For decades, the only available “off-the-shelf” injectable fillers available were Zyplast and Zyderm. Their impact on the upper face was relatively limited, primarily to the glabellar region. The thin-skinned regions of the periorbita and dynamic regions of the upper face also limited the durability of the product. The last few years have brought several new injectable soft tissue fillers to the market in the United States and a renewed interest in the use of autologous fat. These are being used not only as simple line fillers, but as volume replacement materials, and have provided new perspectives in the management of the aging face.
This article reviews the current injectable agents and techniques used in the management of the aging face and provide current concepts for their application.
Botulinum neurotoxin
First used by Dr. Allen Scott of San Francisco in the 1980s, botulinum neurotoxin (BTX) showed promise in laboratory chick models for selective weakening of treated muscles and soon thereafter was used in the management of strabismus . Under the trade name, Oculinum, this product was picked up by Allergan Inc (Irvine, CA), primarily an ophthalmic pharmaceutical company, for this and other neuromuscular disorders around the eye.
Botulinum toxin is found in nature in seven serotypes (A through G) defined by their specific biologic action in cleaving the particular proteins in the active transport of acetylcholine into the neurosynaptic cleft responsible for muscle contraction (and other autonomic functions) . These naturally occurring proteins were described originally as toxins caused by the illness botulism, which is associated with ingestion of large amounts of Clostridium botulinum –contaminated food stuffs. They are better described, with respect to their now widespread medical use, as neuromodulators . Their distinct beneficial action is selective weakening, relaxation, or paralysis of treated muscles or muscle groups. By selective weakening of certain hypertrophic muscle groups in the face and neck, unwanted lines and facial expressions can be suppressed or even eliminated.
Although the B serotype (Myobloc; Solstice Neurosciences, San Francisco, CA) neuromodulator has shown benefit in the treatment of hyperfunctional frown lines, its benefit under current formulations is limited by the shorter duration of effect of the product . This leaves the aesthetic practitioner with the A neurotoxin.
The A serotype has shown the longest duration of effect (90 to 120 days) and least discomfort with injection. The “Coca-Cola” of the available A serotype neuromodulators is Botox (Allergan, Inc). The techniques and dosages described herein are in reference to the use of this medicinally original botulinum neuromodulator, which now has a demonstrated safety and efficacy record of more than 15 years.
Reloxin (Inamed Inc, Santa Barbara, CA), known as Dysport in Europe, is in current phase III US Food and Drug Administration (FDA) clinical trials and shows promise as does Purtox (Mentor Corp, Santa Barbara CA), which is in early-phase FDA trials.
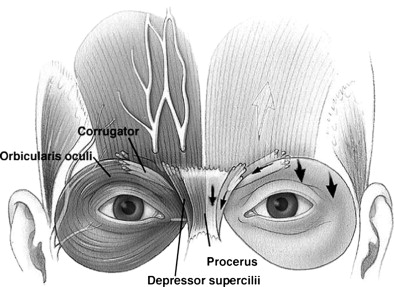
An understanding of how to use BTX relies on a clear understanding of the facial muscular anatomy ( Fig. 1 ).
Although many techniques and surface points of injection have proven effective, it is clear that optimal response with minimal effective dosages requires precise placement in the selected muscle or muscle group.
The author has shown the upper facial anatomy in controlled large population anatomic studies . The interest in lower facial applications reinforces the need for a fundamental understanding of this muscular anatomy . It is clear, however, that because of diffusion effects and the relative safety of BTX, the variability in points of injection and dosages has not significantly reduced the product’s overall satisfactory clinical results. In the author’s opinion, required dosages for a given anatomic area can be reduced by precise localization and direct injection into the targeted muscle or muscle groups. Diffusion is helpful for those who lack a solid understanding of muscle location and general anatomy. In some cases, this has been perpetuated by inaccurate published anatomic drawings.
It is imperative to keep in mind not only the specific muscle locations when providing neuromodulator treatment, but also the functional interrelationships of the muscle action. Many of these act as antagonist-protagonists in the position of the brow (see Fig. 1 ). The use of BTX in general has evolved with experienced and thoughtful injectors from a simple wrinkle treatment to means of reshaping, contouring, and softening the facial features associated with aging and the stigmata of the frowning, angry, or worried facial form.
