and John Danias4
(3)
Department of Ophthalmology, Beth Israel Hospital, New York Eye and Ear Infirmary, New York, NY, USA
(4)
Department of Ophthalmology, SUNY Downstate Medical Center, Brooklyn, NY, USA
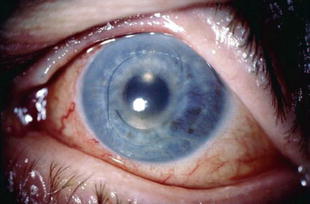
Intraoperative floppy-iris syndrome (IFIS) is a condition characterized by a triad of intraoperative findings: (1) iris fluttering occurring under normal fluidic conditions, (2) iris billowing and prolapse to the phaco and side-port incisions despite proper wound construction, and (3) progressive miosis. Poor preoperative dilation and failure of dilation despite mechanical stretching of the pupil are additional characteristics. IFIS was first described in 2005 by Chang et al. in patients undergoing phacoemulsification while being treated with tamsulosin. The intraoperative findings make cataract surgery in eyes with IFIS difficult and lead to increased risk of complications. More recently, IFIS has been reported to complicate routine trabeculectomy surgery in patients taking alpha-antagonists.
Tamsulosin hydrochloride (Flomax) is the most commonly prescribed medication for treatment of benign prostatic hyperplasia (BPH) and associated symptoms of lower urinary tract obstruction (LUTS). It is reported that 50 and 80 % of men over the age of 50 and 85, respectively, require treatment for LUTS. Over the last decade, pharmacotherapy as opposed to surgery has become a first-line treatment for BPH/LUTS, and tamsulosin is considered a first-line therapeutic agent. Therefore, it is not surprising that more patients undergoing cataract surgery are using tamsulosin, thus accounting for the progressive increase in the incidence of IFIS. In fact, IFIS associated with the use of tamsulosin occurs in approximately 2 % of cataract cases.
Tamsulosin is a selective α1-adrenergic-receptor (AR) blocker with a tenfold greater affinity for α1a and α1d receptors than for α1b-adrenergic receptors. This distinguishes tamsulosin from other alpha-blockers available in the United States—terazosin, doxazosin, and alfuzosin—that all have similar affinity for all three α1-receptor subtypes. Studies have shown that (alpha) α1a AR-selective antagonists relieve obstructive symptoms of LUTS via relaxation of the prostate smooth muscle, whereas (alpha) α1d AR-selective antagonists relieve bladder-based irritability symptoms. In contrast, blockade of the α1b-adrenergic receptors leads to orthostatic hypotension, a side effect associated with nonselective alpha-blockers.
Two α1-ARs have been identified in the iris: α1a and α1b. Several studies have confirmed the presence of the α1a-AR in the rabbit iris dilator muscle, as well as its role in the sympathetic mediation of mydriasis. In contrast, α1b-AR has been localized to the iris arterioles. Although α1-AR localization has not been reported for the human eye, it is on the basis of these animal studies that IFIS has been proposed to develop. Specifically, it has been proposed that the blockade of the postsynaptic α1a-AR in the iris dilator smooth muscle by tamsulosin causes IFIS. This theory is further supported by a report of intraoperative reversal of miosis and possible increase in iris tone after intracameral administration of phenylephrine (an α1-AR agonist that competes with tamsulosin for α1a-ARs).
However, this proposed mechanism cannot explain all the features of IFIS. While it is likely that tamsulosin blockade of α1a-AR causes miosis, it does not explain well the iris floppiness or the elasticity of the pupillary margin. In describing the syndrome, Chang et al. proposed that the iris propensity to billow and prolapse was caused by disuse iris dilator atrophy. They suggested that tamsulosin’s long half-life and a relatively constant receptor blockade lead to disuse atrophy of the iris, which in turn contributes to low iris tone and the presence of a small pupil long after tamsulosin cessation. Although this concept has been disputed by Schwinn et al. based on previous work demonstrating denervation supersensitivity of the α1-AR in rabbits, it is still quite popular.
