Purpose
To describe a surgical method of bleb revision for hypotony maculopathy, to evaluate its long-term efficacy, and to define the relationship between the duration of hypotony maculopathy and visual acuity (VA) outcomes.
Design
Noncomparative retrospective case series.
Methods
Medical records of 33 patients with hypotony maculopathy who underwent primary bleb revision between June 1999 and September 2012 by a single surgeon at an academic medical center were reviewed. Hypotony maculopathy was characterized by the presence of a decrease in VA, retinal striae, and macular edema in the setting of decreased intraocular pressure (IOP) after glaucoma filtering surgery. The main outcome measure was final logMAR VA after bleb revision at 6 and 12 months.
Results
Thirty-three eyes of 33 patients were followed for 4.68 ± 3.56 years (range 0.55–12.69 years). Mean duration of hypotony maculopathy was 4.98 ± 8.93 months. LogMAR VA improved from 0.78 ± 0.40 at baseline to 0.34 ± 0.34 ( P < .001) 6 months after bleb revision and to 0.45 ± 0.55 ( P < .001) 12 months after bleb revision. Spearman rank coefficient (r s ) correlating duration of hypotony and BCVA at both 6 and 12 months was significant ( P = .015 and r s = 0.426, P = .028 and r s = 0.416, respectively). Mean IOP increased from 3.51 ± 2.27 mm Hg to 12.06 ± 4.06 mm Hg ( P < .001) at 12 months. Fifty-two percent were on no antiglaucoma medications at last follow-up. Five eyes (15%) required a second bleb revision to correct persistent hypotony maculopathy.
Conclusion
Surgical repair for hypotony maculopathy provided a significant improvement in VA at 6 and 12 months. Surgical bleb revision is associated with good long-term control of IOP and improved VA in eyes with hypotony maculopathy after previous glaucoma filtering surgery.
Hypotony maculopathy is a complication of glaucoma filtration surgery that occurs in 1.3%–20% of eyes having undergone trabeculectomy with mitomycin C (MMC). The clinical findings were first described by Dellaporta in 1954 as “creasing of retina in hypotonia,” but the actual term for hypotony maculopathy was not coined until 1972 by Gass to emphasize the etiology of vision loss in the setting of chorioretinal folds. The condition is characterized by a decrease in visual acuity caused by macular folds, retinal edema, papilledema, and vascular tortuosity. Structurally, it has been postulated that low intraocular pressure (IOP) causes thickening of the perifoveal choroid and sclera, which causes the perifoveal and foveal retina to become displaced centrally, giving the appearance of radial folds clinically. Over time, these changes can cause photoreceptor damage, which can limit recovery of visual function even after normal IOP has been restored.
Statistically, hypotony can be defined as an intraocular pressure of less than 6.5 mm Hg, which is greater than 3 standard deviations below the mean IOP. Clinically, hypotony has been described as a low pressure in an individual eye leading to pathologic functional and structural changes. In the setting of glaucoma surgery, hypotony is oftentimes the result of overfiltration or excessive aqueous outflow. It is well established that the use of antifibrotic agents (particularly MMC) at the time of glaucoma surgery increases the probability of a successful outcome. However, the use of such agents as an adjunct to trabeculectomy has also been associated with an increased incidence of ocular hypotony. In addition, some studies have shown that the frequency of hypotony maculopathy occurs more commonly as the dose or duration of adjunctive intraoperative MMC is increased. Other risk factors that have been associated with the development of hypotony maculopathy include male sex, younger age, myopia, and preoperative use of carbonic anhydrase inhibitors.
When left untreated, hypotony maculopathy can have long-term visual consequences. Proposed treatments for postsurgical hypotony maculopathy are centered on methods to decrease aqueous outflow and to raise IOP to functional levels. Some of the more conservative measures of treatment include pressure patching and the application of trichloracetic acid or cryotherapy directly to the bleb. Placement of an oversized bandage contact lens has also been shown in 1 study to be helpful for early postoperative hypotony. Injection of autologous blood into or around the bleb is reported to produce more variable results; however, complications have been reported with this procedure. A variety of surgical approaches have been proposed, including resuturing of the scleral flap, patch grafting with donor pericardium or sclera, placement of compression sutures, and transconjunctival suturing of the scleral flap.