The glabellar complex
Furrows created at the base of the nose (radix) are created by the procerus muscle, which is statistically larger in women than men. Although this muscle has limited action as a brow depressor, it is a powerful “wrinkler” of the nose, which, with chronic activity, creates deep furrows. Many patients seeking treatment for vertical glabellar furrows have very limited procerus activity and do not require concurrent treatment. Not all patients are the same; thus, treatment formulas that are universal are wasteful and unnecessary. Three to five units placed in one or two aliquots in the area of radix are sufficient for most patients to achieve a satisfactory reduction in procerus activity (see Fig. 1 ).
The corrugator supercilii and its accompanying depressor orbicularis oculi muscle are clinically indistinguishable. Their anatomy is poorly understood as it relates to that position. In contrast to many schematic or figurative diagrams showing the tail (or insertion) of the corrugator muscle one centimeter above the brow, the corrugator in the majority of patients follows the course of the eyebrow and delicately interdigitates with the orbicularis oculi muscle laterally and the frontalis muscle superiorly. Thus, injections well above the midpupillary brow are of little value in targeting corrugator function and primarily disable lower portions of frontalis muscle. Such injections would be expected to result in medial brow ptosis.
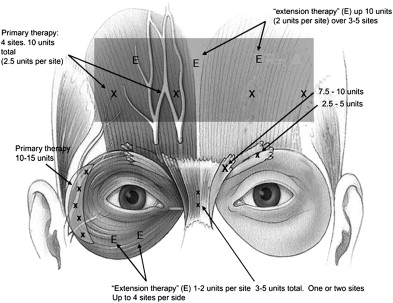
Proper targeting requires the bulk of dosing for the corrugator at the clubhead of the eyebrow. At the author’s institution, we use a minimum of 7.5 units in this area and 2.5 units in the scant muscle of the lateral brow to address “recruitment” of this lateral portion and some of the horizontally oriented orbicularis. These injections are directed at or slightly (within 1 or 2 mm) above the level of the eyebrow as the musculature descends with the aging ptotic brow ( Fig. 2 ).
The lateral orbital region
The orbicularis oculi (O.o.) muscle and the “crow’s feet” are also seemingly poorly understood. Although primary emphasis is focused by many on the softening of lines in this area, the lateral O.o. is the most powerful depressor of the brow and, as such, has the greatest potential with neuromodulation to reshape the upper face. The emphasis on lateral orbicularis muscle is paramount because the muscle is a sphincter, and its superior and inferior portions create vectors of force that are in the horizontal plane. Treating these regions provides for softening vertically oriented supraorbital lines and “crepey” lines in the infraorbital region. Contrary to popular belief, in the author’s opinion, the treatment of these areas has limited impact on horizontal brow position.
Treatment strategies, therefore, are stratified (although not mutually exclusive) around treatment of hypertrophic lines and reshaping the brow. Although single-point limited dosing at the lateral brow margin may provide some benefit in elevating brow position, it is advisable to keep in mind the entire lateral O.o. is responsible for brow depression, and, as shown in the author’s previous work treatment of this large and powerful depressor can have a profound impact on brow position. In contrast, the supra and infraorbital lines of expression can be substantively affected by small doses in these regions. Concerns about effects on extraocular movements and the elevators of the lip have not proven problematic in our experience in which lower eyelid injections are targeted outside the orbital rim and in the immediate subcutaneous plane.
Starting doses for the lateral orbital region are in the range of 10 units per side and can go quite comfortably as high as 20 units per side, in our experience, without impact on sphincteric function. Small 2.5-unit aliquots are placed at roughly 1-cm intervals in a “half-moon” configuration from the infralateral brow to the inferior extent of horizontally oriented lines (see Fig. 2 ). Extension for the crepey skin in the infraorbital region is easily done up to the area of the nasojugal groove.
The forehead
The forehead is probably the most variably and poorly treated region of the upper face with neuromodulators. Injectors must balance the benefit of hyperfunctional line improvement with relaxation of the only brow elevator, the frontalis, and attendant ptosis of the brow that will occur. Dosages exceeding 20 units in the forehead are rarely warranted, in the author’s opinion, because the trade of complete line effacement is not worth the side effect of noticeable brow ptosis.
In addition, many strategies for treating the forehead region leave lateral frontalis muscle action unattenuated, resulting in a “Dr. Spock–like” forehead deformity ( Fig. 3 ) that is both a hallmark of treatment and unattractive. The key to success in forehead treatment is modest dosing (enough to soften the lines with minimal impact on brow position) and uniform distribution of injections to avoid asymmetries and an artificial appearance of brow position.




