19
Cholesterol Granuloma
Cholesterol granuloma of the petrous apex, also called cholesterol cyst, is grossly an expansile cyst that contains yellow-brown viscous debris laden with cholesterol crystals. Microscopically, the cyst contains areas of cholesterol surrounded by chronic inflammatory cells, foreign body giant cells, fibrosis, and blood vessels. The lining is fibrous. The pathogenesis includes obstruction of drainage in a normally aerated space, subsequent hemorrhage, blood breakdown, and release of cholesterol. A granulomatous foreign body reaction triggers fibrous encapsulation of cholesterol. Cholesterol granuloma can occur in any air space of the temporal bone, most commonly in the mastoid. In the petrous apex, cholesterol granuloma is the most common cystic lesion, six times more common than cholesteatoma and 20 times more common than mucocele.1 Small lesions tend to be clinically silent and are occasionally found incidentally. With gradual expansion, the lesion eventually encroaches on neural structures, resulting in hearing loss, dizziness, facial weakness, and possibly facial numbness. Critical elements of the management of these lesions include recognizing and differentiating cholesterol granuloma from other abnormalities in the petrous apex, determining when to intervene, and providing safe, long-term drainage.
■ Clinical Presentation
When patients present with symptoms referable to the petrous apex, a complete review of symptoms and physical exam is important, with specific attention to the cranial nerves, hearing, and balance. In our patients, hearing loss (65%), dizziness (56%), and tinnitus (50%) are the most common symptoms. The majority of patients have multiple symptoms. Headache is a complaint in 32% of patients. Other cranial nerve deficits such as facial twitching or weakness (26%), facial paresthesia (20%), and diplopia (6%) may occur.2 Lesions of the petrous apex may be diagnosed as incidental findings on computed tomography (CT) or magnetic resonance imaging (MRI) done to evaluate sinus disease or head trauma or for unrelated purposes. In these cases, again, a directed history and exam to elicit symptoms related to the petrous apex are necessary.
■ Making the Diagnosis
Both MRI and CT play a role in the diagnosis and management of petrous apex cholesterol granuloma. The diagnosis is made based on MRI characterization of the contents of the cystic lesion and differentiation among epidermoid cyst, giant carotid aneurysm, and other petrous lesions. MRI and CT are complementary in differentiating cystic lesions (cholesterol granuloma, primary cholesteatoma, and mucocele), solid lesions, and nonpathological radiographic anomalies of the petrous apex (Table 19) Distinguishing cholesterol granuloma from cholesteatoma (which requires complete excision or exteriorization) and solid lesions (which require biopsy and possible complete excision) is critical in the successful management of lesions in this area. CT is done to assist with treatment planning. The location of the cyst relative to air cell tracts and neurovascular structures and potential drainage pathways are defined by CT prior to surgical intervention.
Cystic Lesions |
Cholesterol granuloma |
Cholesteatoma |
Mucocele |
Solid Lesions |
Chordoma |
Chondrosarcoma |
Metastatic tumor |
Lipoma |
Giant cell tumor |
Meningioma |
Carotid artery aneurysm |
Dermoid/teratoma |
Radiographic Anomalies |
Retained secretions |
Asymmetric pneumatization |
On CT, cholesterol granuloma is an expansile, cystic lesion with well-defined, smooth margins. It is isodense with brain and nonenhancing, although the capsule may enhance (Fig. 19–1)On MRI, it is the only lesion that is hyperintense on both T1-weighted images (T1WI) and T2WI, and does not enhance with gadolinium (Fig. 19–2). The cyst may contain hypointense debris on T2WI. Generally, the signal is homogeneous, but hemosiderin and ferritin released during breakdown of blood may give a more heterogeneous appearance on T2WI.3
Cholesteatoma also has a smooth bony margin on CT scan, but in some cases, bone erosion results in a more irregular edge. Because of high water content, cholesteatomas are isointense with cerebrospinal fluid (CSF) on CT and hypointense on T1WI and hyperintense on T2WI MRI images. MRI is the best study to differentiate cholesterol granuloma from cholesteatoma. Table 19–2 provides tips on correctly diagnosing cholesterol granuloma radiographically.
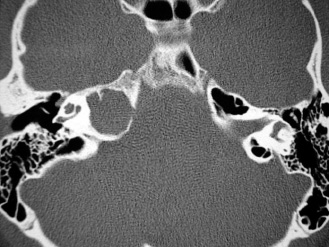
FIGURE 19-1 Axial computed tomographic image of right petrous apex cholesterol granuloma. The cyst is located posterior to the horizontal carotid canal. The margins are sharp and smooth. The temporal bone is well aerated, with moderate pneumatization of the contralateral petrous apex. The cyst is isodense to brain.
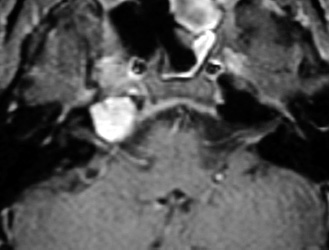
FIGURE 19-2 Axial T1-weighted magnetic resonance image.
Obstruction of petrous air cells may result in retained secretions or an expansile mucocele. On CT, retained secretions of the petrous apex are isodense to CSF, have smooth bony margins, and do not enhance with contrast. Retained secretions in petrous apex air cells display similar MRI characteristics but are limited to normal-appearing air cell spaces without CT evidence of bony remodeling. Mucoceles are hypointense on T1WI and hyperintense on T2WI, and on CT they are isodense to CSF and have smooth expansile borders.
Solid lesions of the petrous apex, such as chordomas, metastatic tumors, chondrosarcomas, and lipomas, will display a variety of MRI characteristics and will show aggressive bone destruction on CT, making them relatively easy to distinguish from cholesterol granuloma.
High fat content in the petrous apex bone marrow produces a hyperintense signal on T1WI and hypointense signal on T2WI MRI. When there is significant asymmetry of the pneumatization of the petrous apex, confusion may arise, and a cyst may be misdiagnosed in the nonpneumatized side. This common radiographic finding can be recognized, however, by noting the lack of bone erosion or expansion and the reduction of signal on fat-suppressed MRI images (Table 19–3).
■ Patient Counseling
Once a petrous apex lesion is diagnosed, the decision for surgical intervention is made. Clearly, surgery is indicated for symptomatic or growing lesions. The growth rate of cholesterol granuloma is unknown, but significant growth may be suspected based on large size or expansile margins. Lesions encroaching on the internal auditory canal (IAC) or other neurovascular structures, even if asymptomatic, are candidates for surgery in the healthy patient. Delay of surgery offers no advantage.
Problem | Prevention/Treatment |
|---|---|
Diagnosis | |
Cholesterol granuloma | CT showing expansile mass with no bone erosion |
MRI showing hyperintense mass on T1WI and T2WI | |
Cholesteatoma | CT may show some bony erosion |
MRI shows hyperintense mass on T2WI and hypointense mass on T1WI |