In addition to the α1a-AR blockade, an interaction between the α1-AR blockers and melanin has been postulated to contribute to IFIS. α1-ARs appear to be significant in melanogenesis, as their blockade in the neonatal period causes a decrease in iris pigmentation. More recently, Goseki et al. reported structural changes in the irides of patients with IFIS. These changes included vacuolation of the dilator muscle cells as well as irregularity of melanocyte pigment granules and presence of lipofuscin-like granules in the iridal clump cells—giant pigment cells in the iris stroma that are believed to be resident macrophages. The authors hypothesized that high local concentration of the α1-AR blocker in the melanocytes of pigment epithelium contributes to the atrophy of the intimately proximal dilator smooth muscle cells and causes IFIS. However, studies in rabbit irides did not find increased binding of α1a-AR drugs to melanin, as evidenced by similar binding of α1a-AR agonist in pigmented and albino irides.
The theory of iris dilator muscle atrophy as the cause of IFIS was also investigated by Kim et al. In this study, the authors demonstrated lack of identifiable myofibrils in iris dilator muscle on electron microscopy of peripheral iridectomy samples from patients on tamsulosin. This finding was in contrast to lack of observed difference on light microscopy in iris dilator muscle thickness between tamsulosin-treated and control iridectomy samples. Also of importance was the lack of direct relationship between duration of tamsulosin use and dilator muscle thickness.
Finally, contrary to the previous reports and based on histopathological evidence, we have proposed that the main site of IFIS pathology is the muscularis of the iris arterioles (in review).
According to a recently published survey, 95 % of the American Society of Cataract and Refractive Surgery (ASCRS) members found that tamsulosin makes cataract surgery more difficult, and 77 % reported that it increases the risk of complications. In the original report by Chang et al., vitreous loss occurred in 12 % of IFIS cases. Posterior capsular rupture was reported in 22 % of resident cataract surgery in patients taking tamsulosin. Significant intraoperative iris trauma was also reported by 52 % of surveyed cataract surgeons in eyes with IFIS. IFIS-associated posterior capsular rupture and vitreous loss were reported to be much lower (0.6 % only) in a follow-up report by Chang et al. suggesting that as surgeons become more aware of the syndrome and anticipate it, the risk of surgical complications decreases.
There appears to be a spectrum of severity of tamsulosin-associated IFIS. In one study, mild, moderate, and severe IFIS was reported in 17, 30, and 43 % of patients on tamsulosin, respectively, with no IFIS in 10 %. Other studies confirmed the spectrum of IFIS severity in patients on tamsulosin but reported a much lower incidence of IFIS (with only 43–57 % of patients on tamsulosin showing any signs of IFIS).
Various management strategies have been proposed in an effort to ensure safe surgery in patients with IFIS. Preoperative discontinuation of tamsulosin was originally recommended, but has been found to be ineffective. It is currently routinely employed by only 20 % of surveyed cataract surgeons. This lack of effect of short-term discontinuation of tamsulosin on IFIS severity can be explained by the presence of significant levels of tamsulosin in the aqueous humor of 60 % of patients who discontinue the drug for up to 4 weeks. Another preoperative strategy is the topical administration of atropine 1 % three times daily for 1–2 days prior to surgery. It should be noted that when administering atropine, discontinuation of systemic alpha-blockers is not recommended because of the risk of acute urinary retention. The most important of the preoperative strategies by far, however, is obtaining a careful present and past drug use history and recognition of the potential problem.
Various intraoperative maneuvers have been suggested for use in IFIS cases. Strategies include careful wound construction, use of gentle hydrodissection, directing irrigating currents away from the pupillary margin, and lowering the irrigation, aspiration rates, and vacuum levels. All of these maneuvers help decrease turbulence in the anterior chamber and decrease washout of the ocular viscosurgical device (OVD). In addition, 38 % of surveyed cataract surgeons routinely administer dilute intracameral unpreserved α1 agonists such as phenylephrine and epinephrine (0.25 ml of 2.5 % unpreserved phenylephrine diluted with 2 ml of BSS or unpreserved epinephrine 1:2,500–1:4,000).
