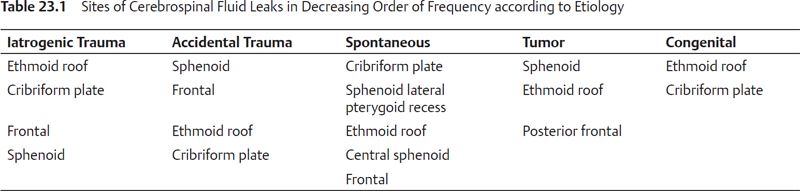
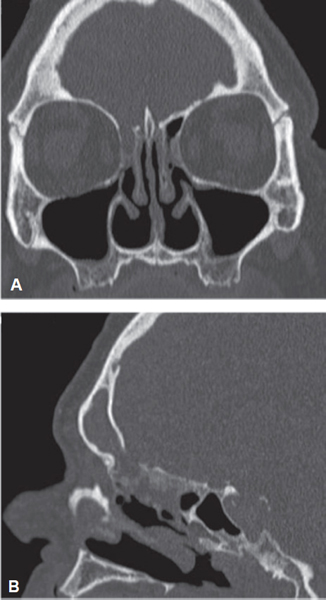
23 Cerebrospinal Fluid: Physiology and Endoscopic Leak Repair Although the Roman physician of antiquity Galen first described cerebrospinal fluid (CSF) rhinorrhea in 200 ad, the first recorded description in modern medicine was not until 1682 by Willis. This was later confirmed on autopsy by Miller in 1862. Grant is credited with the first transcranial repair in 1923, while Dohlman (1948) and Hirsch (1953) described the first extracranial and transnasal approaches, respectively. The evolution of surgical repair of CSF leaks has followed the desire to reduce morbidities associated with open approaches: the invasive nature of the approach, high failure rate, external scars, anosmia, seizures, cerebral hemorrhage, loss of memory, and personality deficits. With the advent of endoscopic sinus surgery (ESS) and advances in instrumentation, Wigand completed the first successful endoscopic CSF leak repair in 1981. The results of multiple institutional series have confirmed the superior efficacy and lower morbidity of the endoscopic approach, making it now widely accepted as the current standard of care.1 A sound understanding of CSF production and circulation is critical in the management of CSF leaks. CSF is a colorless transcellular fluid produced predominantly by the ventricular choroid plexi with minor contributions from their ependymal lining, the external pial-glial membrane, and blood vessels within the pia-arachnoid. Production occurs through active transport (70%) and capillary ultrafiltration (20%) with 10% occurring as a product of metabolic water production. CSF is produced at a rate of 20 mL/h with a total volume of 125 to 150 mL unevenly distributed between the ventricles (20%), the subarachnoid (SA) space of the cranium, and spinal cord (80%) at any one time. A pulsatile wave, generated by cerebral arterial flow and the associated expansion of the vascular compartment in the cranial vault, propels CSF in a craniocaudal direction. This travels from the two lateral ventricles into the single midline third ventricle via the interventricular foramen of Monro. From there it passes into the fourth ventricle via the cerebral aqueduct of Sylvius and ultimately into the SA space by way of three openings in its roof: two foramina of Lushka and the foramen of Magendie. CSF pressure is typically less than 200 mm H2O in adults and is primarily regulated through absorption. Approximately 90% of CSF absorption occur via unidirectional, size-limited, vesicular transport in the arachnoid villi, with the remaining 10% passing directly into the cerebral venules. Absorption of CSF increases linearly above pressures of 70 mm H2O until approximately 110 mm H2O, when the rate of secretion and absorption become equal. Being a product of plasma filtration and membrane secretion, CSF is almost completely acellular with a very low protein concentration of 0.3% (20 to 40 mg/dL). Glucose concentration ranges between 50 and 80 mg/dL, with a low CSF to serum ratio of 0.6 because of its use by the ependymal cells and active removal by arachnoid villi and capillaries.2 CSF leaks can be classified by etiology, size, or location. Etiological classification remains popular because of the ease with which it can be obtained from the patient history. Har-El3 classified CSF leaks into traumatic and nontraumatic. Traumatic leaks are more common and occur through accidental or iatrogenic injury. Iatrogenic fistulae have increased in recent times with the widespread practice of ESS and endoscopic skull base surgery. Nontraumatic causes can be further subclassified into congenital, tumor related, and spontaneous leaks. Table 23.1 lists the common sites of CSF leaks involved in each group. Unintentional iatrogenic CSF leaks occur in the range of 1/1000 to 2/1000 ESS procedures. Leaks occur more frequently on the right side with the most common sites injured being the lateral lamella of the cribriform plate and the ethmoid roof (Fig. 23.1).4 Injury to the paper-thin lateral lamella can occur during a frontal recess clearance or during high resection of the middle turbinate. Posterior ethmoid injuries often occur when excessively pneumatized maxillary sinuses expand superolaterally reducing the height of the ethmoid complex. If the leak is witnessed intraoperatively every effort should be made for immediate repair. Additionally, iatrogenic leaks often occur during endoscopic skull base surgery. This is becoming a more frequent occurrence as rhinologists and neurosurgeons continue to push the envelope of minimally invasive skull base surgery. Often these defects can be quite large and extend up into the ventricles, resulting in high volume CSF leaks. It is imperative that skull base reconstruction is done in a meticulous fashion in these patients. Figure 23.1 (A) Coronal and (B) sagittal computed tomography scans showing an iatrogenic cerebrospinal fluid leak in the anterior ethmoid roof location. Closed head injuries have replaced projectiles as the most common accidental cause with 1 to 3% resulting in fistula. The sphenoid and cribriform plate are the most common sites with up to one-third of patients having multiple sites.5 CSF rhinorrhea usually presents within 48 hours. Most traumatic leaks spontaneously close (50 to 90%) likely as a consequence of the sealant effect