(11)
School of Optometry and Vision Sciences, University of Auckland, Auckland, New Zealand
8.1.1 Background
A 31-year-old female (RM), diagnosed with moderate dry eye 6 months previously by her ophthalmologist, was referred to the Ocular Surface Laboratory (OSL) for an opinion on optimal management of her condition. Experiencing constant burning and grittiness symptoms, and with relief only when sleeping, RM found her quality of life had deteriorated and her ability to function at work for a full day, without severely curtailing her activities, was impaired. Computer work was described as difficult and prolonged screen use, impossible. Any requirement to attend meetings in air-conditioned rooms caused significant concern and she would often have to leave early on account of debilitating symptoms. In the 6 months prior to referral to the OSL, RM had trialled an extensive range of lubricant eye drops, had been prescribed a course of doxycycline (50 mg daily for 12 weeks) and had been prescribed intermittent courses of topical steroids (prednisolone acetate 0.12 % ophthalmic emulsion by day and dexamethasone 0.1 % ointment at night) and topical antibiotics (chloramphenicol). RM reported that these products did not appear to have made any difference to the symptoms she experienced and, indeed in some cases, had exacerbated her symptoms. On referral, RM was performing twice daily lid hygiene and her aqueous deficiency was being managed, as instructed by her ophthalmologist, with punctal occlusion (Sharpoint Silicone Plugs, InterMed Medical Ltd., NZ), twice daily topical cyclosporin emulsion (0.2 %) (Optimis Pharmacy, Penrose, Auckland, NZ) and non-preserved topical lubricants, as required (Systane Ultra, Alcon and LacriLube ointment, Allergan, at night).
8.1.2 Evaluation
At her first OSL visit, RM’s eyes were visibly inflamed, and, on detailed questioning, she reported that in addition to ocular irritation symptoms, she experienced significant oral dryness symptoms and an apparent inability to reflex tear under usual circumstances. A comprehensive battery of tests evaluating ocular surface health and function was thus performed in an attempt to ascertain the cause of RM’s distressing discomfort.
Subjective assessment of established symptoms and risk factors for dry eye, as well as recently experienced symptoms, was undertaken with the McMonnies Dry Eye Questionnaire and the OSDI (Ocular Surface Disease Index), respectively (Nichols et al. 2004; Schiffman et al. 2000). High scoring on both dry eye questionnaires was indicative of severe dry eye symptoms. Non-invasive objective testing demonstrated the presence of a tear meniscus with some irregularity along the length of the lid margin and a modest central tear meniscus height of 0.1 mm. Phenol red thread (PRT) and non-anaesthetised Schirmer testing also showed reduced lacrimal gland function, implicating aqueous deficiency as a contributor to the dry eye status in this case.
Evaporative dry eye was also confirmed through evaluations of the tear lipid layer by interferometry (Keeler Tearscope Plus™). This highlighted an intermittently visible lipid layer that would be classified as an absent/open meshwork pattern (Guillon and Guillon 1993), equivalent to a lipid grade of 0/1. Correspondingly high tear evaporation rates (Delfin Vapometer, Finland) and tear osmolarity (TearLab, USA) and low non-invasive break-up times (Keeler Tearscope Plus™, UK) were recorded in both eyes. Slit lamp examination of the eyelid margins revealed signs typical of MGD with lid margin thickening, mild telangiectasia and marked keratinisation along the lid margin and over the orifices of the meibomian glands, particularly in the lower eyelids. Mild crusting of the eyelashes, characteristic of staphylococcal blepharitis, was also observed, predominantly on the upper eyelids.
Infrared meibography (SDZ Electronics, Auckland, NZ) confirmed limited meibomian gland drop out, with mild irregularity of gland morphology in the upper eyelid and evidence of truncation and moderate inspissation of the inferior glands (Fig. 8.1). Manual gland expression with the aid of a posteriorly placed Mastrota paddle (OcuSoft, USA) yielded minimal discharge from the glands.
