasia, whereas subscores for ocular pain, role difficulties, and dependency improved more in patients with ocular surface disease.
Conclusions
The Boston Ocular Surface Prosthesis significantly improved VA and visual functioning in patients with corneal ectasia, irregular astigmatism, and ocular surface disease who had failed conventional therapies.
Corneal ectasia, irregular astigmatism, and ocular surface disease rank high in the United States as causes of decreased visual acuity (VA) and other eye symptoms. Keratoconus affects between 1 in 500 and 1 in 2000 Americans, and other forms of irregular astigmatism are only slightly less frequent. Conventional corneal contact lenses improve vision in such individuals, but become less and less well tolerated as the disease progresses. Ocular surface disease is a heterogeneous group of conditions that includes dry eye syndrome and immunologic disorders such as Stevens-Johnson syndrome and chronic graft-versus-host disease. In milder forms, these conditions can be treated with topical or systemic medications and soft bandage lenses. However, the symptoms and corneal complications associated with advanced disease often are managed inadequately by conventional measures.
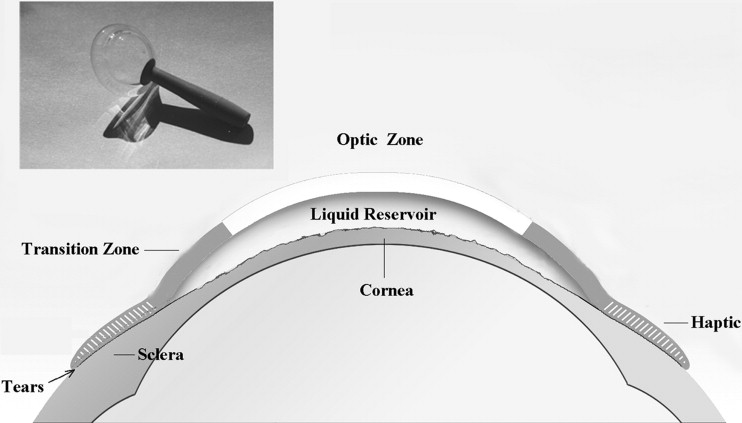
The Boston Ocular Surface Prosthesis (Boston Foundation for Sight, Needham, Massachusetts, USA), a scleral lens that was approved by the Food and Drug Administration in 1994, has been used to improve visual function in individuals with severe keratoconus whose vision is not corrected adequately with spectacles or who are intolerant of contact lenses and would otherwise require corneal transplantation. This device also has been used to reduce symptoms and to improve corneal integrity in eyes with refractory ocular surface disease. The prosthesis ( Figure 1 ) is a gas-permeable scleral lens that vaults the cornea and submerges the entire corneal surface in a pool of oxygenated artificial tears. Each device is custom designed and manufactured using computer-aided design and computer-aided manufacturing technology linked to a high-precision, high-resolution, computerized lathe. The device design features an optic portion linked to a customized bearing haptic portion that aligns precisely with the sclera. Spline functions are use throughout to create seamless transition zones, allowing control of vault independent of base curve. The safety and efficacy of the device have been reported in patients with keratoconus, Steven-Johnson syndrome, severe dry eye syndrome, chronic ocular graft-versus-host disease, and those with reduced VA after penetrating keratoplasty, laser in situ keratomileusis, or other types of eye surgery. A retrospective observational study of 33 patients with chronic graft-versus-host disease found substantial improvements in eye pain, photophobia, driving vision, reading vision, and the quality of life in most participants.
The present study uses a prospective design to evaluate the clinical effects of the prosthesis in patients with ectasia, irregular astigmatism, or ocular surface disease who were referred to the Boston Foundation for Sight clinics because of persistent and disabling eye symptoms, impaired vision, or both. An economic assessment of the prosthesis in the same clinical population also has been performed.
