CHAPTER 51 Blepharoplasty

Anatomy
It is important to develop the ability to ‘see through’ the skin and subcutaneous tissues that drape over the deep anatomic substrates of the periorbital area. The surgeon should get a sense of the contribution of these various substrates to the existing surface anatomy, and therefore a sense of which substrates are available for surgical modification. An understanding of the three-dimensional contours in this area, the contribution of soft tissue and bone, and how they can be enhanced is key in blepharoplasty surgery. Figure 51.1 demonstrates the important characteristics of surface anatomy. Skin and subcutaneous tissues can be excised to reduce redundancy, and fat can be removed to expose the deeper structures, such as the levator aponeurosis and bony orbital rim.
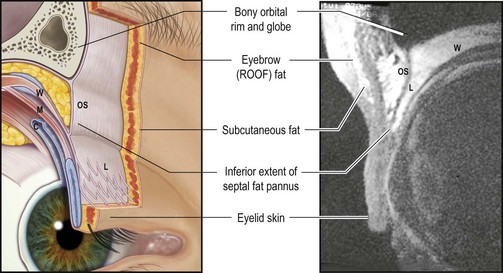
Fig. 51.1 Sagittal section of upper eyelid anatomy.
From Goldberg RA, Wu JC, Jesmanowicz A, et al. Eyelid anatomy revisited. Dynamic high-resolution magnetic resonance images of Whitnall’s ligament and upper eyelid structures with the use of a surface coil. Arch Ophthalmol 1992;110:1598–600, with permission.
The contour of the tightly attached skin over the levator aponeurosis and tarsus forms the eyelid ‘platform,’ which we call the ‘tarsal platform show’. The septal fat pannus overlies the levator and upper tarsal plate. Racial variations exist, and are important here. At one extreme lies the Asian patient, with an abundant septal fat pannus consisting of skin, subcutaneous eyelid and eyebrow fat that covers the entire tarsal plate, and essentially obliterates any visible platform. At the other extreme lies the aged Caucasian patient with superior sulcus fat atrophy, in which case the entire levator can often be followed up into the orbit, sometimes even with Whitnall’s ligament exposed as a horizontal band just below the orbital rim (Fig. 51.2A and B).


The most medial portion of the upper eyelid, combined with the lateral surface of the nose and the medial canthus, constitutes an area that deserves particular attention. Redundancy in this area is often related to eyebrow ptosis, with tissues encroaching from the glabella to form a diamond-shaped deformity. We can see these changes in a composite photograph of a woman at age 25 and age 75 (Fig. 51.3). This anatomically complex area has different tissue characteristics from the interdigitation of different skin textures. Incisions should not extend into this area because of the high potential of producing postoperative webs or other irregularities that give an esthetically unpleasant outcome (Fig. 51.4). Elevation of the redundant eyebrow tissues out of the multicontoured space, for example through endoscopic forehead lift, is often more effective in restoring the normal width of the radix and improving the contours in the multicontoured medial eyelid space.


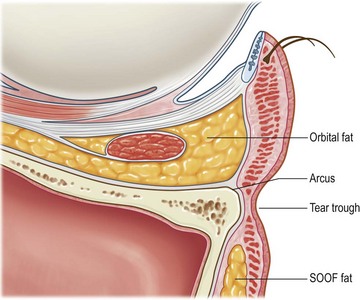
The lower eyelid is composed of skin and underlying orbicularis muscle, which continues past the lower orbital rim onto the face. Behind the orbicularis, near the lid margin, is the tarsal plate. The orbital septum fuses with the inferior border of the tarsus and continues caudally to attach to the crest of the lower orbital rim at the arcus marginalis. Just behind the orbital septum are the lower eyelid orbital fat compartments. The orbital fat is bordered posteriorly and superiorly by the lower eyelid retractors, which arise from the inferior rectus muscle and tendon. The lower lid retractors fuse with the orbital septum approximately 5 mm inferior to the inferior tarsal border before inserting onto the tarsal plate. Posteriorly, the lower eyelid retractors are closely adherent to the palpebral conjunctiva of the lower lid (Fig. 51.5).The orbital fat is surrounded by many fine connective tissue septae (septae of Koorneef). A fascial extension of the sheath of the inferior oblique muscle and Lockwood’s ligament called the arcuate expansion inserts on the inferolateral orbital rim and separates the central from the lateral fat compartments. The inferior oblique muscle originates from the anterior medial orbital floor and separates the medial fat compartment from the central fat compartment as it passes posteriorly and laterally beneath the equator of the globe. The lateral fat compartment lies more posteriorly, the central fat compartment lies more anteriorly, and the medial fat compartment is paler in color. As shown in Figure 51.5, the orbital fat can be easily accessed by incising the conjunctiva and lower lid retractors in the fornix while the orbital septum remains well anterior to these structures.
Eyelid assessment: fundamental principles and surgical planning
Upper blepharoplasty
Upper eyelid fullness is generally a congenital condition (Fig. 51.6A). It can be addressed by removal of fat from the upper eyelid, exposing the underlying levator aponeurosis and tarsus (Fig. 51.6B, presurgery and C, postsurgery). The surgeon must recognize when the fullness in the eyelid complex is caused by eyebrow descent. The eyebrows are held at a certain position by the tone of the frontalis muscle, which maintains comfortable vision. If heavy tissues are removed from below the brow, it will descend to its resting position (Figs 51.7 and 51.8).





If too much of the septal fat pannus and ROOF (retro-orbicularis oculi fat or eyebrow fat pad) is removed, the underlying structures will be exposed to an undesirable degree (Fig. 51.9A and B). As already mentioned, excessive hollowness of the superior sulcus gives an aged appearance to the eyelid complex. Blepharoplasty in the thin aged upper eyelid must be conservative, with minimal removal of fat. Because there will not be much of a septal fat pannus or eyelid fold to cover the incision, the crease is often made high in the eyelid where it will fall into the shadow of the superior sulcus and be relatively hidden.


If the globe is relatively prominent, the tarsal platform show will be more readily exposed by removing orbital fat (Fig. 51.10). The orbital fat and full eyelid tissues actually benefit the patient by masking underlying proptosis. In this situation the admonition ‘big eye, big trouble’ should be heeded, and fat removal should be conservative or even avoided altogether, perhaps in favor of orbital decompression for proptosis reduction.

Racial variations are also significant in planning and executing upper blepharoplasty. For example, compared with the Occidental configuration, the Oriental eyelid is characterized by a full, sometimes bulging superior sulcus and a low crease with narrow or absent tarsal platform. The crease narrows medially to form an epicanthal fold. The fullness is based anatomically on abundant and somewhat fibrotic fat in the subcutaneous, suborbicularis, and postaponeurotic spaces. This abundant fat can be carefully sculpted because it is fibrotic, but it is unforgiving, so it is easy to create a contour abnormality, a visible dent, or an undesired second crease if the fat is not evenly, or conservatively, sculpted. The goal of Asian blepharoplasty is usually to retain the full characteristic of the eyelid while better defining the thin tarsal platform show. To accomplish this, conservative debulking of the inferior edge of the septal fat pannus (with sparing and avoidance of the remainder) is performed. Fixation of the orbicularis or skin edge to the exposed tarsus can also be performed to create a firm, low, and meticulously symmetric crease (Fig. 51.11A and B).


Lower blepharoplasty
Lower blepharoplasty addresses the contours of the lower eyelid and cheek. When evaluating patients for possible lower eyelid surgery, the contours of the orbital fat should be observed. Often the medial, central, and lateral fat pads can be identified and individually graded (Fig. 51.12
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