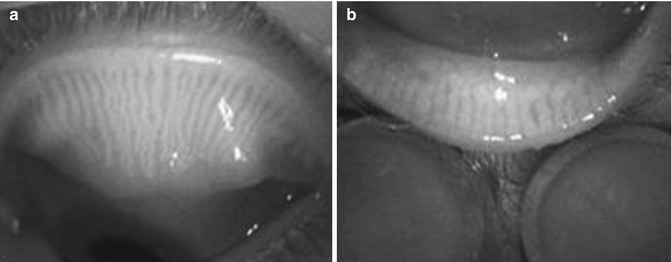
Fig. 8.1
(a) Upper lid meibography. (b) Lower lid meibography
RM’s corneal integrity appeared relatively unaffected by her tear film condition, as confirmed by fluorescein and lissamine green staining. However, there was moderate conjunctival staining with lissamine green in the inter-palpebral zone, particularly nasally, indicating the presence of dead or devitalised cells, or cells devoid of surface glyco-calyx, rendering them hydrophobic in nature (Hamrah et al. 2011).
8.1.3 Management
A staged approach to dry eye management was implemented, in recognition of the need to adopt a multifaceted approach to ameliorating symptoms arising from a multifactorial condition. The breadth of tear film and ocular surface features, found to be compromised in this patient, indicated a diagnosis of combined aqueous deficiency and evaporative dry eye. The approaches by which these aspects were addressed are described in turn.
8.1.3.1 Aqueous Deficiency
The combination of punctal occlusion, topical cyclosporin (0.2 %) and topical lubricants prescribed by RM’s ophthalmologist was, at the time of referral, well tolerated by the patient and was proving sufficient to maintain a modest volume tear meniscus. The management plan for this aspect was not altered, therefore, particularly in light of reported sensitivities to a number of eye products previously, including a lipid/aqueous combination product. The account of symptoms of dry mouth, as well as dry eye, however, suggested the possibility of underlying systemic disease and prompted serological evaluation, to test for auto-antibodies pertinent to Sjögren’s syndrome. These included rheumatoid factor (RF), anti-nuclear antibodies (ANA), anti-SS-A/Ro and anti-SS-B/La. While RM tested sero-negative to these antibodies, at this time, it was recognised that unequivocally discounting a diagnosis of Sjögren’s syndrome was not justified. Antibodies against SSA/Ro are identified in only around 50 % of patients with Sjögren’s syndrome, while antibodies against SSB/La are found in even fewer, around 30 % of patients with Sjögren’s syndrome (Huo et al. 2010). Fractionally borderline results for some of the antibodies in RM’s case indicated that repeat evaluation in the future might be warranted.
8.1.3.2 Evaporative Dry Eye
With serological testing underway, the next step following referral to the Ocular Surface Laboratory was to direct treatment towards RM’s meibomian gland dysfunction and its sequelae. On presentation, RM had been performing regular, twice-daily lid cleansing with a commercial lid preparation, followed by 10-min, warm compress treatments with a microwave-heated wheat bag, according to the advice of her ophthalmologist. Subjectively RM reported modest symptomatic relief from these treatments. After confirming appropriate lid cleansing, warming and expression techniques were being performed by RM; further advice was provided with regard to environmental exposure. The modification to the environment recommended in this case involved, not only minimising exposure to low relative humidity environments created by air conditioning and exposure to high air flow environments but also avoiding exposure to airborne chemicals with the potential to destabilise the tear film. RM described having worked in a building situated adjacent to a vehicle paint-spraying site where exposure to noxious fumes from paint and associated chemicals was a regular occurrence. Paint thinner, for example, is primarily a mixture of aliphatic hydrocarbons, the vapours of which are recognised to induce conjunctival and corneal irritation and inflammation (Bulbulia et al. 1995). Goggles that create a seal around the skin protect the local environment which can help with maintaining higher levels of moisture around the exposed ocular surface (Alex et al. 2013; Korb and Blackie 2013b) and can also reduce exposure to airborne irritants. Spectacles with foam inserts perform a similar function, with superior cosmetic acceptability, and therefore were recommended in this instance (http://www.7eye.com/) and resulted in symptomatic improvement. Interestingly, in this case, the patient’s subsequent decision to change her job made a further noticeable difference to the severity of her ocular discomfort symptoms, corroborating the belief that airborne pollutants were a significant factor in exacerbating her dry eye condition.