We propose that surgical bleb revision is a safe and effective primary method of treating hypotony maculopathy in the setting of overfiltration from trabeculectomy. The purpose of this study is to evaluate the results of surgical bleb revision in those patients with post-trabeculectomy hypotony maculopathy by evaluating changes in visual acuity (VA) and IOP, and to correlate these results with the duration of hypotony maculopathy.
Methods
Approval from the Institutional Review Board of the University of California, Los Angeles was obtained to conduct this noncomparative, retrospective case series. The medical records of all patients who underwent bleb revision surgery by a single surgeon (J.C.) at the Jules Stein Eye Institute between October 11, 1999 and July 16, 2012 were identified and reviewed. Patients who had previously undergone primary trabeculectomy with adjunctive MMC and subsequently developed hypotony maculopathy in the postoperative period were included. Other inclusion criteria included age 18 years or greater and a minimum follow-up of at least 6 months following bleb revision surgery. The diagnosis of hypotony maculopathy was defined clinically according to the presence of macular folds on funduscopy in the setting of an IOP <6 mm Hg or an IOP greater than this in the presence of typical clinical features of hypotony maculopathy and a decrease of 1 or more lines in the best-corrected Snellen visual acuity. Eyes with a history of any other incisional surgery besides trabeculectomy or cataract surgery, prior to the onset of hypotony maculopathy, were excluded.
Surgical Procedure
Anesthesia for all patients at the time of surgery consisted of a peribulbar block of 2% lidocaine. A 3 mL injection was delivered to the inferotemporal orbit with a 23 gauge Atkinson needle. All blocks were performed under monitored anesthesia care in the presence of an anesthesiologist. Topical tetracaine 0.5% eye drops were used to supplement the block as needed during the surgery.
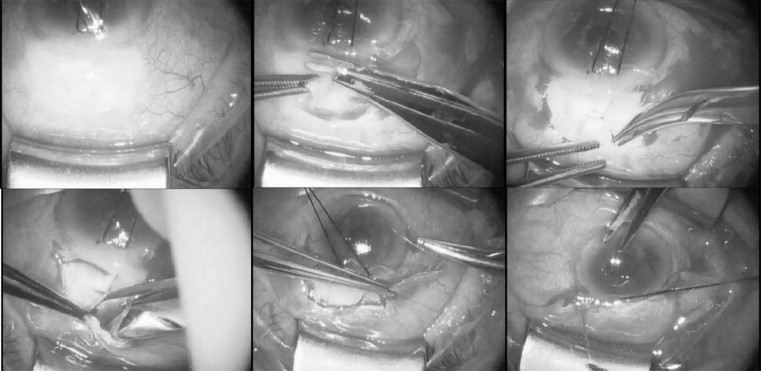
Bleb revision involved sharp dissection and excision of thin or leaky conjunctiva and adjacent Tenon capsule along the outer aspect of the bleb with Westcott scissors. The scleral flap was resutured with 1 or more interrupted 10-0 nylon sutures, when the strength of the tissue permitted. In some cases, a pericardial patch graft or a horizontal mattress compression suture was used to provide additional resistance to aqueous outflow if resuturing of the scleral flap alone was found to be insufficient for this purpose. Finally, the conjunctiva was mobilized by freeing its attachments to the sclera and superior rectus muscle, advanced, and reattached to the limbus with a 9-0 monofilament polyglactin suture on a tapered noncutting needle. These steps are illustrated in Figure 1 .
When deemed necessary by the surgeon, drainage of suprachoroidal fluid was performed in the presence of an anterior chamber maintainer by creating a conjunctival peritomy in the area of the choroidal effusion. A scleral cutdown was then performed approximately 3 mm posterior to the limbus. After initial drainage of suprachoroidal fluid, a Barraquer sweep was inserted into the suprachoroidal space parallel to the limbus to access and remove any other existing pockets of fluid. The scleral wound was then closed with a 9-0 polyglactin suture.
