Purpose
To characterize the morphology of outer retinal holes caused by solar maculopathy, using spectral-domain optical coherence tomography (SD-OCT).
Design
This study is an observational case series.
Methods
The SD-OCT findings of 3 patients (6 eyes) with chronic solar maculopathy are presented.
Results
SD-OCT demonstrates a characteristic appearance of partial-thickness hole(s) in the outer retina at the fovea. In 3 of 6 eyes, there is 1 hole directly beneath the umbo. In the remaining 3 eyes, there are multifocal holes spread across the fovea. Holes in more restricted layers, as had been previously reported with time-domain OCT, were not seen. In addition, advanced visualization of SD-OCT data demonstrates a hyperreflective ring around the outer retinal hole.
Conclusions
SD-OCT can be used diagnose solar maculopathy. In patients with central scotomas, characteristic outer retinal hole(s) without inner retinal cystic changes may prompt the clinician to uncover an undisclosed history of sungazing. Similar OCT findings can be caused by welder’s maculopathy, tamoxifen retinopathy, juxtafoveal macular telangiectasia, foveolar vitreomacular traction, or, rarely, a closed macular hole, achromatopsia, alkyl nitrite abuse, acute retinal pigment epitheliitis, or Stargardt disease.
Solar maculopathy is the result of staring at the sun, whether during a solar eclipse or during normal daylight hours. Solar maculopathy is also known in the literature as solar retinopathy, photic maculopathy, “eclipse burns,” and foveomacular retinitis. Outbreaks are regularly reported in regions that experience a solar eclipse. Occasionally, psychiatric patients and patients using recreational drugs stare directly at the sun, and can present with solar maculopathy. Solar maculopathy has even been reported in sunbathers and after religious rituals involving sungazing. Patients may complain of visual loss or may be asymptomatic. Symptomatic patients complain of a central scotoma, which, if large enough, can reduce visual acuity permanently.
The ophthalmoscopic signs of solar maculopathy are limited to the fovea and are well described by Gass and Mainster. In chronic (ie, longstanding) solar maculopathy, there is a small multifaceted outer retinal hole (or holes) with a pigment halo. On first glance, these holes may appear to be small, full-thickness macular holes because of their reddish center. However, on closer inspection, the holes are restricted to the outer retina stereoscopically, and the foveal reflex is often present. Their borders are usually irregular and often have a multifaceted (sharp, angulated) appearance, as opposed to the round or oval appearance of full-thickness macular holes. There is no focal overlying vitreous debris or operculum. The hole(s) may be solitary or multifocal and may occasionally be large. There seems to be much individual variation in the susceptibility to developing permanent vision loss. In the acute stage, there is a yellow spot in the fovea.
In general, the differential diagnosis of ophthalmoscopically isolated foveal pathology is broad. This may include a full-thickness macular hole, an inner lamellar macular hole, a pseudohole associated with an epiretinal membrane, focal geographic atrophy, limited choroidal neovascularization, a small focal area of central serous retinopathy, cystoid macular edema with a large central cyst, idiopathic juxtafoveal telangiectasia (MacTel), a congenital optic pit, whiplash injuries, and a solitary macular cyst. In order to distinguish among these possibilities, or to uncover foveal pathology that is not appreciated ophthalmoscopically, optical coherence tomography (OCT) imaging has been extremely helpful.
Previous studies of solar maculopathy have demonstrated hyporeflective spaces (“holes”) in the outer retina. Like the ophthalmoscopic findings, the outer retinal holes can be focal or multifocal. Foveal thinning has been shown to be correlated with decreased visual acuity. The precise location of the hole(s) and the overall pattern in the fundus are difficult to appreciate using time-domain OCT. Using a prototype ultra-high-resolution OCT scanner, one report of a single patient with chronic solar maculopathy showed that the holes are limited to the outer retina and the en face appearance is irregular. (This scanner is based on different illumination technology than the current, commercially available spectral-domain OCT [SD-OCT] machines. ) Our study demonstrates the detailed appearance of chronic solar maculopathy in 6 eyes of 3 patients using a commercially available SD-OCT scanner, describes a new feature (hyperreflective ring) visible using SD-OCT, and discusses the differential diagnosis of outer lamellar retinal holes and cysts.
Methods
Three patients seen at Massachusetts Eye & Ear Infirmary who had received a diagnosis of solar maculopathy were identified. All 3 patients were imaged with the Cirrus SD-OCT machine (Carl Zeiss Meditec Inc., Dublin, California, USA).
