Chapter 11
CHEMICAL INJURIES: EMERGENCY INTERVENTION

Chemical injuries of the eye may produce extensive damage to the ocular surface and thus lead to visual impairment.1–4 In addition to causing ocular surface injury, alkalies (Fig. 11–1) readily penetrate into the eye, damaging the corneal stroma and endothelium as well as other anterior segment structures (e.g., iris, lens, ciliary body). Most acids (Fig. 11–2) tend to remain confined to the ocular surface. The important agents involved in chemical injuries of the eye are summarized in Table 11–1.2,3
PEARL… Strong acids, such as hydrofluoric acid, may penetrate as readily as alkalies do, producing the same spectrum of ocular injury.2
ETIOLOGY
The most common alkalis causing injury4 are:
• ammonia (NH3; a common ingredient in many household cleaning agents and causing the most serious injury);
• lye (NaOH; a common ingredient in drain cleaners and causing the most serious injury);
• potassium hydroxide (KOH);
• magnesium hydroxide (Mg[OH]2); and
• lime (Ca[OH]2; the most common cause, which fortunately does not inflict as much damage as rapidly penetrating alkalies do).
The most common acids causing injury4 are:
• sulfuric (H2SO4; the most common cause: an ingredient in automobile batteries2);
• sulfurous (H2SO3);
• hydrofluoric (HF; rapidly penetrating and causing the most serious injuries2);
• acetic (CH3COOH);
• chromic (Cr2O3); and
• hydrochloric (HCl).
EPIDEMIOLOGY AND PROGNOSIS
In the USEIR, 3.6% of all serious injuries are chemical burns. In one study5:
• most victims were young (usually between 16 and 25 years of age) and male (76%);
• the most common sites of accidental injury were industrial premises (63%) and the home (33%);
• criminal assault was rather frequent (11%);
• alkali injuries were nearly twice as common as acid injuries; and
• only 8% of patients required hospitalization, and less than 1% suffered severe, permanent visual loss.
In another study6:
• 70% of patients were adult males, 23% were adult females, and 7% were children;
• most patients were between 16 and 45 years of age;
• industrial accidents accounted for 61% of the injuries; 37% were due to household accidents; and
• 88% of the injuries were classified as mild.

FIGURE 11–1 Severe alkali injury. The entire epithelium is either absent or devitalized. Because of stromal and intraocular penetration, the corneal stroma is cloudy, in contrast to the appearance in Figure 11–2. (From Wagoner MD. Chemical injuries of the eye: current concepts in pathophysiology and therapy. Surv Ophthalmol. 1997;41:275–313, Reprinted by permission from Elsevier Science.)
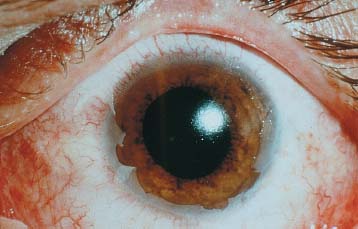
FIGURE 11–2 Acid injury caused by exploding car battery. A 100% epithelial defect is present. Following débridement of necrotic epithelium (some remaining peripherally), the stroma is remarkably clear because of the function of the epithelium as a barrier to acid penetration. (From Mandel ER, Wagoner MD. Atlas of Corneal Disease. Philadelphia: WB Saunders; 1989:71. Reprinted by permission from WB Saunders.)
Although the majority of chemical injuries are without serious sequelae, the prognosis for eyes that present with severe injuries is guarded; in one series,7 only 15% achieved adequate visual recovery.
PATHOPHYSIOLOGY
The severity of ocular injury after chemical exposure is related to:
• surface area of contact;
• depth of penetration; and
• degree of limbal stem cell injury.
Surface Area of Contact
Both alkalies and acids cause the ocular surface epithelial cells to die upon contact. The surface area of contact can be assessed by examination of the fluorescein-staining pattern of the corneal or conjunctival epithelium.
PEARL… It is important to remember that retained particulate matter in the superior fornix (e.g., in case of lime plaster injury) can be a source of continued exposure of the ocular surface to additional damage.
Depth of Penetration
Penetration of alkalies and acids into the corneal stroma may result in keratocyte death and hydration of the ground substance with loss of stromal clarity.8,9 Hydration of collagen fibrils results in thickening and shortening with distortion of the trabecular meshwork and potential increase in IOP.7,8
The time to penetration into the AC varies from almost immediate after ammonia injury to 3 to 5 minutes after sodium hydroxide injury.10,11 Penetration into the AC can result in secondary glaucomaa and cataract.7 Irreversible damage to the ciliary body with hypotony and phthisis may follow prolonged aqueous pH levels above 11.5.11
If the external pH is restored to normal, the aqueous pH levels return to normal within 30 minutes to 3 hours, depending upon the amount of penetration.11
Limbal Stem Cell Injury
PEARL… Following corneal epithelial injury, recovery is dependent upon the most proximal, viable epithelium.12,13
• Complete corneal epithelial injury requires epithelium from the limbus,14–20 where the stem cells of the corneal epithelium reside (see Chapter 32).
• With extensive corneal and limbal epithelial injury, the surrounding conjunctival epithelium provides the only source for epithelial regeneration.21
The clinical course of reepithelialization and its impact upon therapeutic decision making are discussed in Chapter 32.
THERAPEUTIC PRINCIPLES
A modification of our three-step approach to sterile corneal ulceration is applicable for treating the chemically injured eye from the outset.22,23
Step 1: Promote ocular surface epithelial recovery with proper phenotypic transdifferentiation.
PEARL… The recovery of an intact and phenotypically normal corneal epithelium is the most important determinant of a favorable outcome following chemical injury.
• Débridement of necrotic epithelium (Fig. 11–2) allows subsequent migration of adjacent viable epithelium into the denuded area.
• Nonpreserved topical lubricants may facilitate reepi-thelialization in older patients with aqueous tear deficiency. In young patients with adequate tear production, tear supplementation is not necessary.
• Pressure patching and/or bandage soft contact lens
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


