Choanal Atresia and Anterior Nasal Stenosis
Choanal atresia is an incomplete opening between the posterior nasal cavity and the nasopharynx. This condition may be unilateral or bilateral. Unilateral choanal atresia usually presents with chronic unilateral rhinorrhea; however, it causes little or no respiratory distress.
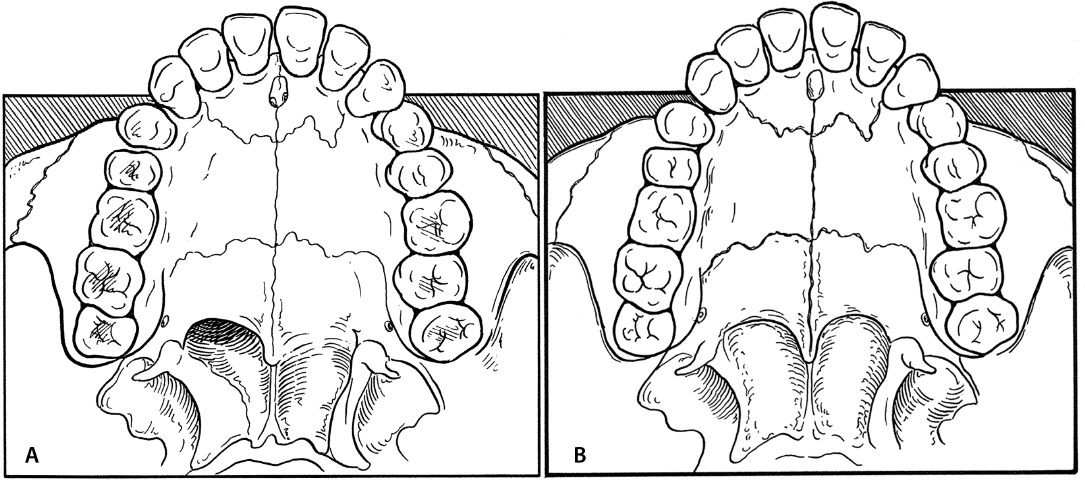
Because neonates are obligate nasal breathers, bilateral atresia causes severe respiratory distress (Fig. 14.1a,b). When neonates cry, they open their mouths to breathe and the distress subsides. The initial distress can be managed with a McGovern nipple (large nipple with cross-cuts in the end) to open the mouth and displace the tongue inferiorly to permit oral breathing. An orogastric tube is often necessary to supply adequate nutrition until the repair is completed.
14-1 Transnasal Repair of Choanal Atresia
Indications
Repair of choanal atresia is necessary to provide an adequate airway.
Preoperative Evaluation
A computed tomography (CT) scan is essential to define the shape of the nasal chambers and to determine both the level of the skull base and whether the atresia is membranous or bony. The scan must be perpendicular to the plane of the hard palate. Bony atretic plates less than 3 mm in thickness are amenable to a transnasal approach.
Operative Technique
1. Transnasal repair is performed under general anesthesia. Orotracheal intubation with an oral RAE tube facilitates access to the nasopharynx.
2. Afrin-soaked neurosurgical patties are placed into the nasal vault for vasoconstriction.
3. A Crowe-Davis mouth gag is used to expose the oropharynx and provide access to the nasopharynx (Fig. 14.1c). The choanae can be visualized with a 120-degree telescope, retracting the soft palate and viewing the posterior choanae from behind. A 0-degree telescope is passed transnasally to view the posterior choanae and other nasal anatomy.
4. Under continual visualization with a 120-degree telescope in the nasopharynx, a urethral sound can be passed along the floor of the nose and used to puncture the atretic plate. This works well for stenoses that contain a membranous component (Fig. 14.1d).
For thick atretic plates, an endoscopic drill is used with visualization provided by a 0-degree telescope. The atretic plate can be visualized, and the drill is used to open the atretic plate medially along the floor of the nose. Direct visualization is required to remain oriented (Fig. 14.1e).
5. After the atretic plate is opened, visualization is maintained with the 120-degree endoscope. A backbiting instrument is used to remove a portion of the posterior septum (Fig. 14.1f). Drills can be used to open the choanae laterally, taking care not to violate the sphenopalatine artery (Fig. 14.1g).
6. Nasal stenting is controversial. If used, it should be for less than 3 weeks. Suction catheters are passed through the nose on each side and pulled out of the mouth (Fig. 14.1h). A size-appropriate endotracheal tube stent is chosen and the stent is folded in half at the area of flexion (Fig. 14.1i). Three-quarters of the endotracheal tube is removed to create two patent tubes connected to each other by the remnant of the endotracheal tube wall (Fig. 14.1i). Next, the suction catheters are sutured to the ends of the newly fashioned stent to allow it to be pulled retrograde into position in the choanae, exiting the nasal vestibule (Fig. 14.1j). The endotracheal tube stents are then cut in such a way that they extend beyond the columella. A section of the discarded endotracheal tube is fashioned as a connecting strut that will be sutured between the two stents coming through the nasal vestibule (Fig. 14.1k). This creates a complete loop of the stent, preventing it from being pulled out of and pushed into the nasopharynx. Suction catheters are then measured to determine the length needed to keep the stents open. The suction catheter should extend beyond the tip of the stent into the nasopharynx by 5 mm. Suctioning should occur every 8 hours and as needed.
Complications
Restenosis