Use of the viscoadaptive agent, sodium hyaluronate 2.3 % (Healon 5, AMO, Santa Ana, CA), is another widely used strategy. Fifteen percent of cataract surgeons reported its use in IFIS cases. As a super-cohesive OVD, Healon 5 aids in mydriasis and blocks iris prolapse through the wound. Unlike other cohesive agents, however, its pseudodispersive quality allows Healon 5 to remain in the eye and maintain anterior chamber depth at higher flow rates. It is reported that 95 % of IFIS cases that utilized Healon 5 did not require the use of adjunctive mechanical devices.
Mechanical devices include iris hooks and pupil expansion rings and are employed to dilate the pupil and prevent iris prolapse. Iris hooks are generally preferred to the expansion rings (23 % vs. 4 %). Positioning the hooks in a diamond configuration with one of the retractors placed through a separate paracentesis just below the main corneal incision further minimizes iris prolapse and trauma. However, once capsulorhexis has been performed, it becomes difficult to place iris hooks safely without capturing the capsular edge. Therefore, the ability to anticipate IFIS and the placement of mechanical devices early in surgery becomes very important. Two other common techniques for small pupil management—mechanical stretching of the pupil and partial thickness sphincterotomies—are ineffective in IFIS and may exacerbate it.
Following the original description of IFIS and its association with tamsulosin, other case reports of IFIS occurring in patients on nonselective α1-AR blockers, as well as saw palmetto (Serenoa repens, an over-the-counter alternative therapy for BPH, believed to act via 5-alpha reductase pathway and also found to have α1-AR-inhibitory properties), have been described. One retrospective study reported a 15.4 % risk of IFIS in patients on alfuzosin compared to an 86.4 % risk in patients on tamsulosin. However, two prospective studies failed to show any significant associations between nonselective α1-AR blockers and IFIS. Alfuzosin’s ability to antagonize phenylephrine-induced contraction of the iris dilator muscle in pigmented rabbits is much lower than that of tamsulosin, and in addition its serum concentrations may be too low to antagonize the effect of perioperative alpha-agonist administration on the dilator muscle.
In 2007, Au et al. reported the first case of IFIS during trabeculectomy in a patient on doxazosin. The authors described excessive iris prolapse through the sclerostomy and the paracentesis site. They also reported difficulty to reposition the iris into the anterior chamber after peripheral iridectomy during routine trabeculectomy with the use of an anterior chamber (AC) maintainer. Intraoperative management of IFIS included switching off the AC maintainer in order to decompress the eye and suturing of the sclerostomy with releasable sutures prior to resumption of the AC infusion. Postoperatively, the location of peripheral iridectomy was noted to be less basal than desired without ostium obstruction. The authors recommended thorough preoperative assessment on prior alpha-antagonist use if planning to use the AC maintainer during trabeculectomy. They also suggested lowering the infusion rate or omitting the use of the maintainer altogether if the risk of IFIS exists, as well as preoperative use of pilocarpine or intraoperative use of Miochol.
Since the initial report of IFIS during trabeculectomy, other cases have been reported in patients on tamsulosin and alfuzosin. The authors described similar iris prolapse through the ostium after sclerostomy during trabeculectomy without the use of an AC maintainer in a patient with history of tamsulosin use and preoperative use of pilocarpine 4 %. Certain intraoperative strategies such as cutting a large peripheral iridectomy, stroking the cornea, sweeping the iris with a Rycroft cannula through the paracentesis incision, and using intracameral injections of viscoelastic and Miochol exacerbated the iris prolapse. Final iris repositioning was achieved by using bimanual irrigation/aspiration probes to sweep the iris into the anterior chamber after creation of a second side-port incision. In the second case report, the authors recommended use of two iris hooks in what is described to be a “fish mouth” configuration in order to prevent iris prolapse. They created two paracentesis incisions at the 3 and 9 o’clock positions through which they placed iris hooks and used them to create a “fish mouth” pupil configuration prior to sclerostomy. This step stretched tight the superior iris and allowed the surgeon to perform an uncomplicated peripheral iridectomy. The iris was then described to return to its preoperative position.
In our own practice, we encountered a case of IFIS during trabeculectomy in a patient taking tamsulosin. Excessive iris prolapse through the ostium was observed immediately after sclerostomy despite prior administration of an OVD. The iris continued to prolapse even after a broad basal peripheral iridectomy was created. Final repositioning of the iris into the anterior chamber was achieved by sweeping the iris with an iris spatula through the paracentesis incision aided by a cohesive OVD and subsequent closure of the sclerostomy with interrupted nylon sutures (in review).
