, Rudolf Leuwer2, Konrad Schwager3 and Sören Wenzel4
(1)
Otology and Neurotology Division, University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA
(2)
Otorhinolaryngology Head and Neck Surgery, HELIOS Hospital, Krefeld, Germany
(3)
Otorhinolaryngology Head and Neck Surgery, Klinikum Fulda, Fulda, Germany
(4)
Otorhinolaryngology Head and Neck Surgery, Pinneberg, Germany
Eustachian tube assessment methods
Cartilage
Lumen: Rüdinger’s safety canal, auxiliary gap and microturbinates
Muscles
Ligaments
Medial and lateral Ostmann’s fat pad
1.1 Introduction
Although there were very early postulations of an airway between the middle ear and the upper airway by Aristotle [40], Bartolomeo Eustachio was the first to exactly describe the auditory tube [146]. It was Valsalva who posthumously suggested naming the auditory tube after its discoverer [7]. Eustachio believed that the tube had to be open under normal conditions [155]. Also, the anatomist Duverney claimed the Eustachian tube (ET) to be permanently open, but he described the airway as bidirectional and claimed there was a second function of the tube: the clearance of fluids from the middle ear [40].
The Eustachian tube anatomy and its clinical significance have been studied using human cadaveric temporal bone specimens as well as CT and MRI studies of living subjects [191]. However, some details should still be discussed.
The Eustachian tube is divided into an osseous posterolateral and a fibrocartilaginous anteromedial portion. Whereas the osseous portion is mainly formed by the petrous part of the temporal bone, the anatomy of the flexible fibrocartilaginous portion is more complex. It is quite obvious that the fibrocartilaginous portion represents the active Eustachian tube function, but the understanding of how the surrounding elements interact remains controversial.
For example, there is a contradictory discussion about the 3D anatomy and function of the tensor veli palatini muscle [52]. Luschka [101], Rüdinger [161] and Proctor [147] called the tensor veli palatini muscle a “dilatator tubae”. Dayan et al. [26] also used this term, but they noticed that the two portions of the tensor veli palatini muscle have different mechanical purposes and thus justified the use of the word “tensor”. Seif and Dellon [175], on the other hand, called the tensor veli palatini muscle a “compressor tubae”. Finally, Pahnke [135] and Gannon et al. [47] described both its impact upon the opening as well as closing function of the Eustachian tube.
It is one of the key merits of Joseph Toynbee to point out that the Eustachian tube is closed at rest and that it only opens for a short period when swallowing [190].
In fact, the Eustachian tube, its numerous morphologic variations [132] and its developmental changes [36] as well as its opening and closing function [70] are still difficult to understand today.
MRI is an excellent method to assess the anatomical landmarks in and around the Eustachian tube [99]. Even the opening and closing function can be demonstrated when using appropriate protocols [93]. However, not only MRI, but also low-dose sequential CT scans are suitable to assess the anatomy as well as the function of the Eustachian tube. The resolution of these scans being sufficient, the advantage of this technique is the ability to take rapid sequential scans [113].
1.2 Orientation and Length
Starting from its pharyngeal orifice, the Eustachian tube has a posterior, lateral and superior direction towards the middle ear [146]. The axis of the tube in adults is about 45° to the sagittal, frontal and horizontal planes of the skull [216]. In children the angle to the horizontal plane is significantly smaller than in adults [196]. The axis has a shallow angulation between the cartilaginous and the osseous portion of the tube, with an obtuse inferior angle. The lumen of the cartilaginous Eustachian tube forms a perpendicular gap with a minor gyration towards the pharyngeal orifice.
The total length of the Eustachian tube is variable. In adults it varies from 31 to 44 mm [146, 216]. In newborns the tubal length is about one half of the adult’s [208]. The osseous part of the tube measures about one-third and the cartilaginous part two-thirds of the total length. In children, however, the relative share of the osseous part is bigger than in adults. The osseous and cartilaginous parts of the tube interlock like a seam. The average length of the tubal cartilage is 31.5 mm [135]. This cartilage extends into the roof of the osseous part [100]. That is why the borderline between the osseous and the cartilaginous part of the Eustachian tube is found between its rigid and flexible portion. Hence, the length of the tubal cartilage and the length of the cartilaginous part of the Eustachian tube are not the same. According to Zöllner [216] the distance between the pharyngeal orifice and the isthmus is 24–28 mm, but we have to take into account that there is no exact definition of the measuring points.
1.3 Compartments
Figure 1.1 is a graphic frontal plane of the Eustachian tube and shows its main compartments: the cartilage, the lumen, the ligaments, the Ostmann’s fat pad and the muscles.
