Purpose
To evaluate the in vivo capsular apposition to the intraocular lens (IOL) in subjects with high myopia by ultralong-scan-depth optical coherence tomography (OCT).
Design
Prospective observational case series.
Methods
Forty eyes from 40 cataract patients scheduled for phacoemulsification surgery at the Affiliated Eye Hospital, Wenzhou Medical College were studied, of which 20 eyes were highly myopic (axial length >26 mm) and 20 eyes were emmetropic (22 mm < axial length <24.5 mm). All eyes were examined with a custom-built ultralong-scan-depth OCT at 4 hours, 1 day, 7 days, 14 days, and 28 days after surgery.
Results
Anterior capsule contact with the IOL was significantly delayed in highly myopic eyes. Complete apposition of the posterior capsule with the IOL was significantly less common among highly myopic eyes than in emmetropic eyes (4 vs 16 eyes; P = .001). Posterior capsule adhesion to the IOL was inversely correlated with axial length (r = −0.494, P < .001, nonparametric Spearman test). The 3 types of complete adhesive capsular bend configurations observed were classified as anterior adhesion, middle adhesion, and posterior adhesion. Incomplete adhesion patterns were classified as funnel adhesion, parallel adhesion, and furcate adhesion. Five highly myopic eyes had slight posterior capsule opacification (PCO) at the last follow-up, as did 1 emmetropic eye.
Conclusions
Ultralong-scan-depth OCT revealed weak capsular adhesion and incompletely adhesive types of capsular bend in highly myopic eyes. These features presumably increase the likelihood of PCO during the early postoperative period.
Posterior capsule opacification (PCO) is a result of lens epithelial cell proliferation and migration. Even with complete cortical cleanup, PCO remains the most common long-term complication after cataract surgery.
Peng and associates showed that the intraocular lens (IOL) barrier plays an important role in inhibiting lens epithelial cell growth, especially in cases with sufficient cortical cleanup. A series of studies have shown that a sharp optic edge of the IOL and a firm capsule–IOL interaction could inhibit lens epithelial cell proliferation and migration.
Many researchers have focused on the design and material of the IOL, which could promote capsular bend formation and firm contact with the capsule. However, we found few studies evaluating the capsule–IOL interaction in highly myopic eyes.
Nagamoto and associates reported that the contact pressure between the optic edge and the posterior capsule is the primary factor inhibiting lens migration. It is universally accepted that there would be low pressure as long as there is excess length in the posterior capsule. We hypothesize that highly myopic eyes with relatively large capsules may develop a lower contact pressure, which may alter the nature of the capsule–IOL interaction.
In this study, we investigated the capsule–IOL interactions, including anterior and posterior capsule adhesion, configuration of the capsular bend, and the incidence of PCO in highly myopic eyes and emmetropic eyes.
Methods
Patients
This prospective study was performed at the Affiliated Eye Hospital, Wenzhou Medical College, in Zhejiang, China and was approved by the Institutional Review Board/Ethics Committee of Wenzhou Medical College. Informed consent to participate in this research study was obtained from all patients. Practices and research were in accordance with the tenets of the Declaration of Helsinki. The study was registered at www.clinicaltrials.gov ; the clinical trial accession number is NCT01605812 . This prospective study included patients with high axial myopia (high myopia group) and age-matched patients with normal axial length (emmetropia group). All eyes underwent uncomplicated phacoemulsification with a single-piece AcrySof IOL (Alcon, Fort Worth, Texas, USA) for cataract treatment.
The preoperative exclusion criteria included diabetes, history of ocular surgery or inflammation, pupils that could not be dilated over 7 mm after mydriasis, and those who were not available for follow-up. The postoperative exclusion criteria included any surgical complication, an anterior capsule that did not totally cover the IOL, and those who refused to be examined. Eyes with an axial length of 26.00 mm or more were classified to the high myopia group. Eyes with an axial length of 22.00-24.5 mm were classified to the emmetropia group. The axial length measurement was taken before pupil dilation using an IOL Master 5.0 (Carl Zeiss Meditec, Jena, Germany). All measurements were performed by the same technician. The horizontal diameter of the cornea (white-to-white) and anterior chamber depth (ACD) were recorded at the same time.
