Bronchoscopy
Introduction
Bronchoscopy is the visual examination of the tracheobronchial tree. Both flexible and rigid instruments are available for this procedure. Rigid bronchoscopy permits instrumentation of the airway and allows for continued ventilation. Flexible bronchoscopy, while giving better visualization of the more distal bronchi, does not allow for easy foreign body removal and cannot be used to maintain an airway unless it is passed through or alongside of an endotracheal tube. However, the laryngeal lumen requirement for this arrangement precludes its use in small children. Direct laryngoscopy (either flexible or rigid) always precedes bronchoscopy.
Indications
Foreign body, lesions in the trachea or bronchi, or mucus plugging of the bronchi are indications for bronchoscopy.
Preoperative Evaluation
Anteroposterior and lateral chest radiographs may be helpful in the preoperative evaluation in the child undergoing bronchoscopy. Computed tomography (CT) may prove helpful in localizing the disease process. Indirect laryngoscopy is useful in the preparation for the endoscopic examination.
34-1 Flexible Bronchoscopy
Introduction
Flexible bronchoscopy is the procedure best suited to viewing respiratory dynamics of the trachea and bronchi and details of the distal airway.
Operative Technique
1. Flexible bronchoscopy occurs after successful flexible direct laryngoscopy has been performed.
2. As preparation is made to pass the bronchoscope through the vocal cords, the child is paralyzed or the anesthesia level is deepened sufficiently to prevent laryngospasm.
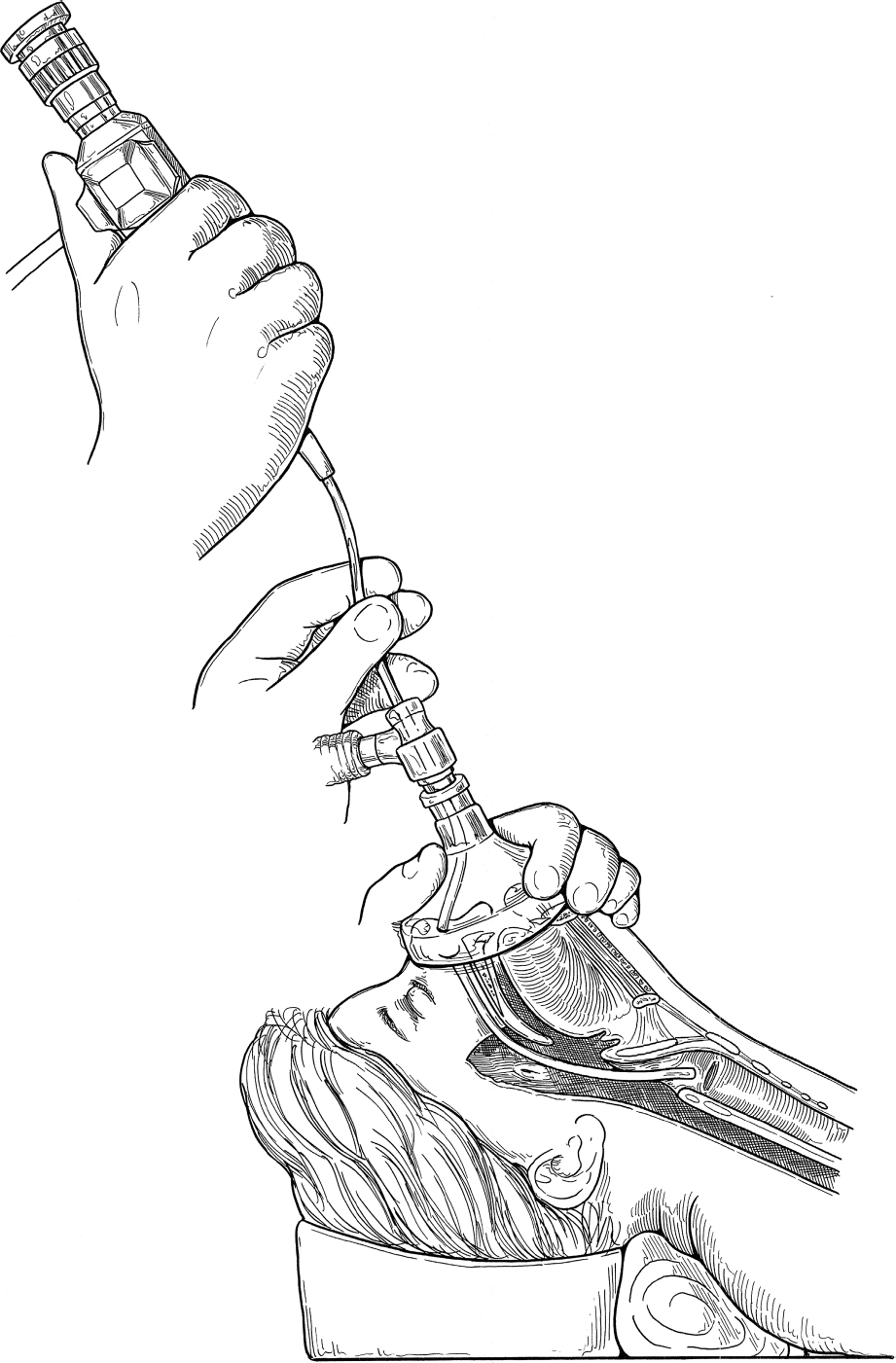
3. The bronchoscope is advanced into the subglottic space and then into the trachea and bronchi (Fig. 34.1).
4. Usually the anesthesiologist can maintain an adequate fit with the mask and adequate ventilation can be maintained. However, if the bronchoscope is too snug in the subglottic or laryngeal area, ventilation may be limited. In this case, the bronchoscope must be withdrawn periodically to the level of the laryngeal inlet so that adequate ventilation can be maintained.
5. The bronchoscope is advanced so that the right and left bronchi are inspected in an orderly manner.
6. The bronchoscope is withdrawn and ventilation maintained by the anesthesiologist utilizing a mask or endotracheal tube, depending on the situation.
Complications
1. Laryngospasm
2. Glottic edema
3. Dental trauma