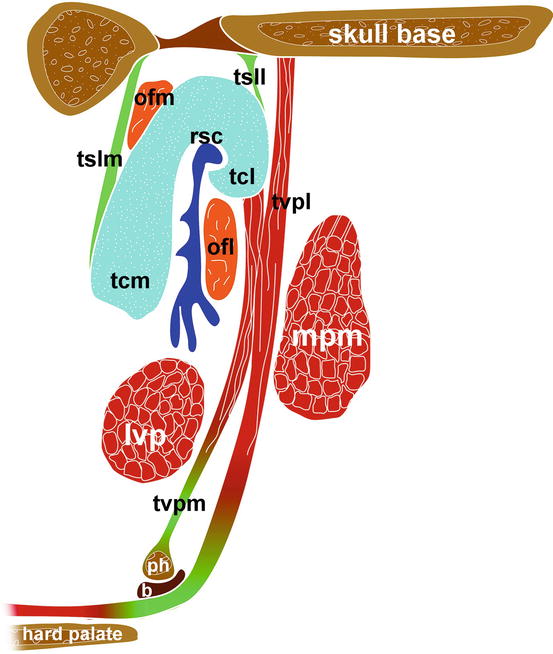
Fig. 1.1
Graphic frontal plane of the Eustachian tube. tvp m tensor veli palatini muscle, medial layer, tvp l lateral layer, ph pterygoid hamulus, b bursa, lvp levator veli palatini muscle, mpm medial pterygoid muscle, tcm tubal cartilage, medial lamina, tcl lateral lamina, ofm medial Ostmann’s fat pad, ofl lateral Ostmann’s fat pad, tslm medial tubal suspensory ligament, tsll lateral tubal suspensory ligament, rsc Rüdinger’s safety canal
1.3.1 Cartilage
The cartilage of the Eustachian tube is one of the most important structures for understanding Eustachian tube function. Together with the tensor veli palatini muscle, it almost completely surrounds its fibrocartilaginous portion [132]. The cross section of the cartilage close to the pharyngeal orifice shows that it is “a dome-shaped structure with arms of different lengths” [12]. In other words, it forms the shape of a shepherd’s crook with a bigger medial and a smaller lateral lamina [161, 216]. The mean height of the medial lamina is 5.1 mm and that of the lateral lamina 1.8 mm. The lateral lamina has a much more constant height than the medial (Fig. 1.2). The thickness of both parts is equal in the middle portion of the Eustachian tube. In comparison to the medial lamina, the lateral lamina becomes thinner towards both orifices. The transition zone between each lamina is not precisely defined [136]. Oshima et al. [132] found a wide variation of the actual shape of the cartilage using MRI studies. The physiological background of these variations still is unknown. Pahnke [136] described that in about 25 % of his specimens, the lower end of the medial lamina forms a hook around the lower portion of the Eustachian tube lumen. In some cases fragments of cartilage seem to be separated from the main cartilage. These fragments can be found on both sides of the medial lamina of the cartilage [161]. However, tracing the adjacent histological specimen shows that there is a continuous connection in most cases [5].
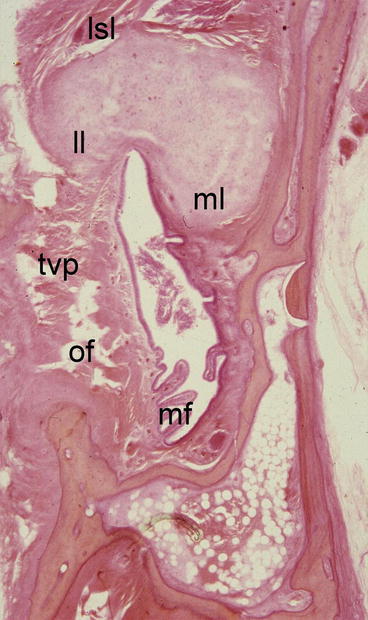
Fig. 1.2
Histological specimen of the Eustachian tube near the skull base. Note the minor height of the medial lamina of the tubal cartilage (from the historical Wittmaack-collection, Hamburg University Medical School). lsl lateral tubal suspensory ligament, ll lateral lamina of the tubal cartilage, ml medial lamina of the tubal cartilage, tvp tensor veli palatini muscle, of Ostmann’s fat pad, mf mucosal folds
There is a gradual transition between the osseous and the fibrocartilaginous part of the Eustachian tube. Rüdinger [161] could show that there is a fibrocartilaginous mass connecting the bone on one hand and the hyaline cartilage on the other hand. That is why the length of the cartilage alone (31.2 mm) differs from the length of the cartilaginous part of the Eustachian tube (26 mm). Occasionally the cartilage may even reach the tympanic orifice of the tube [135].
The medial layer of the tensor veli palatini muscle is attached to the lateral lamina of the cartilage except for the anterior quarter of the fibrocartilaginous portion. The levator veli palatini muscle has a very constant relationship to the anterior part of the cartilage. However, there is no direct contact between muscle and cartilage [73].