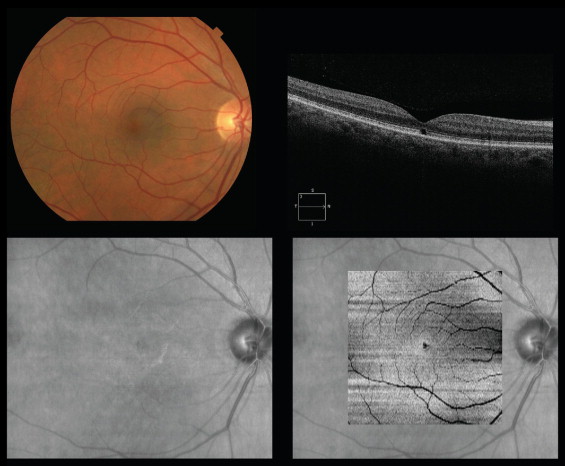
For the stacks of C-scan (en face) images of the outer retina shown in Figure 1 (Bottom right) and in Figure 2 , the Advanced Visualization option of the Cirrus software was used to identify a slab of OCT data restricted to the outer retina. Specifically, a slab was created between the contour formed by the retinal pigment epithelium (RPE) or RPE-fit line and the same contour approximately 50 microns anterior to the RPE. The slab included the data from the RPE to the external limiting membrane. The width of the slab was fine-tuned manually for improved contrast.
Results
Six eyes of 3 patients were analyzed. Patient A is 48-year-old man with a history of schizophrenia who presented with difficulty seeing certain parts of fine print, for example, the “dot on the i, the tail on the Q.” He did admit to sungazing. His best-corrected acuity was 20/20- OD and 20/20- OS. Patient B is a 50-year-old man with a history of schizophrenia who admitted to sungazing 10 to 20 years ago. His visual acuity with correction was 20/30 OU. Fluorescein angiography was normal, and autofluorescence images showed a central hypoautofluorescence centrally OD and a nondiagnostic image (poor contrast) OS ( Supplemental Figure 1 , available at AJO.com ). Patient C is a 47-year-old man with a history of schizophrenia. The patient was a poor historian due to his mental status. His relative did not know of any eye trauma or prolonged sungazing. Because of the lack of any specific associated findings from conditions that can mimic solar maculopathy (see Discussion), he was classified as having a presumed solar maculopathy. Note that even non-schizophrenics with presumed solar retinopathy do not always recall a history of sungazing. His past ophthalmic history is also notable for advanced glaucoma and midperipheral retinal hemorrhages. His visual acuity was 20/200+ (20/125+ with pinhole) OD and 20/80 OS. His reduced visual acuity was attributed to his advanced glaucoma (0.99 cup-to-disc ratio; not shown).
Figure 1 demonstrates the imaging results from the right eye of Patient A. At this relatively low magnification, an irregular fovea is difficult to appreciate clearly in both the color photograph (Top left) and the OCT fundus image (Bottom left). The OCT B-scan (Top right) shows a square-shaped outer retinal hole. An en face image of the OCT data, restricted to the data from the outer retina (see Methods), clearly demonstrates an outer retinal hole.
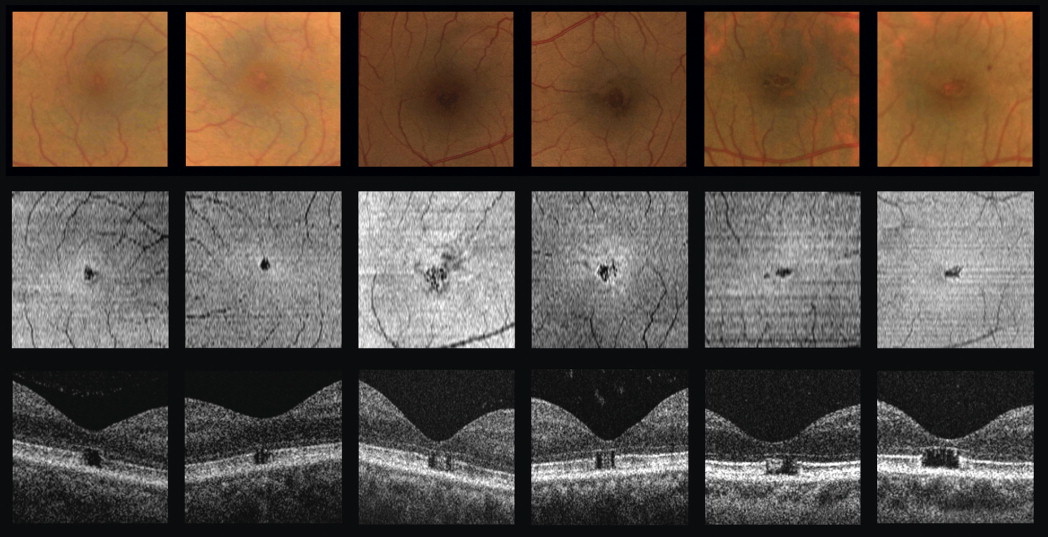
Figure 2 contains a magnified view of the fovea in all 6 eyes in the study. The color photographs show irregular, multifaceted foveolar hole(s). The outer retinal OCT data more clearly demonstrate these holes, which are multifocal in 3 of the 6 eyes and solitary in the other 3 eyes. A hyperreflective ring surrounds the holes, as will be discussed further in Figure 3 . The B-scans show the extent of the outer retinal hole(s), spanning from the RPE layer to the external limiting membrane. Specifically, the hole extends from the inner border of the RPE line up to the external limiting membrane, a region consisting of the inner and outer photoreceptor segments. In Patient B, where 2 RPE lines can be resolved (outer segment/RPE junction and basement membrane/choroid junction, according to the conventions used by Hood and associates ), the inner line is lost while the outer line is preserved. Again, this is consistent with loss of the inner and outer segments.
