Purpose
To describe the anatomic characteristics of structures adjacent to the lacrimal sac fossa and the standardized osteotomy method for endonasal dacryocystorhinostomy in Asians.
Design
Retrospective noncomparative observational case series study.
Materials and Methods
One hundred fifty-two eyes of 76 patients who had normal orbit computed tomographic scans were enrolled. The relationships of the uncinate process, the operculum of the middle turbinate, and the agger nasi cell to the lacrimal sac fossa were analyzed. Bone thickness and proportion of the frontal process of the maxilla in the lacrimal sac fossa was also evaluated.
Results
The uncinate process was attached to the lacrimal sac fossa in 152 cases (100%) at the lower level of the fossa. The operculum of the middle turbinate was attached to the lacrimal sac fossa in 142 cases (93.4%), with wide positional variation. The agger nasi cell was adjacent to the lacrimal sac fossa in 118 cases (77.6%). The descent of the operculum of the middle turbinate relative to the lacrimal fossa had a strong correlation with the descent of the agger nasi cell ( P < .001). The height and length of the nasal bone had a significant negative correlation with the thickness of the frontal process of the maxillary bone ( P < .001).
Conclusion
The uncinate process, operculum of the middle turbinate, and agger nasi cell should be removed for sufficient osteotomy in a significant portion of Asian patients during dacryocystorhinostomy. A thick frontal process of the maxilla can be anticipated for the patient with a low nasal bridge. Further studies on the variation in intranasal procedures and the success rate of endonasal dacryocystorhinostomy need to be established.
External dacryocystorhinostomy (DCR) is a standard approach for treatment of complete nasolacrimal duct obstruction. Endonasal DCR has regained popularity with the application of new technology and instrumentation. The approach may obviate a cutaneous incision and possible lacrimal pump influence in external DCR.
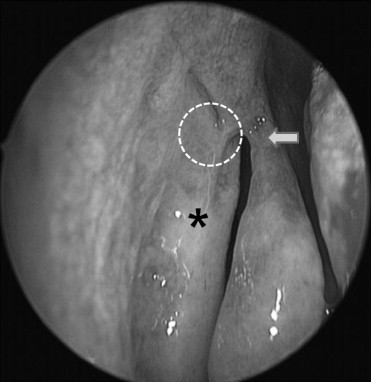
Endonasal DCR is still perceived to be more complicated and challenging than external DCR in terms of intraoperative orientation. The approach from the nasal cavity to the lacrimal sac in endonasal DCR is more complex than the conventional technique in external DCR ( Figure 1 ). An adequately sized and correctly located osteotomy is essential to an efficient anastomosis of the lacrimal and nasal mucosa, which is also important for the long-term patency of the nasolacrimal shunt. Therefore, optimizing surgical procedures for endonasal DCR is based only on a comprehensive understanding of the structural relationships and their variations, which precludes unnecessary mucosal and structural violation and ensures a good surgical outcome.
The uncinate process is a thin bony structure that is continuous with the ethmoid bone anteriorly and may attach to the lamina papyracea, skull base, or middle turbinate superiorly. Uncinectomy is an important surgical step to expose the natural ostium of the maxillary sinus in endoscopic sinus surgery. The anterior part of the uncinate process faces the lacrimal sac fossa; however, the relationship with the lacrimal apparatus has only recently been reported. A few independent surgical studies have reported that the uncinate process may actually overlap the lacrimal sac fossa and must be removed to access the lacrimal sac fossa. In performing endonasal DCR, the uncinate process can provide a landmark to approach the lacrimal sac; an osteotomy is performed with uncinectomy in 90% of cases in one study. The maxillary line has been reported to be an important landmark for uncinectomy and endonasal DCR because it depicts the anterior extent of the uncinate process and corresponds to the suture between the lacrimal bone and maxilla within the lacrimal sac fossa. Incising the uncinate just posterior to the maxillary line would ensure complete removal of the entire process and result in less bleeding.
The operculum of the middle turbinate is an anterior point of insertion of the middle turbinate into the lateral nasal wall. The operculum of the middle turbinate represents the anterosuperior edge of the middle turbinate attached to the frontal process of the maxilla. The operculum of the middle turbinate has also served as an intranasal landmark for identifying the location of the lacrimal sac. Whether or not the operculum of the middle turbinate can serve as a useful landmark of the lacrimal sac fossa in the vertical or anteroposterior position is still debated. The operculum of the middle turbinate has been described by most authors to be located at the upper limit of the sac. However, the position should be researched further because some authors have stated that the bone above the middle turbinate insertion requires removal for full exposure of the sac.
