Chlamydiae have long been important causes of ocular infections and are still the second leading cause of blindness in Africa (1,2). Trachoma is one of the oldest recorded diseases of mankind, documented in the Egyptian Eber’s papyrus in 1900 BC (2,3). It is still endemic in sub-Saharan Africa, including Ghana, Mali, and Tanzania, as well as eastern Mediterranean countries such as Iraq, Saudi Arabia, United Arab Emirates, Qatar, and Oman (1,2,4,5). According to the World Health Organization (WHO) there are 146 million people worldwide with active trachoma (2). It is one of the greatest single causes of preventable blindness and impaired vision in the world today (6). Western Europe and the United States have been trachoma free in the last century, correlating with economic development, and in Southeast Asia progress is being made for the same reason (4). Transmission of the chlamydial agent causing trachoma is by eye-to-eye or hand-to-eye contact. The disease is usually acquired in early childhood. Chronic inflammation from recurrent infections leads to conjunctival scarring and blinding complications in adults. A number of environmental factors such as low living standard and poor hygiene, influence prevalence and severity of trachoma.
The second ocular disease caused by Chlamydia trachomatis is adult inclusion conjunctivitis, also called paratrachoma. Reported prevalences range from zero to 28% (7, 8, 9, 10), but population selection biases, the absence of controls, and differing diagnostic assays used in these studies explain the wide range of results. Adult inclusion conjunctivitis typically occurs in sexually active young adults following transfer of bacteria from the genitalia to the eye. There is a high incidence of cervical or urethral chlamydia in these individuals (9, 10, 11).
With the advent of widespread neonatal ocular prophylaxis, gonococcal infections have decreased and C. trachomatis is now the most common cause of ophthalmia neonatorum in industrialized countries as well as in several developing countries (12, 13, 14, 15). It may be responsible for 20% to 73% of all cases of neonatal conjunctivitis (16, 17, 18). In developing countries the prevalence of genital chlamydial infection in pregnant women ranges from 7% to 29%. One third of infants exposed at birth will develop chlamydial disease (2,14). In North America and Europe, 2% to 6% of all newborns are infected with neonatal chlamydiae (19). However, the incidence of C. trachomatis conjunctivitis is declining, as shown in Argentina with 4.39/1,000 live births in 1995 down to 0.78/1000 live births in 1998 (2).
EPIDEMIOLOGY
Trachoma
Although trachoma has been declining in many areas of the world, estimates suggest that approximately 2.2 million people are blind from trachoma in Africa (1) and trachoma is responsible for 6 million blinded people or 15% of world’s blindness. In some areas trachoma is holoendemic—every child acquires active trachoma and every adult shows evidence of conjunctival scarring. Corneal opacification from trachoma was found to be responsible for 20.6% of all blindness in Jimma zone, Ethiopia (22) and for 4.5% of blind individuals in the Central African Republic (23). Investigations in highly endemic sub-Saharan Africa have shown that women account for about 75% of all trachomatous trichiasis and subsequent blindness due to corneal scarring (1). A survey in Saudi Arabia revealed that over 3.5% of the population showed corneal scars, about half of them due to trachoma (5). However, trachoma is extremely variable, and a high incidence of trachoma in an area may not necessarily be correlated with a high degree of visual impairment (2). The duration of disease and infection is markedly age-dependent. The estimated median duration of disease was 13.2 weeks in 0- to 4-year-old subjects and 1.7 weeks in those age 15 and over in a study by Bailey et al. (24). The cumulative incidence rate of disease was reduced threefold, with age mostly attributable to a more rapid disease resolution.