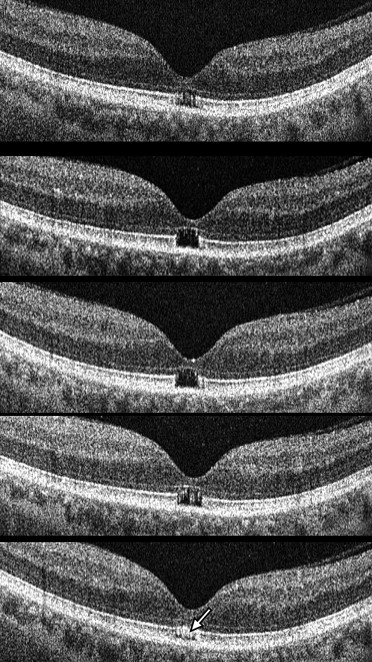
Figure 3 shows a series of adjacent OCT B-scans. A large, solitary outer retinal hole is demonstrated. In addition, there is hyperreflective material lining the edge of the hole, especially the outer edges and top surface at the level of the IS/OS junction line, which correlates with the location of the hyperreflective ring seen around the hole seen in Figure 2 . The correlation was confirmed in additional eyes and was not present in a normal eye ( Supplemental Figures 2–4 , available at AJO.com ).
Macular thickness maps showed preserved central subfield thickness in both eyes of Patient A (231 μm OD, 241 μm OS), reduced central subfield thickness in Patient B (192 μm OD, 191 μm OS), and borderline central subfield thickness in Patient C (219 μm OD, 209 μm OS). The center point thickness (or minimal foveal thickness), as measured manually, was difficult to quantify precisely in these raster scans (not shown).
Results
Six eyes of 3 patients were analyzed. Patient A is 48-year-old man with a history of schizophrenia who presented with difficulty seeing certain parts of fine print, for example, the “dot on the i, the tail on the Q.” He did admit to sungazing. His best-corrected acuity was 20/20- OD and 20/20- OS. Patient B is a 50-year-old man with a history of schizophrenia who admitted to sungazing 10 to 20 years ago. His visual acuity with correction was 20/30 OU. Fluorescein angiography was normal, and autofluorescence images showed a central hypoautofluorescence centrally OD and a nondiagnostic image (poor contrast) OS ( Supplemental Figure 1 , available at AJO.com ). Patient C is a 47-year-old man with a history of schizophrenia. The patient was a poor historian due to his mental status. His relative did not know of any eye trauma or prolonged sungazing. Because of the lack of any specific associated findings from conditions that can mimic solar maculopathy (see Discussion), he was classified as having a presumed solar maculopathy. Note that even non-schizophrenics with presumed solar retinopathy do not always recall a history of sungazing. His past ophthalmic history is also notable for advanced glaucoma and midperipheral retinal hemorrhages. His visual acuity was 20/200+ (20/125+ with pinhole) OD and 20/80 OS. His reduced visual acuity was attributed to his advanced glaucoma (0.99 cup-to-disc ratio; not shown).
Figure 1 demonstrates the imaging results from the right eye of Patient A. At this relatively low magnification, an irregular fovea is difficult to appreciate clearly in both the color photograph (Top left) and the OCT fundus image (Bottom left). The OCT B-scan (Top right) shows a square-shaped outer retinal hole. An en face image of the OCT data, restricted to the data from the outer retina (see Methods), clearly demonstrates an outer retinal hole.
Figure 2 contains a magnified view of the fovea in all 6 eyes in the study. The color photographs show irregular, multifaceted foveolar hole(s). The outer retinal OCT data more clearly demonstrate these holes, which are multifocal in 3 of the 6 eyes and solitary in the other 3 eyes. A hyperreflective ring surrounds the holes, as will be discussed further in Figure 3 . The B-scans show the extent of the outer retinal hole(s), spanning from the RPE layer to the external limiting membrane. Specifically, the hole extends from the inner border of the RPE line up to the external limiting membrane, a region consisting of the inner and outer photoreceptor segments. In Patient B, where 2 RPE lines can be resolved (outer segment/RPE junction and basement membrane/choroid junction, according to the conventions used by Hood and associates ), the inner line is lost while the outer line is preserved. Again, this is consistent with loss of the inner and outer segments.