The elasticity of the tubal cartilage is similar to that of the pinna or the nose [12]. Matsune et al. [109] examined the density of elastin in the intermediate portion between the medial and the lateral lamina of human Eustachian tube cartilage specimens. It was higher in adults. They believe that this elasticity is mandatory for reset forces after the contraction of the tensor veli palatini muscle.
1.3.2 Lumen
The lumen of the Eustachian tube is remarkable because it is not a tube. According to Rüdinger [161], the cross-sectional view through the lumen shows two different compartments:
A.
The first compartment is a half-cylindrical space between the medial and the smaller lateral lamina of the tubal cartilage with a diameter of 0.4–0.5 mm, which is called Rüdinger’s safety canal (Fig. 1.3, from [161]). This space is filled with air or with mucus. It is found in about 85 % of adult individuals [135]. Honjo et al. [70] could visualize this canal in two different X-ray examinations using contrast media. This space is likely always open [161].
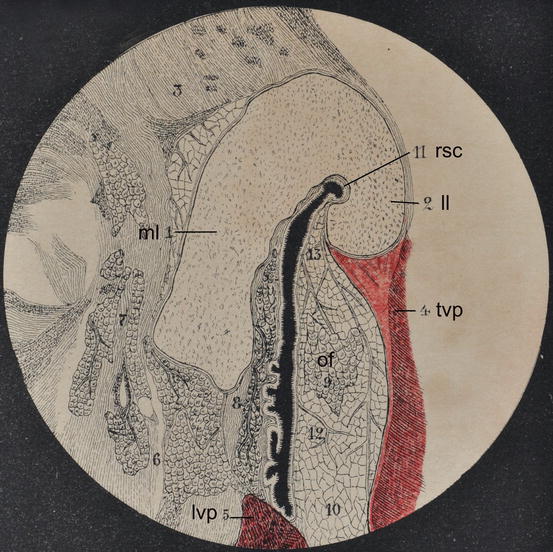
Fig. 1.3
Original illustration from the first edition of [161], showing Rüdinger’s safety canal in humans. rsc Rüdinger’s safety canal, ll lateral lamina of the tubal cartilage, ml medial lamina of the tubal cartilage, tvp tensor veli palatini muscle, of (lateral) Ostmann’s fat pad, lvp levator veli palatini muscle
B.
Below the safety canal, there is a second space Rüdinger called the “auxiliary gap”. This gap plays an important role in clearance and protection. Although we usually talk about the Eustachian “tube”, the term “gap” helps to understand the complex Eustachian tube function.
Inside the auxiliary gap, there are longitudinal mucosal folds [161]. These folds are mainly located in the posterior, i.e. medial, wall of the gap. There are significant differences in the number of these folds in paediatric and adult populations. Sando et al. [168] and Ozturk et al. [134] emphasize that these “microturbinates” may contribute to the clearance and protection function of the auxiliary gap.
Matsune et al. [109] could demonstrate that there is mucosa-associated lymphatic tissue within the cartilaginous portion of the Eustachian tube. Lymphatic tissue of the nasopharynx, however, does not extend into the tube [5]. The pharyngeal tonsil may reach the tubal torus and may even deform it, but this does not necessarily induce a tube malfunction [164]. On the other hand, children with recurrent otitis media with effusion may benefit from adenoidectomy due to the removal of an infectious source rather than from the removal of the adenoidal mass [138].
Between the tympanal and the pharyngeal orifice, the vertical diameter of the tube increases from a minimum of 3.5 mm in the petrous portion of the temporal bone [12] to a maximum of 6–10 mm at 6–7 mm proximally to the pharyngeal orifice [135]. The increase is not necessarily continuous. For example, close to the pharyngeal orifice, there is a local dilation of the lumen called Kirchner’s diverticulum.
1.3.3 Ligaments
The cartilaginous part of the Eustachian tube is firmly attached posteriorly to the osseous orifice by fibrous bands [36] and to the skull base by the superior tubal ligament [147]. This ligament is also called the tubal suspensory ligament [216]. Due to a small fat pad behind the medial lamina of the cartilage, the so-called medial Ostmann’s fat pad, the fibrous plate is divided into a lateral and a medial suspensory ligament. Both ligaments reach the tubal cartilage laterally and medially in a nearly tangential way. The lateral suspensory ligament passes into the tendon of the lateral layer of the tensor veli palatini muscle. On the superficial side of the tensor veli palatini muscle, there is a fascia called the Weber–Liel fascia. This fascia arises from the skull base and separates the tensor from the medial pterygoid muscle. We learn more about this fascia in Chap. 3. There is another fascial plate on the medial side of the tensor muscle. This facia is connected to the lateral lamina of the tubal cartilage and passes the lateral boundary of the lateral Ostmann’s fat pad. The lower end of this fascia passes into the salpingopharyngeal fascia, also called von Tröltsch fascia. Hence, strong fasciae that connect the Eustachian tube and the pharynx encase the tensor veli palatini muscle.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