Methods
Study Population and Medical Record Abstraction
The study includes 101 individuals who were seen for the first time at the Boston Foundation for Sight for corneal disease between January 1 and June 30, 2006, because they had not responded satisfactorily to conventional treatments. Medical records were abstracted using an explicit, pretested, data-extraction instrument to obtain pretreatment information on patients’ demographic characteristics, eye and any related systemic diagnoses, contact lens tolerance, eye medications, eye pain and photophobia, and best-corrected visual acuity (BCVA). The posttreatment data focused on the eyes that were fitted with a prosthesis, the number of clinic visits and length of time required to complete fitting, BCVA after fitting, and reasons a prosthesis was not fitted when this was the case. The National Eye Institute’s validated Visual Functioning Questionnaire (VFQ-25) was completed at the first consultation visit and again 6 months after the prosthesis was fitted. The questionnaire was administered either in person or by telephone interview by a trained interviewer who was not otherwise involved in the patient’s care. Medical record data were abstracted by experts in ophthalmology (D.S.J.) and optometry (L.J.) and by the principal investigator (W.B.S.). Abstraction forms were reviewed for completeness, and questions of consistency were resolved.
Visual Acuity
BCVA was measured using Snellen scores with glasses or contact lenses (habitual vision correction) at baseline and after the prosthesis had been fitted. Scores were measured using standardized illumination with the projected image calibrated for the length of the examination room. Improvements in VA are reported for each fitted eye and also as the change in VA in the patient’s better eye before and after fitting. The focus on VA in the better eye reflects its closer relationship with visual functioning among patients with impairments of vision. Improvements in VA were analyzed in terms of changes in Snellen scores and as changes in the logarithm of the minimal angle of resolution (logMAR) VA where negative changes reflect improved VA.
Visual Functioning
The VFQ-25 was administered at the time of initial clinic visits and again by telephone 6 months later using a standardized script. Data were scored using the National Institutes of Health/National Eye Institute scoring algorithm that converts a base set of 25 vision-targeted questions into 11 vision-related constructs, plus as single-item general health rating question. Scoring is a two-step process that first converts responses to a 0 to 100 scale and then averages scores for each of the subscales. Higher scores represent better functioning. Under standard scoring procedures, missing data are excluded when subscale scores are calculated. The composite VFQ-25 score is an unweighted average of the vision-targeted subscale scores and excludes the general health rating question. Subscales measure general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, color vision, and peripheral vision.
Our study builds on the work done by Steinberg and associates, who developed the Visual Functioning Index 14 (VF-14), which they applied to patients with cataracts. Boisjoly and associates used the VF-14 and other questionnaires to assess global measures of visual symptoms in patients undergoing corneal transplantation. Both groups concluded that visual function impairment was a valid and useful index of outcomes and often was better than VA alone. Steinberg and associates found a statistically significant association of 0.27 between the VF-14 score and VA in the better eye. We verified these investigators’ findings by demonstrating a moderate correlation between VA (Snellen scores) in the better eye and visual function assessed using VFQ-25 scores in our clinical population ( r = 0.49; P < .0001).
Statistical Methods
Differences in baseline characteristics between patients who received a prosthesis and those who did not despite being clinically eligible were calculated using two-tailed t tests for continuous variables and 2 × 2 Chi-square tests for categorical variables. Standardized differences were used to calculate the magnitude of differences for continuous variables or proportions by dividing the difference by the pooled standard deviation. Standardized differences are on a scale similar to a normal or z-score.
Analyses of changes in VA and visual functioning (VFQ-25 scores) between baseline and follow-up were performed for patients who received a prosthesis and had observations at both time points. Changes in VA are expressed as changes in VA groupings that reflect well-accepted functional equivalents of Snellen scores and also by converting Snellen values to logMAR VA. Results are reported both for eyes fitted with a prosthesis and as changes in the VA in the patient’s better eye. The former reflects the technical ability of the prosthesis to improve vision, whereas the latter correlates better with improvements in visual functioning. The statistical significance of changes in the logMAR VA was calculated using t tests. Changes in visual functioning were calculated both for the composite VFQ-25 score and individual subscores using two-sided t tests to examine whether differences were significantly different from 0.
Multivariable regression models were constructed to assess the relationships between patient characteristics (independent variables) and changes in VFQ-25 scores (dependent variable). The statistical significance of independent variables was tested using the t statistic, and the significance of the model was estimated using an F test.