The risk of acquiring C. trachomatis is strongly linked with environmental and behavioral characteristics. Numerous studies have demonstrated that limited access to water supplies, low water consumption by the household, the presence of flies, and poor hygiene are all risk factors for becoming infected with C. trachomatis (25). The infection is usually transmitted by ocular secretions from contaminated fingers, clothes, and aerosolized nasopharyngeal secretions (26). The basic pattern is mother-to-child transfer. The higher incidence of acute disease and blindness in women may be explained by their lower status in society, their permanent close contact with children and common applicators used to apply eye makeup (1,2). Face flies are found commonly in seasons with the highest prevalence of active trachoma and are believed to feed on ocular discharges, but it has been difficult to quantify the role of flies in transmission. Reducing fly densities in rural African villages, however, has been demonstrated to reduce active disease (27) as has the introduction of face washing (28). Although malnutrition is common in hyperendemic areas, no relationship was found between nutritional status and trachoma in preschool children (29).
Coinfection with other bacteria occurs often and may facilitate transmission and proliferation of chlamydia. Moreover, bacterial conjunctivitis may cause disastrous sequelae in eyes already infected with trachoma, and bacterial infection may play a greater role than trachoma in producing blinding complications (30).
Adult Inclusion Conjunctivitis
Chlamydia was the causative organism in 2% of patients with acute conjunctivitis in a study performed in Australia (9). A distinctive feature was the long delay before a definitive diagnosis of ocular chlamydial infection was made.
Inclusion conjunctivitis is an oculogenital disease and as such, its epidemiology differs dramatically from that of trachoma. It was originally described in Europe as “swimming pool conjunctivitis,” contracted from swimming in contaminated pools (31). Today proper chlorination has eliminated chlamydiae from this source, but nongenital infection may occur with bathing in unchlorinated water (9). Adult inclusion conjunctivitis is usually transmitted by autoinoculation from genital secretions or by genital-to-eye-inoculation by an infected sexual partner. At present, a minimum of 70% of women (and possibly all) with chlamydial conjunctivitis are estimated to have genital C. trachomatis infection, which is mostly asymptomatic. Chronic disease of the female genital tract may produce pelvic inflammatory disease, tubal blockage, ectopic pregnancy, and infertility (9,32,33). Also 54% of men with chlamydial conjunctivitis had a positive chlamydial urethral culture, and 70% of these patients had no genital symptoms (34). Up to 32% of men and 63% of women with genital Neisseria gonorrhoeae have coexistent chlamydial infections, and it has been suggested that N. gonorrhoeae can activate latent Chlamydia (35). Eye-to-eye transmission is possible, but extremely rare (9).
Neonatal Inclusion Blennorrhea
Intrapartum transmission of neonatal chlamydial ocular infection from the mother’s genital tract was first described by Halberstaedter and von Prowazek (36) in 1909. Characteristic inclusion bodies were found in specimens from eyes of infected newborns as well as from the cervices of their mothers. Subsequently, Lindner (37) demonstrated infectious agents in urethral swabs from fathers of infants with neonatal inclusion conjunctivitis. Without prophylaxis, the transmission rate from an infected mother to her infant is approximately 50%, with the risk of development of conjunctivitis being 30% to 40% for infected babies (38). Although infection is thought to typically occur as the fetus passes through an infected birth canal, a study suggests bacterial transmission to infants’ eyes from their nasopharyngeal passages or those of their caregivers after birth (39). Moreover, a transmembrane or transplacental route of infection may be involved in early chlamydial infections in infants delivered by cesarean section (40).
CLINICAL FEATURES
Trachoma
The initial infection of trachoma is characterized by an abrupt nonspecific conjunctivitis, followed by follicle formation at about the third week (Fig. 18-1). The symptoms appear within 5 to 7 days postinoculation. A purulent discharge consisting of mixed inflammatory cells may develop, along with a tender preauricular lymph node. Conjunctival follicles grow, and peripheral corneal follicles as well as a marked trachomatous pannus develop. Later, large papillae may mask the typical gelatinous follicles. Resolving limbal follicles leave typical Herbert’s peripheral pits (Fig. 18-2). Cicatricial changes of the conjunctiva and the underlying tarsus lead to entropion formation and trichiasis. Often a heavy linear scar parallel with and 1 to 2 mm from the lid margin extends across the entire lid (Arlt’s line, Fig. 18-3) (41). Untreated lid deformities and added superinfection may progress to corneal complications and severe visual loss. Whereas in early disease epiphora dominates, advanced disease may cause severe keratoconjunctivitis sicca due to atrophy of meibomian glands, loss of mucus-secreting cells, and occlusion of the tear lacrimal ducts (42,43). Lacrimal system complications observed in severe, inactive disease include dacryocystitis, dacryocystocele, and dacryocutaneous fistula (43).