The agger nasi cell is the most anteriorly placed anterior ethmoid cell and has been reported to be present in 78% to 100% of cases. The most anterior ethmoid cell has been described to be removed to perform an osteotomy for dacryocystorhinostomy because it is positioned anteriorly from the posterior lacrimal crest and thus faces the upper and posterior parts of the lacrimal sac fossa in 41%, 79%, and 90% of cases. In some patients, these air cells have been described as possibly extending the entire length of the lacrimal sac fossa.
The lacrimal sac fossa is formed by the frontal process of the maxilla and the lacrimal bone. The frontal process of the maxilla usually occupies the anterior half of the sac, and the thin lacrimal bone covers the posterior half. In particular, the frontal process of the maxilla is thicker than the lacrimal bone and can provide a challenging step for a sufficient osteotomy. However, there are few reports about the thickness and proportion of the frontal process of the maxilla in the lacrimal sac fossa.
There are few reports on the relationship of the lacrimal sac fossa to these bony structures, and the results vary widely. The majority of studies have analyzed the lacrimal system of whites anatomically and presented guidelines for endonasal DCR. It has been our experience that DCR procedures for Asians are more difficult than for whites and we reasoned that the difficulty might be attributable to the anatomic differences in the intranasal structures between the races.
Performing endonasal DCR on Asians with a low nasal bridge is sometimes more difficult than on patients with a higher nasal bridge. Based on such surgical experience, we sought to determine the relationship between nose shape and surgical anatomy for endonasal DCR.
We investigated the relationship between intranasal bony structures adjacent to the lacrimal sac fossa in Asians using high-resolution computed tomography (CT) scans and introduced the methods for successful osteotomy. Furthermore, we attempted to reveal the usefulness of nose shape as a predictor of facility in endonasal DCR.
Methods and Materials
One hundred fifty-two nasal cavities of 76 consecutive patients ≥20 years of age (42 men and 34 women; male-to-female ratio = 1:0.8) who had normal orbital CT scans between January 1, 2005 and December 31, 2007 were studied. We excluded those patients who had a history of thyroid orbitopathy, orbital inflammation, sinusitis, trauma, or other anomalies. All patients had thin-section 2-mm CT sections obtained in the transverse axial and coronal planes throughout the orbits and nasal/paranasal structures. The images were analyzed with a digital image workstation (Sienet Magic-View 1100; Siemens, Erlangen, Germany).
Relationship Between the Lacrimal Sac Fossa and the Uncinate Process
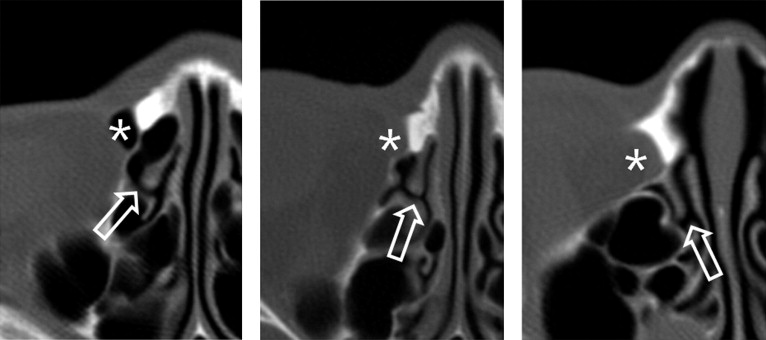
On the axial CT image, the lacrimal sac fossa was divided into the following 3 levels: upper, middle, and lower. The first axial level showing the uppermost part of the lacrimal sac fossa was regarded as the upper level, the axial slice showing the lacrimal sac fossa just before joining the nasolacrimal duct was the lower level, and the mid-slice level between the 2 levels was designated as the middle level. On each level, insertion of the uncinate process was categorized into 3 types, as follows ( Figure 2 ): Left, turbinal position: the uncinate process is inserted onto the lateral wall of the middle turbinate; Middle, maxillary position: the uncinate process is inserted onto the maxillary bone; and Right, lacrimal position: the uncinate process is inserted onto the lacrimal sac fossa.
