Purpose
To report the occurrence of chronic hypotony as a complication following Boston type 1 keratoprosthesis (KPro) implantation and to determine associated risk factors.
Design
Retrospective case series.
Methods
The medical records of all patients undergoing KPro implantation between January 2004 and November 2010 at the Wilmer Eye Institute were reviewed. Patients who developed chronic hypotony following Boston type 1 KPro implantation not attributable to anatomic problems (eg, retinal detachment, overfiltering glaucoma tube shunts, tissue necrosis with aqueous leak) or other causes were identified. Demographics and preoperative, intraoperative, and postoperative clinical findings were analyzed. Light microscopic examination of an enucleated globe as well as fibrous retroprosthetic membranes excised at the time of vitrectomy from another patient was performed.
Results
Sixty-eight eyes received KPro implantation over the study period. Six eyes experienced chronic hypotony, with a median time of 18.5 months between KPro implantation and the onset of hypotony. The incidence of chronic hypotony in this series was calculated to be 3.7% at 1 year (95% CI = 0.9%–14.0%) and 13.3% at 2 years (95% CI = 5.5%–30.0%). Of the 6 eyes that developed chronic hypotony, 5 had a previous history of glaucoma or ocular hypertension, but only 3 had a glaucoma drainage implant. All eyes progressing to chronic hypotony were noted to have a retroprosthetic membrane prior to the onset of hypotony. Cox regression modeling demonstrated an increased risk of chronic hypotony in eyes with retroprosthetic membranes ( P < .01) but no increase in risk for older patients ( P > .1), eyes with glaucoma drainage implants ( P > .5), or a previous history of multiple donor corneal transplants ( P > .5).
Conclusion
Chronic hypotony can be a significant complication of KPro implantation and should be assessed carefully in eyes with retroprosthetic membranes. Further study of an association between hypotony and retroprosthetic membrane formation may be useful to gain insight into the mechanism of this complication and potential prevention or treatment options.
Donor corneal transplantation is a commonly used surgical technique with great success for treating corneal blindness. However, eyes with corneal vascularization, significant limbal stem cell deficiency, or multiple previous graft rejections have high failure rates. Those eyes may be candidates for artificial corneal surgery.
The Boston type 1 keratoprosthesis (KPro) is one of the most commonly used artificial corneal devices worldwide. Because of the refinement of technical approaches and postoperative management, there has been a marked decrease in the occurrence of various postoperative complications such as endophthalmitis and device extrusion. This has spurred a substantial increase in the number of KPro procedures performed in recent years, with more than 6000 devices implanted worldwide thus far.
Nevertheless, KPro is not free of complications; patients with KPro implantations require vigilant follow-up. Several previous case series have established the formation of retroprosthetic membranes (RPM) and elevated intraocular pressure to be among the most common complications. Previous studies also reported infrequent cases of hypotony largely secondary to glaucoma tube shunt problems, retinal detachment, tissue necrosis with aqueous leak, and other anatomical causes.
Herein, we report the occurrence of chronic hypotony not related to anatomical problems in a series of patients who underwent KPro implantation. We summarize the clinical and histopathologic findings and evaluate the putative risk factors for its occurrence.
Methods
After receiving approval from the Johns Hopkins University Institutional Review Board to retrospectively review patient medical records for the purpose of this publication, electronic and paper records were obtained for all patients who underwent KPro implantation at the Wilmer Eye Institute between January 1, 2004 and November 30, 2010. Pediatric patients were excluded from this review.
All surgeries were performed by a single surgeon (E.K.A.) in a somewhat uniform manner. All patients had a diagnosis of corneal opacification or disease secondary to previous multiple immunologic graft rejections, acquired or congenital limbal stem cell deficiency, or other conditions with poor likelihood of donor corneal graft survival, necessitating KPro for visual rehabilitation. In all cases, a Boston type 1 KPro with the perforated backplate had been implanted. A soft bandage contact lens (Kontur Contact Lens Co, Hercules, California, USA) was inserted at the end of the surgery in all cases. A fluoroquinolone antibiotic and prednisolone 1% topical drop were given to all patients for postoperative use. Patients with inflammatory ocular surface diseases and significant dry eye were also placed on vancomycin eye drops 14 mg/mL 4 times daily.
Medical records were reviewed retrospectively with regard to demographics, preoperative diagnoses, comorbid conditions, postoperative complications, management strategies, and outcomes. All data were abstracted onto standardized data collection forms and entered into a database for analysis. Putative risk factors for hypotony were evaluated in Cox regression analyses performed in STATA 11 (StataCorp, College Station, Texas, USA). Histopathologic findings of tissues obtained from 2 patients were reviewed in detail by an ophthalmic pathologist (C.G.E.).
Results
Sixty-eight eyes of 68 adult patients who underwent Boston type 1 KPro implantation were identified. The most common preoperative indication for the surgery was multiple donor graft failures from immunologic rejection (average 1.7). One patient was excluded because of lack of follow-up beyond the immediate postoperative period. The median follow-up for the remaining patients (n = 67) was 16.9 months (interquartile range = 6.9–26.7 months).