Results
Patient Characteristics
Eighty patients received a prosthesis for one or both eyes. The principal eye diagnosis was corneal ectasia or irregular astigmatism in 54 patients and ocular surface disease in 47 patients. Sixteen patients had undergone a previous corneal transplantation, and 3 previously had undergone laser in situ keratomileusis (2 with ectasia and 1 with dry eye syndrome). Baseline characteristics are summarized in Table 1 . The population contained approximately equal numbers of men and women and had a mean age of 44 years. Three patients were 18 years of age or younger and 14 were 60 or older. Nearly one half were experiencing photophobia, and one-third reported eye pain. Patients who received at least 1 prosthesis had somewhat greater compromise of visual function (VFQ scores 57.6 vs 65.1; P = .10) and lower likelihood of receiving systemic medications as treatment for their eyes (20% vs 38%; P = .09). Secondary eye diagnoses were more frequent in patients with ocular surface disease than ectasia (87% vs 37%; P < .0001), including 68% having undergone punctal occlusion, having a surface breakdown in 64%, and lid problems in 36%.
| Characteristic | Received Prosthesis (n = 80) | No Prosthesis (n = 21) | P values a |
|---|---|---|---|
| Primary eye diagnosis (no. of patients) | |||
| Ocular surface disease | 38 | 9 | |
| Dry eye syndrome | 18 | 3 | .55 |
| Chronic graft- vs-host disease | 11 | 3 | .99 |
| Other | 9 | 3 | .71 |
| Corneal ectasia or irregular astigmatism | 42 | 12 | |
| Keratoconus | 32 | 9 | .81 |
| Other | 10 | 3 | .70 |
| Other patient characteristics | |||
| Mean age (years) | 44.0 | 45.0 | .81 |
| Baseline composite VFQ score mean | 57.6 | 65.1 | .11 |
| Gender (% female) | 49% | 48% | .99 |
| Habitual vision correction | |||
| Spectacles | 48% | 52% | .81 |
| Contact lenses | 23% | 19% | .99 |
| Photophobia in either eye | 48% | 43% | .81 |
| Eye pain in either eye | 36% | 24% | .32 |
| Topical treatment for eyes (% yes) | 41% | 48% | .63 |
| Systemic treatment for eyes (% yes) | 20% | 38% | .09 |
a P value based on t test for continuous variables and Fisher exact test for 2 × 2 categories.
Baseline Levels of Visual Acuity
Baseline levels of BCVA are shown in Table 2 for the patients’ better eyes of all candidates for an ocular surface prosthesis and in Table 3 for each eye in the 80 patients who received at least one prosthesis. Emphasis is placed on the better eye because of its stronger correlation with visual functioning. Results are shown as Snellen score groupings that represent commonly accepted visual functioning equivalents. Patients who received a prosthesis were somewhat less likely to have normal or near-normal vision in their better eyes than those who did not (46% vs 62%; P = .23). Patients with corneal ectasia were less likely to have normal VA (29% vs 66%; P = .002) than those with ocular surface disease.
| Visual Acuity | Received Prosthesis | No Prosthesis (n = 21) | ||
|---|---|---|---|---|
| All (n = 80) | Diagnosis Surface Disease (n = 38) | Diagnosis Ectasia (n = 42) | ||
| 20/10 to 20/35 (at or near normal) | 46% | 66% | 29% | 62% |
| 20/40 to 20/60 (moderate deficit) | 34% | 24% | 43% | 14% |
| 20/70 to 20/190 (severe deficits a ) | 10% | 3% | 17% | 5% |
| 20/200 to 20/390 (legally blind) | 0% | 0% | 0% | 10% |
| 20/400 to 20/900 (nonambulatory) | 9% | 5% | 12% | 0% |
| 20/1000 or worse (counting fingers or hand movements, light perception) | 1% | 3% | 0% | 10% |
a Lowest end of occupational vision range. Total percentages may not sum to 100% because of rounding errors.
| Visual Acuity | Eyes Receiving Prosthesis | Eyes with No Prosthesis (n = 17) | ||
|---|---|---|---|---|
| All Eyes (143 Eyes) | Diagnosis Surface Disease (n = 68) | Diagnosis Ectasia (n = 75) | ||
| 20/10 to 20/35 (at or near normal) | 30% | 48% | 13% | 47% |
| 20/40 to 20/60 (moderate deficit) | 32% | 32% | 32% | 2 |
| 20/70 to 20/190 (severe deficits a ) | 15% | 8% | 21% | 2 |
| 20/200 to 20/390 (legally blind) | 8% | 3% | 12% | 0% |
| 20/400 to 20/900 (nonambulatory) | 12% | 6% | 17% | 0% |
| 20/1000 or worse (counting fingers or hand movement, light perception) | 4% | 3% | 4% | 35% |
Reasons for Not Fitting a Prosthesis
The fitting procedure was not completed or was deferred in 21 patients, including 11 in whom a delay in obtaining approval of insurance coverage was responsible and 6 in whom the prosthesis did not improve VA. Other reasons included difficulty fitting the device, its failure to relieve symptoms, and, in one patient, that it felt “too wet.”