Location of the Operculum of the Middle Turbinate
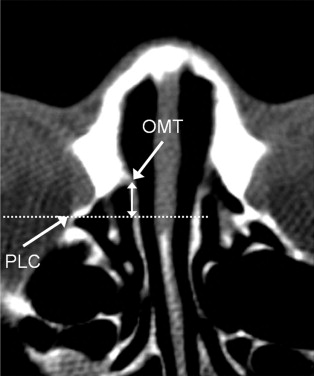
The axial level immediately before the anterior portion of the middle turbinate was separated from the lateral nasal wall was regarded as a level of the operculum of the middle turbinate. To determine the vertical relationship of the operculum of the middle turbinate to the lacrimal sac fossa, the number of slices from the upper level to the lowest slice in which the anterior portion of the operculum of the middle turbinate was attached to the maxilla was counted and converted into the actual distance in millimeters. The anterior projection of the operculum of the middle turbinate from the posterior lacrimal crest was determined by measuring the distance from the rearmost part of the posterior lacrimal crest to the operculum of the middle turbinate ( Figure 3 ).
Relationship Between the Lacrimal Sac Fossa and the Agger Nasi Cell
In order to measure the vertical location of the agger nasi cell from the upper level of the lacrimal sac fossa, the number of slices from the upper level of the lacrimal sac fossa to the lowest slice, where the agger nasi cell was seen, was counted and converted into millimeters.
Thickness and Proportion of the Frontal Process of the Maxilla in the Lacrimal Sac Fossa
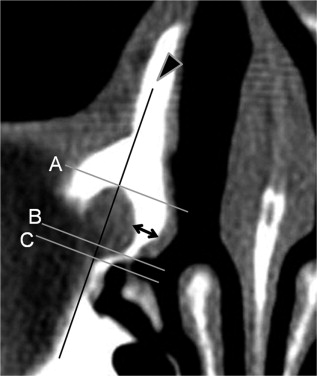
The thickness of the frontal process of the maxilla in the lacrimal sac fossa was measured halfway between the anterior extent of the lacrimal fossa and the maxillary-lacrimal suture line in the 3 levels ( Figure 4 ). The proportion of the frontal process in the lacrimal sac fossa was also determined by measuring the percentage of the frontal process in the long axis of the lacrimal sac fossa after a perpendicular line from the maxillary-lacrimal suture to the long axis line of the lacrimal sac fossa was drawn ( Figure 4 ).
Nasal Bone Height and Length
The nasal bone height was obtained by measuring the distance from a line connecting both nasomaxillary sutures to the rhinion ( Figure 5 ). The nasal bone length was determined by counting the number of slices from the rhinion to the nasion where the frontal bone meets the nasal bone.

Statistics
In all analyses, the mixed-model algorithm in SAS (version 9.1; SAS Institute, Cary, North Carolina, USA) was used. The correlation of the nasal bone and frontal process of the maxilla was assessed by conducting mixed-model analysis using Bonferroni’s correction, in which the height and length of the nasal bone were used as independent variables and the thickness and proportion of the frontal process of the maxilla were used as dependent variables. Also, the correlation of the operculum of the middle turbinate and agger nasi cell was assessed by the same method of analysis, in which the degree of descent of the operculum of the middle turbinate from the upper level of the lacrimal sac fossa was used as an independent variable and the degree of descent of the agger nasi cell was used as a dependent variable. To improve the normality and linearity, log transformation of measurement values was taken into consideration, if necessary. Statistical significance was considered at a P value < .05.
Results
Relationship of the Lacrimal Sac Fossa and the Uncinate Process
The uncinate process was attached to the lacrimal sac fossa in 152 of 152 cases (100%) ( Table 1 ). The anterior insertion of the uncinate process was oblique; the uncinate process generally attached to the lacrimal bone at the lower level, became anterior to the maxillary bone–lacrimal bone at the middle level, and then joined with the middle turbinate at the upper level.
| Position of the UP | Retrolacrimal a | Lacrimal b | Maxillary c | Turbinal d |
|---|---|---|---|---|
| Upper level | ||||
| Current study | 0 (0%) | 0 (0%) | 35 (23.0%) | 117 (77.0%) |
| Fayet study | 4 (5.2%) | 4 (5.2%) | 22 (28%) | 47 (61%) |
| Middle level | ||||
| Current study | 0 (0%) | 17 (11.1%) | 98 (64.5%) | 37 (24.3%) |
| Fayet study | 4 (5.2%) | 18 (23%) | 43 (55.8%) | 12 (15%) |
| Lower level | ||||
| Current study | 0 (0%) | 122 (80.3%) | 30 (19.7%) | 0 (0%) |
| Fayet study | 25 (32%) | 35 (45%) | 17 (22%) | 0 (0%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