RM’s low-lipid delivery state was deemed to be the result of obstruction of the gland orifices due to significant keratinisation that could be observed extending onto the lid margin surface (Fig. 8.2a). Hyperkeratinisation of the meibomian ductal system is recognised to be a core mechanism in the development of obstructive MGD (Henriquez and Korb 1981; Knop et al. 2011).
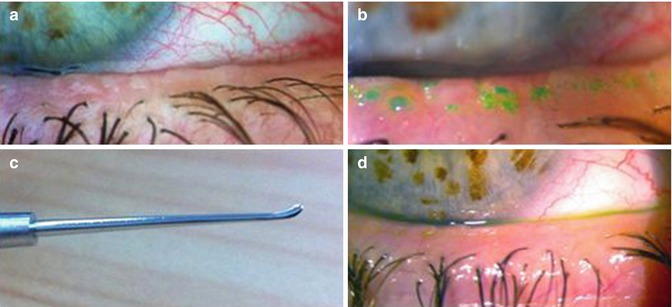
Fig. 8.2
(a) Lower lid hyperkeratinisation; (b) hyperkeratinisation stained with lissamine green; (c) golf club spatula for debridement; (d) lid quality post-debridement
The decision was made to debride the lid margin, in an effort to facilitate egress of the meibomian fluid from the inferior glands (Korb and Blackie 2013a). Topical anaesthesia of the eyelid margin with oxybuprocaine 0.4 %, (Bausch & Lomb) was followed by staining with lissamine green (Fig. 8.2b) to highlight the keratinised areas. Utilising the magnification of the slit lamp, the surface of the lid margin was carefully debrided with a golf club spud (Fig. 8.2c), and the excess keratinised material gently removed. The resulting lid margin profile was significantly smoother as seen in Fig. 8.2d, and the number of glands yielding secretion markedly increased. To date, this improvement has been maintained for over 8 months, post-treatment.
Debridement was thus successful in facilitating meibum outflow from the glands, but, somewhat disappointingly, it was observed that the lipid layer created, following debridement, was of poor quality and the tear film lacked stability, as indicated by a non-invasive break-up time of less than 4 s. The abnormal coloured fringes that were visible (Fig. 8.3a) suggested the presence of lipid globules amidst areas of little or no lipid cover (Guillon and Guillon 1993). Without confluence, such a layer is believed incapable of performing its required function of inhibiting tear evaporation (Craig and Tomlinson 1997).
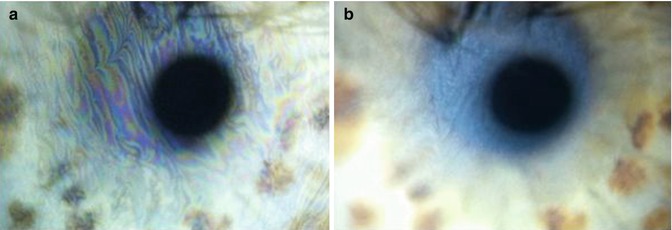
Fig. 8.3
(a) Non-confluent lipid cover pre-omega-3 therapy, grade 0. (b) Confluent lipid layer post-omega-3 therapy, grade 2/3
A means of modifying the lipid quality was therefore sought. Low-dose doxycycline taken over an extended period (e.g. 50 mg daily for 2–3 months) is a well-established therapy for improving gland function in MGD (Sobolewska et al. 2014) and was thus considered as a potential therapy. Reflecting their anti-inflammatory rather than anti-bacterial properties, low-dose tetracyclines improve lipid quality on account of their ability to suppress the production of the bacterial lipases which otherwise serve to destabilise the tear film in MGD (Dougherty et al. 1991). Our patient, however, had not tolerated doxycycline well during a previously prescribed course and was reluctant to commence further doxycycline treatment. It was elected therefore to adopt a more natural approach to lipid layer alteration, through diet. Essential fatty acid supplementation has recognised anti-inflammatory effects throughout the body, due competitive inhibition, between the omega-3 fatty acid, eicosapentaenoic acid, and omega-6 fatty acid, arachidonic acid, to synthesise mediators with anti-inflammatory properties over potentially harmful inflammatory mediators (James et al. 2000). Mounting evidence suggests positive effects in MGD from dietary supplementation with omega-3 fatty acids, with a recent randomised, placebo-controlled, trial describing improvements in symptomatology as well as in clinical signs such as lid margin inflammation, meibomian gland expression, tear film stability and tear production (Olenik et al. 2013).
