Fig. 39.1
(a, b) Multiple cervical lesions noted on MRI spine consistent with multiple sclerosis
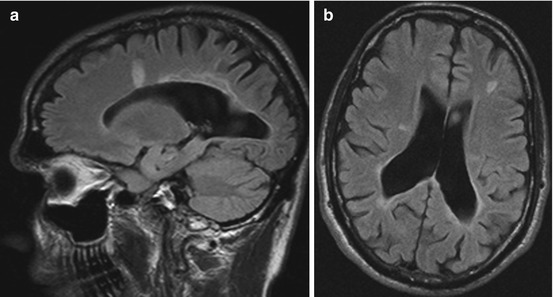
Fig. 39.2
(a, b) Periventricular and juxtacortical lesions on MRI brain
After the workup, the patient underwent an occipital nerve block with xylocaine and immediately achieved a significant (80 %) reduction in his pain intensity. He was then started on carbamazepine, which was increased to 400 mg twice daily with good control of his symptoms.
39.4 Summary of the Case
Our patient presented for evaluation for new paroxysmal occipital pain in the setting of relapsing remitting MS and a long-standing history of migraine with visual aura. His occipital symptoms are described as stabbing, sharp, and intermittent, with pain around the posterior scalp on the left with allodynia in that area. Pain radiated to the front of the head, a finding explained by convergent input to the trigeminal nucleus caudalis from the upper cervical roots and the first division of the trigeminal nerve. Clinically, he has features that are most typical for occipital neuralgia, though some aspects are reminiscent of Lhermitte’s sign, which may share a common pathogenesis in some cases (i.e., lesions in the upper cervical spine) of occipital neuralgia. His workup confirmed the presence of a lesion in the upper cervical spine consistent with a probable demyelinating etiology. Such localization has been noted in case series of MS patients with occipital neuralgia-type pain.
39.5 Definition of Central Neuropathic Pain Attributable to Multiple Sclerosis
The International Association for the Study of Pain (IASP) in its Taxonomy, revised in 2011, defined central pain as “pain initiated or caused by a primary lesion or dysfunction in the central nervous system.” This was distinguished from peripheral neuropathic pain (i.e., caused by damage to the peripheral somatosensory nervous system, such as peripheral neuropathy or radiculopathy) as well as from nociceptive pain (i.e., from damage to nonneural tissue attributed then to activation of nociceptors, such as damage to muscles, joints, viscera, etc.). The International Headache Society criteria define the syndrome of central neuropathic pain attributable to MS as involving unilateral or bilateral craniocervical pain with a range of clinical symptoms. Sensory symptoms, if present, should be attributable to demyelination of the central nervous system, though precise localization is often difficult. Silent lesions and unexplained symptoms are common.
39.6 Brief General Information
Central pain syndromes in MS are both common and clinically significant. A range of recent data has found that the large percentage of MS patients experience neuropathic pain and many will present with multiple pain complaints. Central pain in MS may manifest as dysesthetic limb pain, trigeminal neuralgia (TN), occipital neuralgia, Lhermitte’s sign, and painful tonic spasms, among others. Though prevalence estimates vary, most support the idea that dysesthetic limb pain remains the most common form of central pain in MS, followed by Lhermitte’s sign, and then the cranial neuralgias. Beyond a single case series, very little evidence regarding occipital neuralgia in MS has been reported. Trigeminal neuralgia, however, has been recognized for some time as a common entity in MS patients. Some cases of TN in MS show well-situated plaques in the trigeminal root zone of the pons, while other patients with similarly placed lesions remain asymptomatic.
Central pain syndromes have been attributed to damage to the spinothalamocortical pathways. However, imaging studies generally show disseminated lesions in both brain and spinal cord, which do not readily correlate to pain symptomatology. Damage to spinal cord nociceptive pathways mediated through loss of GABA inhibitory interneurons has also been proposed as a possible contributing factor. Regardless, pain symptoms in MS are often patchy, highly variable, and typically associated with abnormalities in quantitative sensory testing.
Risk factors for the development of chronic pain in MS patients are inconsistent, with the association between pain syndromes and older age, longer disease duration, and greater disease severity being somewhat controversial. There is good evidence, however, that patients with one pain syndrome appear to be more likely to have another pain syndrome. Chronic pain has also been frequently linked to comorbid depression, anxiety, and several other psychosocial factors including scores on pain coping scales and pain-related catastrophizing.
In our patient, a new central pain syndrome is superimposed on long-standing migraine, reflecting the complicated reality of coexisting pain syndromes in MS. Migraine appears to be associated with MS, and MS patients have been found in a number of studies to be more than twice as likely to report migraine headaches.
Despite case reports of headaches triggered by acute MS lesions, in the majority of cases, the headache symptoms preceded the diagnosis of MS, suggesting a more complex relationship between primary headache disorders and MS than a “single-lesion” theory may imply. Given that most headache disorders precede the diagnosis of MS by several years, recent work has looked at the idea that migraine may predispose patients to developing MS. In particular, our own recent work suggests that migraine constitutes a modest risk factor for the development of MS. Hypothetically, migraine may lead to changes in the permeability in the blood-brain barrier and endothelial damage, thereby lowering the threshold for developing CNS-directed autoimmune process in susceptible individuals.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


