Purpose
To determine the prevalence, associated factors, and surgical outcomes of patients with body dysmorphic disorder in an oculofacial surgery practice.
Design
Retrospective cross-sectional analysis of a consecutive case series.
Methods
Participants consisted of a consecutive series of 728 patients who completed the Dysmorphic Concern Questionnaire in an oculofacial surgery practice at The Cole Eye Institute between November 2013 and June 2014. A questionnaire score ≥9 was used as a positive screen for body dysmorphic disorder. Three control patients scoring ≤8 in the same month were randomly selected for each positive-screening patient. Main outcome measures included number of reoperations, surgical complications, and follow-up visits; preoperative and postoperative pain scores; and the technician word count. Categorical variables were analyzed with Pearson χ 2 tests or Fisher exact tests, while continuous variables were analyzed with Wilcoxon rank sum tests or t tests.
Results
A total of 728 patients completed the questionnaire and 50 (6.9%) scored 9 or more. Using a confidence interval of 95%, patients in the positive questionnaire screen group were younger ( P = .004), had more eyelid surgeries ( P = .007), experienced higher rates of complications after surgery ( P = .002), reported higher postoperative pain scores ( P = .034), required more reoperations ( P = .050), and had a higher technician word count compared to the control group ( P = .003).
Conclusions
The prevalence of body dysmorphic disorder in an oculofacial surgical setting matches reports from other surgical specialties, and is significantly higher than in the general population. Patients screening positively for body dysmorphic disorder tend to have higher postoperative pain scores and more postoperative complications.
Body dysmorphic disorder is defined as excessive preoccupation with an imagined or slight physical deformity, accompanied by repetitive behaviors such as mirror checking, skin picking, excessive grooming, and reassurance seeking. It often results in profound life disturbances, and the presence of body dysmorphic disorder inversely correlates with postoperative satisfaction and quality of life. A past survey of aesthetic surgeons estimated that 2% of their patients had body dysmorphic disorder. Although this estimation compares similarly to the general population rates of 0.7%–2.4%, recent studies suggest a higher prevalence of body dysmorphic disorder in general dermatologic patients (6.7%), patients in a cosmetic dermatologic practice (14.0%), patients in a maxillofacial setting (10%), and patients seeking rhinoplasty (21%).
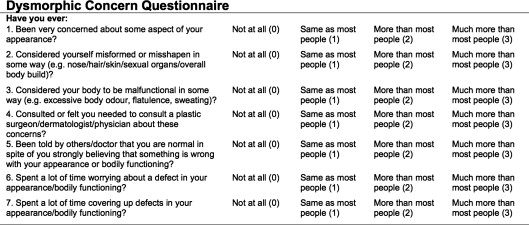
Until recently, finding a convenient screening tool for body dysmorphic disorder for the clinical setting has proven difficult. The Body Dysmorphic Disorder Examination is a reliable diagnostic tool for body dysmorphic disorder, but it consists of a 34-item clinician-administered examination that may require 30 minutes to complete. Only 2 shorter questionnaires, the Body Dysmorphic Disorder Questionnaire–Dermatology Version and the Dysmorphic Concern Questionnaire, have been validated in a surgery practice setting. The Dysmorphic Concern Questionnaire consists of 7 self-reported questions that measure a patient’s concern about his or her physical appearance on a scale from 0 to 3, with a total maximum score of 21. A Dysmorphic Concern Questionnaire cutoff point of greater than or equal to 9 has been validated as a clinical screening tool for body dysmorphic disorder, providing a specificity of 90.6% and a sensitivity of 96.4%. Although the Dysmorphic Concern Questionnaire has been validated in other non–psychiatric clinic settings, it does not provide a Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-V) diagnosis.
A series of 3 patients has been reported in an oculoplastic surgery practice. This single report did not quantify the prevalence, the characteristics, or the surgical outcomes of body dysmorphic disorder patients in an oculofacial plastic surgery practice. In order to identify patients with body dysmorphic disorder, we have been including the Dysmorphic Concern Questionnaire in the evaluation of all patients since 2013. We sought to determine the prevalence and characteristics of body dysmorphic disorder in an oculofacial plastic surgery practice and to determine the surgical outcomes in such patients.