Surgical Procedures
All surgeries were performed by a single experienced surgeon. Phacoemulsification was performed using a standardized technique. A 2.2-mm clear corneal incision was made, and a continuous curvilinear capsulorrhexis measuring approximately 5.5 mm in diameter was created. The capsulorrhexis overlapped the IOL optic in all cases. After hydrodissection, endocapsular phacoemulsification of the nucleus and aspiration of the residual cortex were performed. IOL implantation into the capsule bag was performed with an injector. The ophthalmic viscoelastic device was removed from the anterior chamber and the capsular bag by coaxial irrigation/aspiration. The haptics of the IOL were adjusted to the vertical position of the capsular bag. For each patient, digital retroillumination images were captured by slit lamp to confirm that the anterior capsule overlapped the optical edge of the IOL.
Intraocular Lens
The IOL used in our study is the single-piece acrylic AcrySof platform (Alcon Laboratories) with a sharp-edge design. Its haptic length is 13.0 mm and its optic zone diameter is 6.0 mm.
Postoperative Measurements With Ultralong-Scan-Depth Optical Coherence Tomography
An ultralong-scan-depth optical coherence tomography (OCT) instrument with ∼7.5 μm axial resolution was used to visualize the entire IOL and its interaction with the capsule. This instrument has been described in detail in previous published studies. Briefly, it uses a custom-designed spectrometer to achieve a depth of 7.3 mm in air. The scan width was set to 8 mm. X-Y cross-aiming was applied to align the scanning position, which was necessary to image the entire IOL and capsule. After full pupil dilation with 1% tropicamide and 2.5% phenylephrine hydrochloride, the subjects were asked to sit in front of the instrument and to look straight at the central red fixation target. The cross-sectional scan was taken from the bottom to the top of the eye when the incident light passed through the IOL center. Thirty-two images were captured during the examination. The capsular adhesion rate was calculated as a completed adhesive capsule–IOL image was found in the 32 images. The longest IOL measured among the images in each examination was used for analysis.
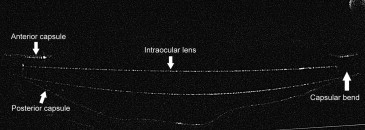
The follow-up examinations were performed 4 hours, 1 day, 7 days, 14 days, and 28 days after the surgery. The capsule–IOL interaction was evaluated in the emmetropic and highly myopic eyes by analyzing anterior and posterior capsule adhesion, configuration of the capsular bend, and contact between the posterior capsule and the posterior edge of the IOL ( Figure 1 ).
PCO was observed using retroillumination by slit lamp at every follow-up visit.
Statistical Analysis
The independent t test was used to compare the differences between the emmetropia and high myopia groups. Fisher exact test was used to compare categorical data. The nonparametric Spearman test was used to analyze the correlation between anterior and posterior capsule adhesion and axis length, anterior chamber depth, and IOL power. P values of less than .05 were considered significant.
Results
Background Statistics
No differences in terms of patient background were found between the emmetropia and high myopia groups, except for anterior chamber depth, axis length, and IOL power ( Table 1 ).
| High Myopia | Emmetropia | P Value | |
|---|---|---|---|
| Patients/eyes (n) | 20/20 | 20/20 | >.999 |
| Mean age (y) | 66.1 ± 8.13 | 63.86 ± 8.61 | .421 |
| Male/female (n) | 3/17 | 5/15 | .118 |
| Left/right eye (n) | 12/8 | 10/10 | .276 |
| Axis length (mm) | 28.84 ± 1.78 | 23.15 ± 0.51 | <.001 b |
| Corneal horizontal diameter (mm) | 11.74 ± 0.50 | 11.88 ± 0.46 | .156 |
| Anterior chamber depth (mm) | 3.63 ± 0.67 | 3.17 ± 0.36 | <.001 b |
| IOL power (D) | 9.78 ± 3.40 | 21.03 ± 2.46 | <.001 b |
a Data are expressed as the means ± standard deviation. Differences between groups were analyzed by independent t test. Categorical data were compared using Fisher exact test.