FIGURE 18-1. Follicular conjunctivitis in trachoma.(see color image)
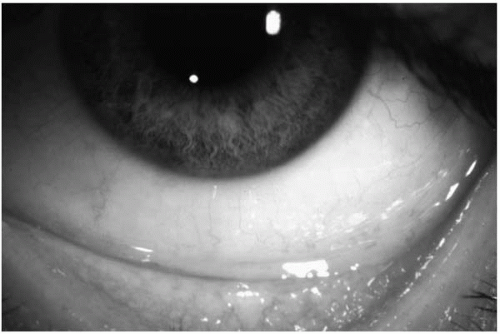
FIGURE 18-2. Peripheral Herbert pits after resolution of limbal follicles in trachoma.
Two classification schemes are used to categorize the stages of trachoma, the MacCallan system dating back to 1908, and that of the WHO (44,45). MacCallan (44) divided the course of trachoma into four stages, based on developmental changes in the follicles, papillary hypertrophy, and scar formation (Table 18-1). His classification is useful for epidemiologic studies, but it neglects the intensity of the inflammatory reaction in chlamydial disease. The WHO uses a simple grading scheme for clinical assessment of ocular trachoma (Table 18-2) (45). Trachoma is divided into two inflammatory stages (follicular inflammation, TF; trachomatous inflammation intense, TI) and three stages associated with scarring (trachomatous scarring, TS; trachomatous trichiasis, TT; corneal opacity, CO). This classification system demonstrated high interobserver reliability in trachoma studies.
TABLE 18-1. STAGES OF TRACHOMA, ACCORDING TO MACCALLAN, 1931
Stage I
Early stage of follicles
Stage IIa
Large and gelatinous follicles
Stage IIb′
Papillary enlargement as well as follicles
Stage IIb″
Follicles with the added complication of spring catarrh
Stage IIc
Trachoma complicated by gonococcal conjunctivitis
Stage III
Cicatrization has commenced
Stage IV
Cicatrization is complete
Adult Inclusion Conjunctivitis
Symptoms of adult inclusion conjunctivitis, such as redness, foreign-body sensation, photophobia, and mucopurulent discharge, typically begin 2 days to 3 weeks after inoculation (19). Examination reveals a follicular conjunctivitis, mainly localized to the inferior tarsal conjunctiva, associated with papillary hypertrophy (Figs. 18-4 and 18-5). Usually, the infection is bilateral, but Garland et al. (9) reported monocular inclusion conjunctivitis in the majority of their patients. Nontender lymphadenopathy of the ipsilateral preauricular nodes may also be present. Corneal complications include a superficial punctate keratitis as well as pannus formation. This superficial micropannus, however, is distinct from the severe macropannus developing in trachoma. Marginal and central subepithelial infiltrates as well as epidemic keratoconjunctivitis-like subepithelial lesions may occur (19,46,47). If adult inclusion conjunctivitis is left untreated, it usually heals spontaneously but may persist for longer than a year. Few cases will lead to conjunctival or corneal scarring. Coinfection with adenovirus is rare but must be suspected in prolonged follicular keratoconjunctivitis (48). Anterior uveitis may complicate inclusion conjunctivitis. Moreover, antibodies to C. trachomatis are significantly increased in acute anterior uveitis compared to healthy controls or other forms of uveitis (49). A common genetic predisposition to Chlamydia infection and acute anterior uveitis in the context of human leukocyte antigen (HLA)-B27-positivity may be responsible for this phenomenon. Reactive arthritis occurs in approximately 2% to 4% of patients after previous infections mainly of the urogenital tract with C. trachomatis or of the gut with enterobacteriae (50). Although HLA-B27 is found in only approximately 50% of patients with acute reactive arthritis, HLA-B27 seems to be crucials for the development of sacroiliitis and chronic spondyloarthropathy (50).