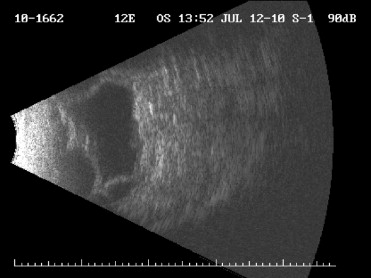
A total of 7 patients were identified as having hypotony following KPro surgery. Hypotony was identified when a lower than usual eye pressure was detected at more than 1 visit by digital palpation. In all cases, B-scan sonogram demonstrated a small globe with irregular contour of the globe wall and diffuse thickening of the posterior ocular coats ( Figure 1 ) . Choroidal detachments and/or scleral folds upon exertion of pressure with the sonogram probe were also noted in some cases. Ultrasound biomicroscopy was not performed. Hypotony occurred shortly after application of a diode laser in 1 eye with 2 prior glaucoma tube shunts. This was determined to be a case of acute hypotony, leaving 6 eyes with chronic hypotony.
Demographics and clinical features of the 6 patients who developed chronic hypotony are summarized in Tables 1 and 2 . No case had an evident cause to explain the hypotony, such as corneal melt with aqueous leak or retinal detachment. On average, the time period between KPro implantation to the development of hypotony was 18.5 months. All patients developing chronic hypotony complained of a progressive decrease in visual acuity in the affected eye and were noted to have RPMs. Three of the 6 eyes with chronic hypotony had glaucoma tube shunts inserted 3 to 100 months prior to KPro implantation. Overall, 35 eyes in the entire series (35/67, 52%) had 1 or more glaucoma drainage implants, including 15 eyes with Ahmed valves, 20 with Baerveldt implants, 1 with a Molteno implant, 1 with a Krupin valve, and 4 implants of unknown design. Comparable to the 49 of 61 KPro patients without hypotony (80%), 5 of 6 patients with hypotony had a previous donor corneal transplantation prior to KPro implantation. The median number of donor corneal transplants performed in patients with hypotony was 2. One eye with hypotony (Patient 3) underwent primary KPro implantation because of severe corneal and conjunctival scarring in the setting of trachoma.
| Patient # | Age | Sex | Pre-op VA (in Affected Eye) | Pre-op IOP (in Affected Eye) (mm Hg) | Diagnosis | Prior PKs | Comorbid Conditions |
|---|---|---|---|---|---|---|---|
| 1 | 56 | Male | CF | 17 | Aniridia | 2 | Glaucoma, aphakia |
| 2 | 61 | Male | CF | 13 | Keratoconus | 3 | Glaucoma, pseudophakia (stable) |
| 3 | 69 | Female | HM | 7 | Trachoma | 0 | Cataract |
| 4 | 67 | Male | 20/320 | 14 | Aniridia | 1 | Glaucoma, aphakia |
| 5 | 32 | Female | HM | 17 | Aniridia | 1 | Glaucoma, pseudophakia (subluxated) |
| 6 | 37 | Male | 20/250 | 18 | Aniridia | 2 | Glaucoma, aphakia |
| Patient # | Simultaneous Procedures at the Time of KPro | Type of Glaucoma Tube Shunt (n) | Follow-up (mo) | Best VA After KPro | Time From KPro to Hypotony a (mo) | Intervention | VA at Last Examination |
|---|---|---|---|---|---|---|---|
| 1 | None | None | 53.3 | 20/160 | 24 | PPV+SO | 20/400 |
| 2 | None | None | 54.2 | 4/200 | 12 | Pre-phthisical | HM |
| 3 | Cataract removal without IOL implantation | None | 28.3 | 6/200 | 27 | PPV+SO | HM |
| 4 | None | Baerveldt (1) | 55.7 | 20/250 | 24 | PPV+SO | HM |
| 5 | Explantation of IOL, anterior vitrectomy | Baerveldt (1) | 47.3 | 20/400 | 17 | Enucleation | NLP |
| 6 | None | Ahmed (1) | 11.5 | 20/100 | 7 | PPV+SO | 8/300 |
a Time period between the implantation of Boston type 1 keratoprosthesis and development of hypotony.
Proportional hazard estimates could not be obtained from models including the presence of RPM as a covariate given the absence of failures in patients without RPM. Cox regression analysis demonstrated significantly greater risk of developing chronic hypotony in patients with RPM ( P < .01). No increased risk of chronic hypotony was observed with increasing age, multiple (2 or more) prior corneal transplants, presence of any glaucoma drainage implant, or presence of an unvalved glaucoma drainage implant ( P > .12 for all).
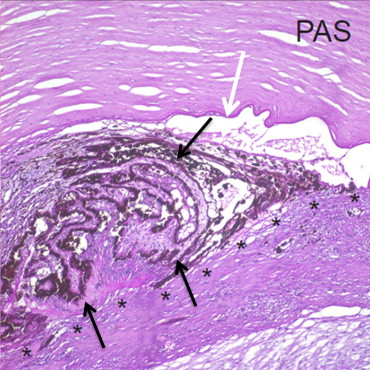
Intraoperative and postoperative findings and final outcomes are summarized in Table 2 . Ligation of the tube was recommended in 3 of the chronic hypotony patients who had a glaucoma tube shunt in situ. The tube shunt was sutured ab externo in 2 patients, albeit without any improvement in the low intraocular pressures, suggesting that overfiltration was not the cause of chronic hypotony. One patient (Patient 5) with a tube shunt deferred any intervention, and the eye progressed to phthisis bulbi, requiring enucleation. Pathologic examination revealed diffuse stromal scarring and neovascularization in the remaining native cornea. The anterior chamber appeared collapsed with a thick retrocorneal fibrocellular membrane tightly entrapping the ciliary body and atrophic iris, which were both displaced anteriorly ( Figure 2 ) . The retrocorneal and cyclitic fibrous membranes contained foci of chronic inflammation and foreign body reaction. The retina was detached in a funnel-shaped configuration and showed atrophy, gliosis, and hemosiderin deposition.