Main Outcomes
Demographic data, including age, race, sex, ocular history, and glaucoma subtype, were collected for all patients. All visual acuity was converted to logMAR visual acuity from the recorded best-corrected Snellen visual acuity (BCVA). The BCVA at the time of hypotony maculopathy diagnosis was compared with the BCVA after bleb revision at 6 and 12 months. IOP measurements were also collected at the same time points. Duration of hypotony from the time of diagnosis until bleb revision was recorded, in addition to any complications after bleb revision surgery, including the need for additional surgery. Other variables that were analyzed include surgical technique at the time of bleb revision and the number of glaucoma medications needed for adequate IOP control at final follow-up. The relationship between logMAR BCVA at 12 months as a function of both duration of hypotony maculopathy and preoperative IOP was also plotted. Successful resolution of hypotony maculopathy was not defined by IOP criteria alone but was also defined by improvement of BCVA and macular abnormalities. Failure was defined as IOP <5 mm Hg, decreased visual acuity, persistent macular striae or macular edema, need for a second bleb revision surgery, or need for additional glaucoma surgery for IOP reduction.
Statistical Analysis
Statistical analysis was performed with a paired-samples t test to compare logMAR BCVA and IOP preoperatively and postoperatively. Long-term outcomes were plotted on a Kaplan-Meier survival curve according to predefined criteria for failure. Specifically, postoperative failure was defined as an IOP of less than 5 mm Hg, a decrease in BCVA from baseline, persistence of macular striae or edema after revision, the need for a second bleb revision, or the need for additional glaucoma surgery to achieve adequate IOP control. The Spearman rank correlation coefficient (r s ) was used to determine the correlation between duration of hypotony maculopathy and logMAR BCVA at 6 and 12 months. All data are presented as the mean ± standard deviation unless otherwise indicated. A P value of <.05 was considered statistically significant for the purpose of our analysis.
Results
Demographics and Clinical Characteristics
A total of 126 charts of patients who underwent bleb revision were reviewed. Thirty-three eyes of 33 patients met criteria for trabeculectomy-induced hypotony maculopathy and were included in this study. Bleb revision in the remaining 93 patients was performed for other reasons, such as the presence of a bleb leak in the absence of hypotony maculopathy, glaucoma progression requiring revision of an existing bleb to achieve a further reduction in IOP, bleb dysesthesia, or bleb failure leading to inadequate IOP control. Demographic and clinical characteristics of the study patients are summarized in the Table . The average age of the study population was 63.12 ± 13.3 years (range 43–93 years). Sixteen patients were male and 17 were female. Demographic and clinical characteristics, including race and glaucoma diagnosis, are summarized in the Table .
| Age (y) | 63.12 ± 13.3 (range: 43–93) |
| Male:female ratio | 16:17 |
| Race | 27 (82%) white |
| 2 (6%) African American | |
| 1 (3%) Hispanic | |
| 3 (9%) Asian | |
| Laterality | 20 (60.6%) left eyes |
| Type of glaucoma | 17 (52%) primary open-angle glaucoma |
| 2 (6%) pigmentary dispersion glaucoma | |
| 2 (6%) pseudoexfoliative glaucoma | |
| 5 (15%) normal tension glaucoma | |
| 2 (6%) chronic angle closure glaucoma | |
| 1 (3%) steroid-induced glaucoma | |
| 2 (6%) uveitic glaucoma | |
| 1 (3%) angle recession glaucoma | |
| Lens status | 15 (45.5%) phakic |
| 18 (55.5%) pseudophakic | |
| Macula striae | 33 (100%) |
| Choroidal effusion | 5 (15%) |
| Macular edema | 8 (24%) |
| Duration of hypotony | 4.98 ± 8.93 months (3 days–4 years) |
All study patients had previously undergone an initial trabeculectomy with MMC. Concentration of MMC used was available for 16 patients and ranged from 0.2 mg/mL to 0.3 mg/mL for 1 minute in those patients. Of these, 14 patients received MMC at a concentration of 0.3 mg/mL at the time of trabeculectomy, 1 received 0.25 mg/mL, and 1 received 0.2 mg/mL. These data were not available for the remaining 17 patients who had their initial trabeculectomy done elsewhere.