TABLE 18-2. STAGES OF TRACHOMA ACCORDING TO THE WHO, 1987
Clinical Findings
WHO Grade
Code
≥5 follicles in the upper tarsal conjunctiva; Follicles must be ≥0.05 mm in diameter
trachomatous inflammation follicular
TF
Pronounced inflammatory thickening of the tarsal conjunctiva which obscures half of the normal deep tarsal vessels
trachomatous inflammation intense
TI
Presence of easily visible scars in the tarsal Conjunctiva
trachomatous Conjunctival scarring
TS
At least one eyelash rubs against the eyeball; also includes evidence of recent removal of an in-turned lash
trachomatous trichiasis
TT
Easily visible corneal opacity present over the Pupil that is so dense that at least part of the pupil margin is blurred when seen through the opacity
corneal opacity
CO
Twelve of 84 infected volunteers (14%) developed symptoms of otitis media in experimental inclusion conjunctivitis (47). C. trachomatis was cultured from the middle ear aspirates of patients with acute otitis media with and without effusion and chronic otitis media (51). In animal experiments otitis could be induced by direct inoculation into the middle ear as well as indirectly by infection of the nasopharynx and the conjunctiva (51,52).
Neonatal Inclusion Blennorrhea
Symptoms of neonatal inclusion conjunctivitis appear 5 to 12 days postpartum (earlier with premature rupture of amniotic membranes). Acute infection typically presents with binocular lid edema, conjunctival hyperemia, papillary hypertrophy, and copious mucopurulent discharge (Fig. 18-6). A follicular reaction, indicating the formation of secondary germinal centers, cannot be established in newborns before 6 to 8 weeks, but may develop in chronic disease. It may be extremely difficult to differentiate between chlamydial and other bacterial causes of conjunctivitis on the basis of physical examination. Moreover, more than one organism was isolated from the conjunctiva in 50% of cases with chlamydial conjunctivitis (17). Age of presentation, however, is about 1 week later in infants with other bacterial infections compared to Chlamydia (17).
FIGURE 18-4. Adult inclusion conjunctivitis. Follicular conjunctivitis localized to the inferior tarsal conjunctiva(see color image)
Corneal manifestations similar to those of adult inclusion conjunctivitis such as superficial punctate keratopathy, fine micropannus, and peripheral subepithelial infiltrates have been described in newborns. Conjunctival and corneal scarring are possible sequelae (53). Untreated, neonatal inclusion blennorrhea may pursue a prolonged course with systemic involvement. A high incidence of pharyngeal infection is found in babies with isolation-positive chlamydial conjunctivitis. Lower respiratory tract infections, including pneumonitis, otitis media, proctitis, and vulvovaginitis, may complicate neonatal ocular disease (38,54).
PATHOGENESIS, PATHOLOGY, AND IMMUNOLOGY
Chlamydia are unique among bacteria in that they are obligate intracellular gram-negative organisms with a complex intracellular development cycle that consists of an infectious metabolically inactive elementary body and a noninfectious, metabolically active reticulate body. They are unable to produce adenosine triphosphate and thus are energy parasites (55). Because of their singular biologic character, the chlamydiae are assigned their own order, the Chlamydiales, consisting in turn of one family, the Chlamydiaceae, two genera, the Chlamydia and the Chlamydophila, and nine species. Human chlamydial infection is often caused by Chlamydia trachomatis, less frequently by Chlamydophila pneumoniae, and rarely by Chlamydophila psittaci, Chlamydophila abortus, or Chlamydophila felis (56). C. trachomatis isolates are commonly classified into 15 distinct serovars, designated A-K, L1-L3, and MoPn, which is a mouse adapted strain. Serovars A-C cause trachoma, serovars D-K (and occasionally, variants of B or Ba) are primarily associated with sexually transmitted infections, and serovars L1-L3 cause lymphogranuloma venereum (57,58). C. trachomatis is essentially a pathogen of mucosal surfaces, infecting and replicating within epithelial cells. The infected cell ruptures, releasing thousands of elementary bodies.