It is important to point out that there are multiple other disease states and drugs that can potentially cause similar iris findings. In diabetics, surgically induced miosis has been reported to occur with greater frequency compared to normal controls during routine cataract surgery. Resting pupil size in diabetic patients has also been noted to be smaller than that in healthy subjects—a finding attributed to sympathetic neuropathy. More recently, changes in the distribution and concentration of the potent vasoconstrictor endothelin-1 (ET-1) that mediates iris dilator contraction via endothelin-A (ETA) receptors have been proposed to occur in patients with diabetes and hypertension. In addition, ETA-selective inhibitors have been shown to relax smooth muscle contraction, as demonstrated by a blockade of norepinephrine- and angiotensin II-mediated vasoconstriction in human subjects. It, thus, appears that control of iris dilation and contraction is a multifactorial process. Therefore, rather than focusing on one drug as the cause of IFIS of variable severity, perhaps multiple factors should be considered in order to determine the risk of IFIS and its severity.
In summary, IFIS is an important risk factor for cataract surgery complications. Although the exact mechanism of IFIS has yet to be elucidated, several preoperative and intraoperative strategies can be employed to reduce the rate of complications. Of these, by far the most important risk-reducing strategy is preoperative recognition of the patient at risk. Therefore, careful history taking remains crucial to surgical success.
Acknowledgments
Supported by NEI EY 01867 and an unrestricted grant from RPB.
Bibliography
Akhtar RA, Abdel-Latif AA. Surgical sympathetic denervation increases alpha 1-adrenoceptor-mediated accumulation of myoinositol trisphosphate and muscle contraction in rabbit iris dilator smooth muscle. J Neurochem. 1986;46:96–104.
Au L, Wechsler D, Fenerty C. Alpha antagonists and intraoperative floppy iris syndrome (IFIS) during trabeculectomy. Eye. 2007;21:671–2.
Blouin M, Blouin J, Perreault S, et al. Intraoperative floppy iris syndrome associated with Alpha-1 adrenoreceptors. Comparison of tamsulosin and alfuzosin. J Cataract Refract Surg. 2007;33:1227–34.
Chadha V, Borooah S, Tey A, et al. Floppy iris behaviour during cataract surgery: associations and variations. Br J Ophthalmol. 2007;91:40–2.
Chang DF, Braga-Mele R, Mamalis N, et al. Clinical experience with intraoperative floppy-iris syndrome. Results of the 2008 ASCRS member survey. J Cataract Refract Surg. 2008;34:1201–9.
Chang DF, Campbell JR. Intraoperative floppy iris syndrome associated with tamsulosin. J Cataract Refract Surg. 2005;31:664–73.
Chang DF, Osher RH, Wang L, Koch DD. A prospective multicenter evaluation of cataract surgery in patients taking tamsulosin (Flomax). Ophthalmology. 2007;114:957–64.
Dhingra N, Rajkumar KN, Kumar V. Intraoperative floppy iris syndrome with doxazosin. Eye. 2007;21:678–9.
Goepel M, Hecker U, Krege S. Saw palmetto extracts potently and noncompetitively inhibit human alpha1-adrenoceptors in vitro. Prostate. 1999;38:208–15.
Goseki T, Shimizu K, Ishikawa H, et al. Possible mechanism of intraoperative floppy iris syndrome: a clinicopathological study. Br J Ophthalmol. 2008;92:1156–8.
Gurbaxani A, Packard R. Intracameral phenylephrine to prevent floppy iris syndrome during cataract surgery in patients on tamsulosin. Eye. 2007;21:331–2.
http://stream.expoplanner.com/ascrs2006/hand-outs/076414_powerpointtamsulosin.ppt. Accessed 10 Mar 2009.
Koike T, Kitazumi H, Mukai H. Tissue distribution of NS-49, a phenethylamine class alpha1A-adrenoceptor agonist, in pigmented rates. Arzneimittelforschung. 2001;51:402–7.