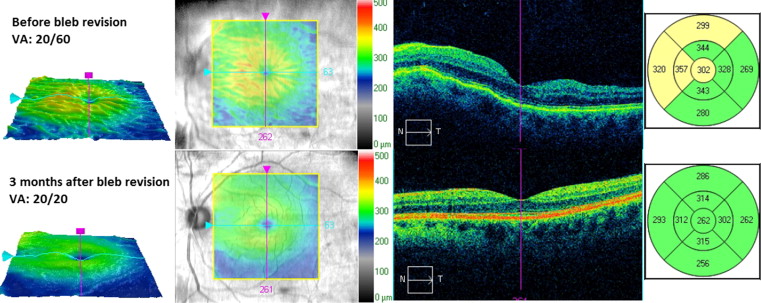
The mean time between the diagnosis of hypotony maculopathy and surgical revision was 4.98 ± 8.93 months (range 3 days–4 years). Prior to bleb revision surgery, all patients (100%) had macular striae and 5 (15%) had accompanying choroidal effusions visible on indirect ophthalmoscopy. Eight patients (24%) had macular edema at the time of diagnosis. A typical example of optical coherence tomography (OCT) findings is shown in Figure 2 for a study patient before and after bleb revision.
Surgical Technique
All 33 patients underwent bleb revision surgery for hypotony maculopathy as described above in the Methods section. All patients underwent resuturing of the scleral flap with accompanying conjunctival advancement following resection of any friable or leaking conjunctival tissue. Nine patients (27%) required a pericardial patch graft to provide additional resistance to aqueous flow. Concomitant choroidal drainage was performed in 1 patient (3%). A compression suture was placed in 11 patients (33%) to further secure the scleral flap.
Outcomes
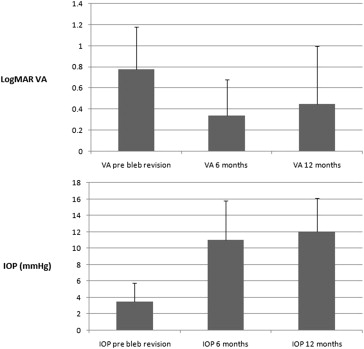
Patients were followed for a total of 4.68 ± 3.56 years (range 0.55–12.69 years) from the time of bleb revision surgery to final follow-up. Twenty-nine patients (88%) experienced improvement of BCVA following bleb revision, and of these, 28 patients (85%) experienced an improvement of −0.2 or more in logMAR BCVA. Mean logMAR BCVA prior to bleb revision was 0.78 ± 0.40 (range 0.2–2.0). Mean logMAR BCVA was 0.34 ± 0.34 (range 0–2.0) at 6 months after bleb revision and 0.45 ± 0.55 (range 0–2.0) 12 months after bleb revision. The change in mean BCVA at both 6 months and 12 months was found to be statistically significant, with P < .001 at both 6 months and 12 months when compared to the preoperative BCVA.
The mean preoperative IOP before bleb revision was 3.51 ± 2.27 mm Hg (range 0.5–10 mm Hg). Mean IOP at 6 and 12 months post bleb revision were 11.03 ± 4.73 mm Hg (range 3–20 mm Hg) and 12.06 ± 4.06 mm Hg (range 3–21 mm Hg), respectively. Mean IOP at 6 and 12 months was significantly higher than preoperative IOP, with P < .001 at both time points. Thirty-one out of 33 patients (94%) had a sustained increase in IOP at 12 months. Figure 3 demonstrates these BCVA and IOP results graphically.
Seventeen of the 33 study patients (52%) did not require topical glaucoma medications at final follow-up. Nine patients (27%) required 2 or more topical glaucoma medications to achieve adequate IOP control at their last follow-up visit.
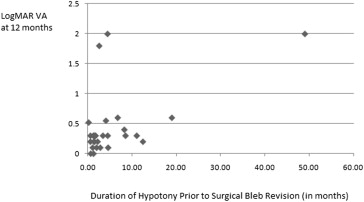
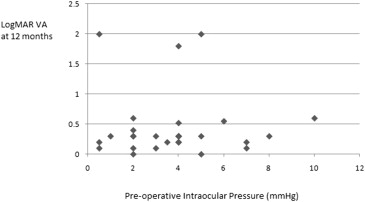
LogMAR VA at 12 months was also plotted as a function of hypotony duration as well as preoperative IOP. These results are shown graphically in Figures 4 and 5 . Duration of hypotony maculopathy vs change in logMAR VA was also plotted ( Figure 6 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