Changes in Visual Acuity in Patients’ Fitted Eyes
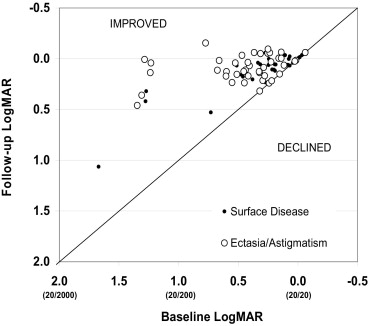
Vision was improved by at least 1 Snellen group in 73% of fitted eyes and by 2 groups or more in 38% of eyes ( Table 4 ). Improvements in VA were greater in patients with ectasia than in those with surface disease (improvements of at least 1 group in 86% vs 58%; P < .001; and by 2 or more groups in 55% vs 19%; P < .0001; respectively). Analysis of the logMAR of Snellen values shows that improvements were largest in eyes with severe baseline deficits (20/200 or worse, corresponding to 1.0 logMAR or higher; Figure 2 ). In this scatterplot, decreases in logMAR values represent improvements in vision, as do points above the no change line. For example, the left-most circles (representing patients with ectasia) indicate improvements of vision from logMAR values of more than 1.5 (Snellen equivalent, approximately 20/1000 or worse) to logMAR values ranging from 0.0 (normal vision) to 1.0 (Snellen equivalent, 20/200). The mean change in logMAR VA was −0.39 ( P < .001) in all eyes, including a change of −0.54 in patients with ectasia ( P < .001) and −0.22 in patients with ocular surface disease ( P < .001). Improvements in the logMAR of VA were strongly correlated with more severe baseline visual deficits ( P = .001) and were significantly greater in patients with ectasia than surface disease after controlling for baseline levels of VA ( P = .003; Table 5 ). Other patient-level variables such as age and gender were not statistically significantly associated with improvements in VA.
| Change in Visual Acuity | All Fitted Eyes (n = 141), % | Surface Disease Diagnosis (n = 66), % | Ectasia/Astigmatism Diagnosis (n = 75), % |
|---|---|---|---|
| Vision worse | 0 | 0 | 0 |
| No change | 27 | 42 | 12 |
| Improve | |||
| One line | 35 | 39 | 32 |
| Two lines | 23 | 15 | 29 |
| Three lines | 7 | 2 | 12 |
| Four lines | 6 | 2 | 11 |
| Five lines | 1 | 0 | 3 |
| Explanatory Variable | Coefficient | P value |
|---|---|---|
| (Constant) | −0.85 | <.001 |
| Baseline logMAR visual acuity | 0.7 | <.001 |
| Diagnosis of surface disease | −0.11 | .003 |
Changes in Visual Acuity in Patients’ Better Eyes
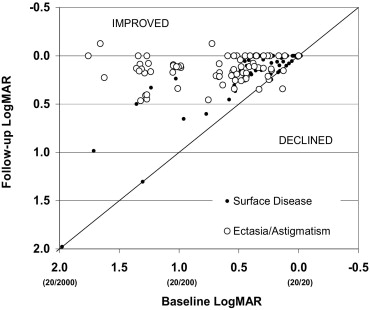
Patterns of improvement were similar to those in fitted eyes, but were somewhat less dramatic. Improvements of one or more visual groups occurred in 62% of all patients, including 71% with corneal ectasia and 51% of patients with ocular surface disease. The mean improvement in the logMAR VA was 0.27 ( P < .001) overall, 0.36 ( P < .001) in patients with ectasia or astigmatism, and 0.17 in patients with ocular surface disease ( P < .001). The scatterplot in Figure 3 shows consistent improvements in VA in the better eye. Especially large improvements were noted in 5 patients with ectasia and in 2 patients with ocular surface disease who were legally blind (Snellen 20/200 or worse) at baseline and improved to 20/100 or better with the use of the prosthesis.