Manvikar S, Allen D. Cataract surgery management in patients taking tamsulosin staged approach. J Cataract Refract Surg. 2006;32:1611–14.
Masket S, Belani S. Combined preoperative topical atropine sulfate 1 % and intracameral nonpreserved epinephrine hydrochloride 1:2500 for management of intraoperative floppy-iris syndrome. J Cataract Refract Surg. 2007;33:580–2.
Mirza SA, Alexandridou A, Marshall T, et al. Surgically induced miosis during phacoemulsification in patients with diabetes mellitus. Eye. 2003;17:194–9.
Norris JH, Mall S, Burnett CAM. Floppy iris syndrome hull hooks (FISH Hooks): a new technique for managing IFIS in trabeculectomy surgery. Eye. 2009;23(3):743–4.
Odin L, O’Donnell Jr FE. Adrenergic influence on iris stromal pigmentation: evidence for alpha-adrenergic receptors. Invest Ophthalmol Vis Sci. 1982;23:528–30.
Oshika T, Ohashi Y, Inamura M, et al. Incidence of intraoperative floppy iris syndrome in patients on either systemic or topical alpha (1)-adrenoceptor antagonist. Am J Ophthalmol. 2007;143:150–1.
Palea S, Chang DF, Rekik M, et al. Comparative effect of alfuzosin and tamsulosin on the contractile response of isolated rabbit prostatic and iris dilator smooth muscles. Possible model for intraoperative floppy iris syndrome. J Cataract Refract Surg. 2008;34:489–96.
Parssinen O, Leppanen E, Keski-Rahkonen P, Mauriala T, Dugue B, Lehtonen M. Influence of tamsulosin on the iris and its implication for cataract surgery. Invest Ophthalmol Vis Sci. 2006;47:3766–71.
Schwinn DA, Afshari NA. Alpha-1-Adrenergic receptor antagonists and the iris: new mechanistic insights into floppy iris syndrome. SurvOphthal. 2006;51:501–12.
Schwinn DA, Roehrborn CG. Alpha-1-Adrenoceptor subtypes and lower urinary tract symptoms. Int J Urol. 2008;15:193–9.
Settas G, Fitt AW. Intraoperative floppy iris syndrome in a patient taking alfuzosin for benign prostatic hypertrophy. Eye. 2006;20:1431–2.
Smith SA, Smith SE. Evidence for a neuropathic etiology in the small pupil of diabetes mellitus. Br J Ophthalmol. 1983;67:89–93.
Suzuki F, Taniguchi T, Nakamura S, et al. Distribution of alpha-1 adrenoceptor subtypes in RNA and protein in rabbit eyes. Br J Pharmacol. 2002;135:600–8.
Takmaz T, Can I. Clinical features, complications, and incidence of intraoperative floppy iris syndrome in patients taking tamsulosin. Eur J Ophthalmol. 2007;6:909–13.
Venkatesh R, Veena K, Gupta S, Ravindran RD. Intraoperative floppy iris syndrome associated with terazosin. Indian J Ophthalmol. 2007;55:395–6.
Wenzel RR, Ruthemann J, Bruck H, et al. Endothelin-A receptor antagonist inhibits angiotensin II and noradrenaline in man. Br J Clin Pharmacol. 2001;52:151–7.
Wollensak G, Schaefer HE, Ihling C. An immunohistochemical study of endothelin-1 in the human eye. Curr Eye Res. 1998;17:541–5.
Yamada T, Okuyama Y, Mukai H. In vitro melanin binding of NS-49, a phenethylamine class alpha 1A-adrenoceptor agonist. Arzneimittelforschung. 2001;51:299–303.
Yeu E, Grostern R. Saw palmetto and intraoperative floppy-iris syndrome. J Cataract Refract Surg. 2007;33:927–8.
Yu Y, Koss MC. Studies of alpha-adrenoceptor antagonists on sympathetic mydriasis in rabbits. J Ocul Pharmacol Ther. 2003;19:255–63.
Zaczek A, Zetterstrom C. Cataract surgery and pupil size in patients with diabetes mellitus. Acta Ophthalmol Scand. 1997;75:429–32.
Ziada A, Rosenblum M, Crawford ED. Benign prostatic hyperplasia: an overview. Urology. 1999;53:1–6.