provided by blood products and localized inflammation.6 Historically, conservative management with bed rest and lumbar drains has been the mainstay of treatment. Surgical intervention is advocated after 7 to 10 days for persistent leaks to reduce the risk of developing ascending meningitis (30 to 40%), although some argue that earlier surgical repair may reduce the risk further. The use of prophylactic antibiotics in traumatic CSF leaks remains controversial, with two meta-analyses on the subject that provided conflicting evidence on their effectiveness in reducing the rate of ascending meningitis.7,8 Both studies had methodological flaws however, and in 2011, a Cochrane Database review was performed to address the deficiencies of these meta-analyses. This extensive review of more than 20 randomized and nonrandomized trials concluded that there was insufficient evidence supporting the role of prophylactic antibiotics in CSF leaks associated with traumatic base of skull fractures.9 Congenital encephaloceles with leakage of CSF can be subclassified into sincipital (frontoethmoidal) and basal types. Basal types tend to be encountered more commonly by rhinologists. This type most often presents as a nasal mass but may also present with rhinological symptoms, meningitis, and craniofacial deformities. Most commonly, congenital encephaloceles occur near the middle turbinate’s attachment to the cribriform plate. They pose a challenge to the repairing surgeon, both technically and with regard to timing. The potential for telecanthus to occur over time has been described in cases that are left untreated.10 Intracranial and sinonasal tumors can be responsible for CSF leaks through direct invasion and erosion of the skull base by the tumor. Indirectly, defects can also occur when chemotherapy and radiotherapy treatments are used to shrink these tumors; this can lead to devitalization of the bony skull base. Additionally, tumors may block the CSF pathway, resulting in obstructing hydrocephalus. Repairing the CSF leak without relieving the raised intracranial pressure (ICP) may further exacerbate the intracranial hypertension and is likely to fail. Spontaneous CSF leaks occur in the absence of a discernible cause, although increased ICP is thought to play a central role in most cases. They represent a distinct entity with differing demographic, radiographic, and clinical manifestations. Patients are typically obese, middle-aged women who often present with symptoms of benign intracranial hypertension (BIH). Radiologic features include empty sella, arachnoid pits, dural ectasia, optic nerve changes, widespread skull base attenuation, and pneumatization of the lateral sphenoid recess.11 Surgeons should identify these patients as they often have multiple leak sites, coexistent meningoencephaloceles, and are more likely to recur following repair without management of the underlying intracranial hypertension. Essential to the successful management of CSF leaks is the definitive diagnosis of a leak and the precise localization of its site. The detection of β-2 transferrin in nasal secretions using immunoelectrophoresis remains the most commonly used diagnostic test for confirmation of CSF leaks. Beta-2 transferrin is found only in CSF, perilymph, and aqueous humor. This results in a high diagnostic sensitivity (97%) and specificity (93%).12 Only 0.17 mL is needed for testing and β-2 transferrin is stable for up to 7 days regardless of collection site or storage temperature.13 False-positive results are uncommon but can occur in patients with liver cirrhosis or contamination with neuraminidase secreting bacteria. Beta-trace protein is commonly used in Europe with similarly high specificity and sensitivity. Precise localization of the CSF leak is one of the critical factors in the success of fistula repair. A summary of localization methods can be seen in Table 23.2. Imaging is useful in all cases of CSF repair for identifying potential sites, delineating the bony anatomy, and sizing the osseous defect. Imaging modalities commonly used include axial and direct coronal standard CT, high-resolution multidetector helical CT with multiplanar coronal and sagittal reconstruction, CT cisternography with iodinated and nonionic contrast agents, and magnetic resonance imaging (MRI) with and without intrathecal gadolinium. The sensitivity of high-resolution CT in leak localization when compared with intraoperative endoscopic findings has been shown to be > 90%. Furthermore, when submillimeter collimation is available, very accurate radiologic sizing of the osseous defect is demonstrated.14 Although utilized commonly in the early days of CSF leak repair, CT cisternograms are now used less because of their invasiveness and lower sensitivity. With this said, they may still have a role in select cases of very low volume/intermittent leaks or in localization of the dural defect in cases with multiple or broad-based osseous defects.15 MRI has also been shown to be sensitive (75 to 90%) for CSF leak identification with a specificity close to 100%.16
Anatomy and Physiology
Classification of Cerebrospinal Fluid Leaks
Traumatic—Iatrogenic Leaks
Traumatic—Accidental Leaks
Nontraumatic—Congenital Leaks
Nontraumatic—Tumor Leaks
Nontraumatic—Spontaneous Leaks
Preoperative Work-Up
Diagnosis
Localization
Imaging
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