Anterior and Posterior Capsular Adhesion to the Intraocular Lens
Anterior capsule contact with the IOL was delayed in highly myopic eyes. However, at the last follow-up, most anterior capsules had achieved perfect adhesion with the IOL ( Table 2 ).
| Nasal Anterior Capsule a | Temporal Anterior Capsule | Posterior Capsule a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| High Myopia | Emmetropia | P Value | High Myopia | Emmetropia | P Value | High Myopia | Emmetropia | P Value | |
| 4 hours | 0 (0%) | 4 (20%) | .105 | 0 (0%) | 1 (5%) | >.999 | 0 (0%) | 3 (15%) | .23 |
| Day 1 | 0 (0%) | 12 (60%) | <.001 b | 1 (5%) | 10 (50%) | .003 b | 0 (0%) | 6 (30%) | .02 b |
| Day 7 | 7 (35%) | 18 (90%) | .001 b | 10 (50%) | 16 (80%) | .096 | 1 (5%) | 15 (75%) | <.001 b |
| Day 14 | 17 (85%) | 19 (95%) | .605 | 17 (85%) | 18 (90%) | >.999 | 3 (15%) | 16 (80%) | <.001 b |
| Day 28 | 19 (95%) | 20 (100%) | >.999 | 18 (90%) | 19 95%) | >.999 | 4 (20%) | 16 (80%) | <.001 b |
a Differences between high myopia and emmetropia were analyzed by Fisher exact test.
b Statistically significant differences among groups ( P value < .05).
Table 2 summarizes the percentage of eyes with first found perfect adhesion between capsule and IOL optic at each follow-up in both groups. Three emmetropic eyes displayed complete attachment of the posterior capsule and IOL immediately after surgery. Fisher exact test showed significant difference between highly myopic and emmetropic eyes in terms of posterior capsule–IOL adhesion when comparing measurements taken at 7 days, 14 days, and 28 days of follow-up. On the 28th postoperative day, the posterior capsules were completely attached to the IOL in only 4 eyes in the high myopia group, which was significantly less than in the emmetropia group ( P = .001).
As shown in Figure 2 , both the anterior and posterior capsular adhesions were obviously delayed in the highly myopic eyes during the follow-up.
The time points where the anterior and posterior capsular adhesion rates in emmetropic eyes were over 80%, respectively, were chosen to analyze the correlations between capsule adhesion, axis length, anterior chamber depth, and IOL power. We selected the seventh day and 14th day to correlate the ocular parameters with anterior and posterior adhesion, respectively ( Table 3 ).
| Eye Parameter | Anterior Capsular Adhesion b (Nasal) | Anterior Capsular Adhesion b (Temporal) | Posterior Capsular Adhesion c | |||
|---|---|---|---|---|---|---|
| r | P Value | r | P Value | R | P Value | |
| AL (mm) | −0.371 | .003 d | −0.271 | .035 d | −0.494 | <.001 d |
| ACD (mm) | −0.171 | .187 | −0.041 | .753 | −0.358 | <.001 d |
| IOL (D) | 0.330 | .009 d | 0.212 | .101 | 0.448 | .005 d |
a The correlation analysis was conducted by the nonparametric Spearman test.
b The anterior adhesion of eyes at the seventh day was chosen to analyze the correlation with eye parameters.
c The posterior adhesion of eyes at the 14th day was chosen to analyze the correlation with eye parameters.
d Statistically significant differences among groups ( P value < .05).
Types of Capsular Bend Formation
Various configurations of capsular bend were observed at the last follow-up. As shown in Figure 3 , 3 types of capsular bends with complete adhesion were found. Anterior adhesion was observed in most cases (70%). Four capsular bends in highly myopic eyes were observed with middle adhesion, whereas 1 was found in emmetropic eyes. Only 1 nasal capsular bend was found with posterior adhesion in a highly myopic eye ( Table 4 ).