Such improvements were, indeed, realised following a conscious effort by RM to increase her omega-3 intake, both naturally from the regular consumption of smoked salmon and in the form of a nutritional supplement. After an 8-week period, her non-invasive break-up time was noted to have increased by around 3.5 s, in tandem with an improvement in her lipid layer quality to a marmoreal/wave combination pattern (thickness around 60–80 nm), implying presence of a confluent lipid layer (Fig. 8.3b) (Guillon and Guillon 1993). Tear evaporation rate was correspondingly decreased.
A concurrent reduction in bulbar conjunctival hyperaemia (Fig. 8.4) and symptoms was also noted, following the lid margin debridement and the described change in diet.
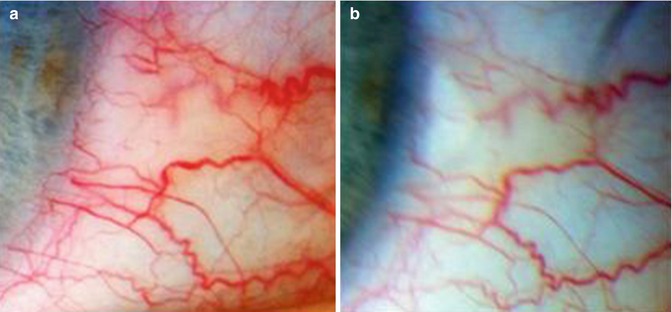
Fig. 8.4
Bulbar hyperaemia pre- (a) and post (b)-lid margin debridement and omega-3 treatment
Following the dietary changes, RM’s tear film and ocular surface condition was observed to stabilise and symptoms were described as tolerable, although not fully ameliorated. With the hope of achieving further symptomatic relief, RM thus opted to engage in an opportunity to trial treatment with the E > Eye Intense Pulsed Light (IPL) device for MGD within the Ocular Surface Laboratory. The potential benefits of IPL technology, as an MGD therapy, were discovered during cosmetic IPL skin treatments for patients with acne rosacea, where it was noted that individuals with associated ocular rosacea experienced concurrent improvements in their dry eye condition following IPL treatment on the upper cheek area of the face (Mark et al. 2003). Toyos in the United States is a firm proponent of IPL for MGD on the basis of his personal clinical findings (Toyos et al. 2005). However, the reports of these open-label treatments require validation with randomised, placebo-controlled trials to confirm the true benefit. Certainly, from an anecdotal perspective, patient RM has experienced further improvement in meibomian gland function since commencing monthly IPL treatments, with both immediate and sustained increases in lipid layer quality. She currently exhibits an amorphous/normal coloured fringe pattern, corresponding to lipid grade 4/5 (Fig. 8.5), and this has been associated with a reduction in ocular discomfort symptoms.