Surgical Options for the Management of Cataract and Glaucoma
Three standard surgical options for the management of patients with cataract and glaucoma are generally acknowledged:
1.
Cataract extraction with IOL implantation alone
2.
Sequential surgery—trabeculectomy followed by cataract extraction with IOL implantation
3.
Combined surgery—cataract extraction with IOL implantation combined with trabeculectomy
Cataract Extraction with IOL Implantation Alone
The option of cataract extraction with IOL implantation alone is appropriate for patients with a visually disabling cataract whose glaucoma is considered mild based on the appearance of the optic disk and minimal visual field loss. Generally speaking, these patients have their IOP readily controlled on one or two topical medications, and they are compliant with the medical regimen. They are stable with respect to their glaucoma and surgical intervention is needed only for coexisting cataract. It should be noted that laser trabeculoplasty does appear to be a bit more effective in patients before they undergo cataract surgery, although the reason for this is not well understood [10]. Therefore, for patients with marginal IOP control but who are not considered candidates for incisional glaucoma surgery, it may be advisable to perform laser trabeculoplasty first, wait several months, and then consider cataract surgery. Current techniques for phacoemulsification and IOL insertion are associated with excellent functional outcomes and are easier to perform than combined procedures. Phacoemulsification alone in glaucomatous eyes has been associated with a long-term reduction of IOP as well as less need for postoperative medications. This reduction in IOP is long lasting; several studies have reported reduction in pressure persisting up to 5 years postoperatively [11–14]. With clear-corneal phacoemulsification, especially when performed temporally, the superior conjunctival tissue is preserved should trabeculectomy be required in the future.
The major concern with this option is the possibility of a significant IOP elevation in the immediate postoperative period. Transient elevations in IOP after cataract surgery are associated either with acutely altered aqueous outflow (secondary to inflammation or retained viscoelastic material) or develop as a consequence of the glaucoma process itself. Significant elevations in IOP are common within the first 24 h after ECCE. With phacoemulsification, the level of elevation and the magnitude of IOP spikes are considerably less than with ECCE. Glaucoma patients who have cataract surgery alone should be adequately controlled preoperatively, with the expectation that if elevation of IOP occurs postoperatively, it can be easily treated and that the period of elevated IOP should not have an adverse effect on the optic nerve (Sidebar 30.2).
Sidebar 30.2. Anterior Chamber Intraocular Lenses, Pupillary Block, and Peripheral Iridectomy
(5)
Department of Ophthalmology, University of Tennessee Health Science Center, Memphis, TN, USA
(6)
Hamilton Eye Institute, University of Tennessee, Memphis, TN, USA
(7)
Department of Ophthalmology, University of Virginia School of Medicine, 800715, Charlottesville, VA 22908-0715, USA
Despite advances in instrumentation and surgical techniques for cataract surgery, glaucoma following cataract surgery remains a common problem. Elevation of intraocular pressure (IOP) may occur early or late in the postoperative course due to a variety of mechanisms, resulting in either open- or closed-angle glaucoma. Angle-closure glaucoma after anterior chamber intraocular lens (ACIOL) implantation is usually preventable and, when it does occur, can be effectively treated.
In pseudophakic pupillary block glaucoma, the implanted intraocular lens (IOL) is involved in the obstruction of the aqueous flow through the pupil, resulting in iris bombe with subsequent closure of the drainage angle. This condition is more frequently encountered in the presence of an ACIOL than with a posteriorly implanted IOL (PCIOL). Potential mechanisms include obstruction by the smooth round optical portion of the IOL or development of adhesions between vitreous and the posterior iris.
While the role of routine surgical iridectomy is controversial in posterior chamber implants, it is widely accepted as standard of care in anterior chamber implants. Surgical iridectomy performed at the time of an ACIOL implant provides an alternate route for aqueous to pass from the posterior into the anterior chamber if the pupil becomes blocked by an intact vitreous face or the IOL itself. This critical step is often neglected intraoperatively due to elevated anxiety and distraction from the impetus for ACIOL implantation (prolapsed vitreous, ruptured capsule, zonule instability) or in haste to complete the case (Figs. 30.1, 30.2, and 30.3).