FIGURE 18-5. Adult inclusion conjunctivitis. Follicular conjunctivitis of the upper tarsal conjunctiva.(see color image)
FIGURE 18-6. Neonatal inclusion conjunctivitis with lid edema and copious mucopurulent discharge.
The pathophysiology of chronic chlamydial disease is still unknown in detail, but most likely depends on both parasite and host factors. Recent data provide compelling evidence for a chlamydial cytotoxin for epithelial cells present in the elementary body and delivered to host cells very early during infection. This cytotoxin may also provide a mechanism for immune evasion compatible with the clinical characteristics of persistent oculogenital infections (57). Infection with C. trachomatis leads to the upregulation of several functionally important genes in the host cell such as IL-11, LIF, chemokine gene MIP2a, transcription factor genes, apoptosis-related genes, and adhesion molecule genes such as ICAM-1 (59). Chlamydia seems to reprogram the host cells at various key positions that act as intra- or intercellular switches (59).
Ocular infections are characterized by distinct immunologic and pathologic responses to the different chlamydial strains causing either trachoma or inclusion conjunctivitis. The immune response seems to confer partial protection against subsequent infection, yet appears also to be responsible for much of the observed pathology and tissue destruction seen in trachoma. In trachoma, repeated infection with the causative organism, perhaps exacerbated by superinfection with other organisms, is necessary to cause severe conjunctival scarring and blinding complications. The stimulus for continual inflammation may not be from repeated exposure to chlamydial surface antigens but may rather be due to a labile product released by the living organisms (60). Cellular responses elicited in nonimmune cells (i.e., mucosal epithelial cells) infected by chlamydiae may be necessary and sufficient to account for chronic and intense inflammation and the promotion of cellular proliferation, tissue remodeling, and scarring (61). Inflammatory cells become activated in both an antigen-nonspecific and, for reinfection, an antigen-specific manner to produce their own repertoire of cytokines and growth factors (61).
Both humoral and cell-mediated immune responses are involved. Target antigens are the major outer membrane protein (MOMP) and heat shock proteins (HSP60) (62,63). Antichlamydial antibodies can neutralize chlamydiae and block attachment and internalization of the organism (62). Experimental studies in monkeys and human indicate that tear immunoglobulins, especially immunoglobulin A (IgA), may play a vital role in mediating protective immunity (64,65). But antibodies may limit the extent of chlamydial multiplication and prevent more invasive disease rather than to effect a cure (66). Moreover, antichlamydial antibodies do not protect against reinfection (67,68). Serum IgG antichlamydia antibody was detected in 42% of patients with trachoma and in 37% of patients with acute inclusion conjunctivitis by Numazaki et al. (69). Antichlamydial IgM was present in 13% of patients with trachoma and in 33% of patients with acute inclusion conjunctivitis. Forty percent of the trachoma patients and 34% of patients with inclusion conjunctivitis were IgA-positive. However, antichlamydial IgG and IgA was also present in 25% and 22% of healthy controls, respectively, compared to IgM, which was positive in only 2% of the healthy population (69). IgA antibodies in tears were detected as early as 5 days after onset of clinical symptoms in patients with inclusion conjunctivitis. The IgA response in tears was not significantly correlated with the severity of the ocular infection, whereas serum IgA titers increased with the severity of clinical findings (70, 71, 72). In neonatal inclusion blennorrhea, passively transferred maternal antibodies supposedly do not confer any protection against the transmitted chlamydiae. The detection of IgA antibodies in tears and serum among chlamydia-positive neonates without corresponding maternal antibodies may suggest a production of antichlamydial IgA antibodies in the newborn. The antibody response in serum of newborns with chlamydial conjunctivitis is poor, as would be expected (70, 71, 72).
Only gold members can continue reading. Log In or Register to continue