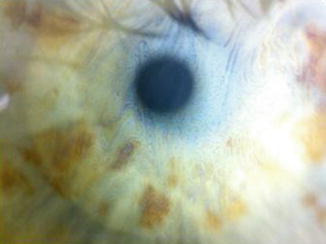
Fig. 8.5
Confluent lipid layer, post-IPL, grade 4/5
At the present time, RM is enjoying significantly reduced irritation symptoms, in comparison to those on presentation, and is delighted with the reduction in her red eye appearance. Her quality of life has improved significantly, such that she can now work a full day without marked restrictions on her activities. She continues with cyclosporin therapy, punctal occlusion and artificial lubricants as required, supplemented with ointment at night. Due to hypertrophy of the punctum secondary to silicone punctal plugs, which was causing intermittent mechanical irritation, a more permanent solution to punctal occlusion has recently been sought with cautery to replace the silicone plugs. Lid hygiene, warm compress therapy and manual expression form part of a daily routine for RM. These ongoing strategies, applied in conjunction with lid margin debridement, dietary regulation and monthly IPL treatments, have, in the words of this individual, ‘given her back her life’.
8.2 Dry Eye Case Report 1
Colin Chan12
(12)
University of Sydney, Vision Eye Institute, 270 Victoria Ave Chatswood, Sydney, 2067, Australia
A 56-year-old self-employed lady was referred by her optometrist with a several year history of dry eye and contact lens tolerance issues. Previous treatments had included TheraTears drops, TheraTears flaxseed and fish oil supplement, Zaditen and warm compresses, all of which had provided some relief. Serology testing was negative for Sjögren’s syndrome. She ultimately wanted to consider a refractive lens exchange because of her contact lens issues and her unsuitability for laser given her underlying dry eye condition.
Initial slit lamp findings were mild sub-tarsal papillary changes and limbal injection in both eyes. There was significant lid margin disease and insippation of the meibomian glands; tear BUT was 3 s in both eyes. Manifest refraction in the right eye was +2.75/−0.25 × 125 giving 6/7.5 and in the left was +2.75/−0.50 × 180 yielding 6/7.5. Corneal topography showed regular with the rule astigmatism in both eyes. A diagnosis of dry eye secondary to meibomian gland dysfunction and contact lens keratoconjunctivitis/hypersensitivity was made.
She responded well to an initial pulse of FML tds for 3 weeks. Zaditen tds was reinitiated and the patient asked to continue the omega-3 supplements and warm compresses. TBUT increased to 5 s in both eyes with a decrease in limbal injection.
The patient represented later that year with markedly reduced vision eye and increased irritation especially in the right eye. She stated that things had gotten worse after recent house renovations and a trip to New Zealand. She had worn her contact lenses minimally. Manifest refraction in the right eye was +1.50/−0.75 × 151 yielding 6/45 only and in the left eye +2.25/−0.25 × 86 giving 6/18. There was superior haze in her right cornea with overlying punctuate defects and diffuse nummular opacities in her left eye (Figs. 8.6 and 8.7). Topographies showed induced corneal irregular astigmatism (Fig. 8.8a, b).
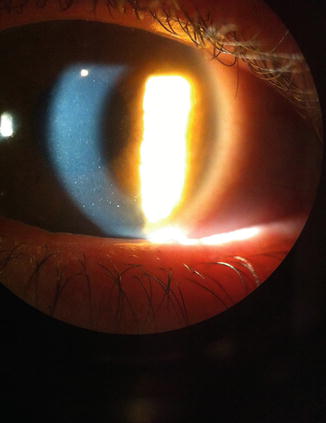
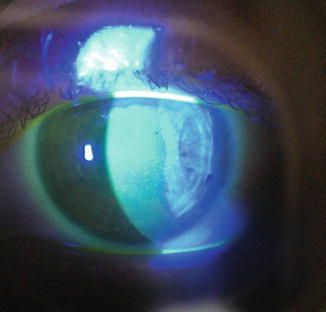
Fig. 8.6
Mild superior corneal haze in right eye
Fig. 8.7




Punctate staining over area of haze typical of nummular or contact lens keratitis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