Methods
This study was a cross-sectional analysis of a consecutive case series. We reviewed the medical records of all patients who completed the Dysmorphic Concern Questionnaire in the clinical practice of 1 surgeon, Julian D. Perry (J.D.P.), at the Cole Eye Institute between November 20, 2013 and June 18, 2014. All new patients were offered the Dysmorphic Concern Questionnaire during the study period. Data collected from medical records included the following: Dysmorphic Concern Questionnaire score, age upon survey, sex, ethnicity, height, weight, body mass index (BMI), marital status, number of children, number of previous facial surgeries, number of previous cosmetic surgeries, number of previous eyelid surgeries, number of other surgeries, number of Botox/filler/other procedures, number of previous doctors visited, and whether or not the patient underwent surgery by 1 of the authors (J.D.P.). For those patients who underwent surgery, charts were reviewed for reoperations, surgical complications, number of follow-up visits, preoperative and postoperative pain numerical rating scale scores, and the technician word count as a proxy for postoperative complaints during first follow-up visit. Intraoperative complications were determined from the operative note. A postoperative complication was defined as an unexpected problem requiring more than topical or intralesional medication, or a persistent, bothersome, and unexpected structural, visual, or neurologic deficit. The Cleveland Clinic Foundation Institutional Review Board approved this study. Informed consent was obtained from the patients, and the study is in accordance with HIPAA regulations.
As part of each standard initial patient evaluation, the technician administered the 7-item Dysmorphic Concern Questionnaire by asking the patient to respond to each verbal question using the following answers: not at all (0), same as most people (1), more than most people (2), and much more than most people (3). The technician recorded the scores in the patient chart. Patients completed the questionnaire only at the initial visit. A Dysmorphic Concern Questionnaire score of ≥9 was defined as a positive screen for body dysmorphic disorder. For each positive-screening patient, 3 control patients scoring ≤8 in the same month were randomly selected. Those positive-screening patients and controls that underwent surgery by 1 of the authors (J.D.P.) were analyzed separately. Technician word count was defined as the number of words in the technician-entered history of present illness in the electronic medical record. Technicians were not masked, and several different technicians performed the Dysmorphic Concern Questionnaire. The Dysmorphic Concern Questionnaire is depicted in the Figure .
Categorical variables were summarized using frequencies and percentages, while continuous variables were summarized using medians and quartiles (for those variables that were not normally distributed) or means and standard deviations (for those variables that were normally distributed). Differences between groups on categorical factors were analyzed with Pearson χ 2 tests or Fisher exact tests, while differences between groups on continuous factors were analyzed with Wilcoxon rank sum tests (non-normal distributions) or t tests (normal distributions). All analyses were performed using SAS software (version 9.1; SAS Institute, Cary, North Carolina, USA). An overall significance level of ≤.05 was assumed for all analyses.
Results
A total of 728 patients completed the Dysmorphic Concern Questionnaire between November 2013 and June 2014. Fifty patients (6.9%) scored 9 or more on the Dysmorphic Concern Questionnaire. Selecting 3 control patients for every positive Dysmorphic Concern Questionnaire screening patient provided a control group of 150 patients. A second dataset that consisted of only those patients who were operated on by one of the authors (J.D.P.) contained 95 patients (72 controls and 23 cases).
There was no statistically significant difference in sex, race, or marital status between the positive Dysmorphic Concern Questionnaire screen group and the control group. Table 1 shows the relationship between group and categorical variables for the entire cohort.
| Factor | Level | Total | Case | Control | P Value | ||
|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | ||||
| Sex | .27 | ||||||
| Male | 73 | 15 | 30.0 | 58 | 38.7 | ||
| Female | 127 | 35 | 70.0 | 92 | 61.3 | ||
| Race | .41 F | ||||||
| American Indian/Alaska | 1 | 0 | 0.00 | 1 | 0.67 | ||
| Asian | 3 | 0 | 0.00 | 3 | 2.0 | ||
| Black | 22 | 6 | 12.2 | 16 | 10.7 | ||
| Declined | 1 | 0 | 0.00 | 1 | 0.67 | ||
| Hispanic | 1 | 1 | 2.0 | 0 | 0.00 | ||
| Multiracial | 1 | 1 | 2.0 | 0 | 0.00 | ||
| White | 169 | 41 | 83.7 | 128 | 85.3 | ||
| Unknown | 1 | 0 | 0.00 | 1 | 0.67 | ||
| Marital status | .24 | ||||||
| Divorced | 20 | 5 | 10.0 | 15 | 10.0 | ||
| Married | 114 | 23 | 46.0 | 91 | 60.7 | ||
| Single | 43 | 16 | 32.0 | 27 | 18.0 | ||
| Widowed | 21 | 5 | 10.0 | 16 | 10.7 | ||
| Unknown | 2 | 1 | 2.0 | 1 | 0.67 | ||
| Did patient undergo surgery by author? | .81 | ||||||
| No | 105 | 27 | 54.0 | 78 | 52.0 | ||
| Yes | 95 | 23 | 46.0 | 72 | 48.0 | ||
Patients in the positive Dysmorphic Concern Questionnaire screen group were younger (median age of 51.8 years vs 61.0 years; P = .004) and had more eyelid surgeries (0.90 surgeries vs 0.52 surgeries; P = .007) than those in the control group. There was a trend toward lower weight and higher number of previous cosmetic surgeries in the positive Dysmorphic Concern Questionnaire screen group. Table 2 shows the relationship between group and continuous variables for the entire cohort.
| Factor | Case | Control | P Value | ||
|---|---|---|---|---|---|
| N | Statistics a | N | Statistics a | ||
| Age upon survey | 50 | 51.8 (19.8) | 150 | 61.0 (16.5) | .004 S |
| Height | 38 | 164.1 (12.0) | 132 | 167.8 (9.8) | .089 S |
| Weight | 43 | 72.2 (20.6) | 136 | 77.9 (17.3) | .11 S |
| Body mass index | 38 | 26.7 (6.3) | 132 | 27.4 (5.1) | .53 S |
| Number of children | 12 | 1.0 (0.0, 2.5) | 43 | 2.0 (0.0, 3.0) | .60 W |
| Number of cosmetic surgeries | 50 | 0.34 (0.82) | 150 | 0.15 (0.47) | .16 W |
| Number of eyelid surgeries | 48 | 0.90 (.97) | 150 | 0.52 (0.83) | .007 W |
| Number of other surgeries | 50 | 2.0 (1.0, 6.0) | 150 | 2.0 (1.0, 4.0) | .32 W |
| Number of Botox/filler/other procedures | 50 | 0.0 (0.0, 0.0) | 150 | 0.0 (0.0, 0.0) | .97 W |
| Number of previous doctors visited | 49 | 11.0 (4.0, 24.0) | 150 | 12.0 (6.0, 19.0) | .86 W |
Patients in the positive Dysmorphic Concern Questionnaire screen group who underwent surgery were significantly more likely to have complications (19.1% vs 0%; P = .002) compared to those in the control group who underwent surgery. Complications included lagophthalmos after levator advancement in a previously operated eyelid (2 cases), trichiasis after canthoplasty (1 case), and persistent scalp hypesthesia with persistent unexplained visual complaints after repeat blepharoptosis repair, blepharoplasty, and brow lift (1 case). Patients in the positive Dysmorphic Concern Questionnaire screen group who underwent surgery possessed higher postoperative pain scores as well ( P = .034). Patients in the positive Dysmorphic Concern Questionnaire screen group who underwent surgery underwent more reoperations (22.7% vs 6.9%; P = .050). Table 3 shows the relationship between group and categorical variables for patients undergoing surgery.
| Factor | Level | Total | Case | Control | P Value | ||
|---|---|---|---|---|---|---|---|
| N | (%) | N | (%) | ||||
| Reoperation | .050 F | ||||||
| No | 84 | 17 | 77.3 | 67 | 93.1 | ||
| Yes | 10 | 5 | 22.7 | 5 | 6.9 | ||
| Complications from author operations? | .002 F | ||||||
| No | 89 | 17 | 81.0 | 72 | 100.0 | ||
| Yes | 4 | 4 | 19.1 | 0 | 0.00 | ||
| Preoperative pain score | .35 W | ||||||
| 0 | 83 | 19 | 82.6 | 64 | 90.1 | ||
| 3 | 2 | 1 | 4.4 | 1 | 1.4 | ||
| 4 | 1 | 0 | 0.00 | 1 | 1.4 | ||
| 5 | 4 | 2 | 8.7 | 2 | 2.8 | ||
| 8 | 1 | 0 | 0.00 | 1 | 1.4 | ||
| 9 | 3 | 1 | 4.4 | 2 | 2.8 | ||
| Postoperative pain score | .034 W | ||||||
| 0 | 63 | 14 | 73.7 | 49 | 92.5 | ||
| 1 | 1 | 1 | 5.3 | 0 | 0.00 | ||
| 4 | 1 | 0 | 0.00 | 1 | 1.9 | ||
| 5 | 2 | 0 | 0.00 | 2 | 3.8 | ||
| 6 | 1 | 1 | 5.3 | 0 | 0.00 | ||
| 7 | 1 | 1 | 5.3 | 0 | 0.00 | ||
| 8 | 3 | 2 | 10.5 | 1 | 1.9 | ||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


