Purpose
To biometrically and molecularly characterize clinically diagnosed posterior microphthalmos.
Design
Prospective case series.
Methods
Twenty-five affected patients from 13 families diagnosed by ophthalmologists experienced with the condition at the King Khaled Eye Specialist Hospital were studied. All participants underwent axial length measurement, keratometry, corneal pachymetry, and candidate gene analysis ( MFRP , PRSS56 ). Main outcome measures were the results of ocular biometry and gene analysis.
Results
All patients (2-47 years of age) had high hyperopia, normal-appearing anterior segments, posterior chamber foreshortening, and characteristic papillomacular folds/wrinkles. For the right eye, mean cycloplegic refraction was +15.09 diopters (D) (range 9.88-18.75). Axial length (mean 16.25 mm [range 14.88-19.88]) had strong inverse correlation (Pearson coefficient −0.88, P < .0001) with corneal power (mean 48.89 D [range 41.91-52.25]) and a positive correlation with corneal diameter (Pearson 0.64, P = .001). Corneal thickness and anterior chamber dimensions were within normal ranges. Left eye data were similar. Nineteen Saudi patients (8/13 families) harbored 4 different homozygous PRSS56 mutations, 1 Indian and 1 Saudi patient harbored 2 different homozygous MFRP mutations, and 4 Saudi patients (3/13 families) had no detectable mutation in either gene. Patients with MFRP mutations were not clinically different from patients with PRSS56 mutations or no identified mutation. Truncating PRSS56 mutations were associated with shorter axial lengths (mean 15.72 mm) than missense PRSS56 mutations (mean 16.37 mm) or no identified mutation (mean 17.57 mm).
Conclusions
These data define posterior microphthalmos biometrically and reveal that corneal steepening proportional to the degree of axial foreshortening is part of the phenotype. Corneal diameter decreases with decreasing axial length, suggesting posterior microphthalmos and nanophthalmos represent a spectrum of high hyperopia rather than distinct phenotypes. In the Saudi population PRSS56 mutations are the major cause, and in our cohort truncating mutations were associated with a more severe phenotype.
Posterior microphthalmos is defined clinically as an otherwise-normal eye with the following: high hyperopia, normal-appearing anterior segment of normal or subnormal dimensions, short axial length, characteristic papillomacular folds and/or wrinkles, chorioretinal folds, pseudopapilledema, sclerochoroidal thickening, and/or uveal effusions. These features are also present in nanophthalmos, but in the latter the anterior segment, although appearing structurally normal, is noticeably small. To date, approximately 100 posterior microphthalmos cases are described in the literature, and most of these studies have emphasized the axial length and posterior segment findings. Axial lengths have varied from 12.30 to 20.36 mm (mean 15.97 mm) and hyperopia from +7.5 to 21.5 diopters (D) (mean +14.92 D). Steeper-than-normal corneas were reported in some cases; however, for most cases the anterior segments were described as normal. To date, detailed biometric analysis of the cornea and its relationship (or lack of relationship) to axial length has not been formally studied in a cohort of posterior microphthalmos patients.
Recently, recessive mutations in the membrane-type frizzled-related protein ( MFRP ) and the serine protease PRSS56 have been shown to cause posterior microphthalmos, although not all analyzed cases have identifiable mutations in 1 of these 2 genes. The fact that recessive mutations in MFRP and PRSS56 can also cause nanophthalmos suggests that posterior microphthalmos and nanophthalmos represent a spectrum of hyperopia rather than 2 distinct conditions, but data are lacking on the biometric determinants of the final phenotype and on possible genotype/phenotype correlation. In this study, we attempt to address the existing gap in our knowledge of what defines posterior microphthalmos by performing a detailed biometric analysis in a large cohort of clinically diagnosed posterior microphthalmos patients and studying how this analysis correlates with the mutations in the 2 genes that are known to cause this condition.
Subjects and Methods
Human Subjects
Prospective approval from the Institutional Review Boards of the King Khaled Eye Specialist Hospital and King Faisal Specialist Hospital and Research Centre was obtained for this prospective study, which adhered to the tenets of the Declaration of Helsinki. Patients and families referred to and clinically diagnosed by 2 of the authors (S.R.N., A.O.K.) were invited to participate, and all patients and their families gave informed consent to participate in this research study. All patients had hyperopia of ≥8 D, axial length <20 mm, characteristic full-thickness retinal papillomacular folds (in 23 patients) or wrinkles (in 2 patients), a normal-appearing anterior segment with grossly normal dimensions, normal intraocular pressure, and no developmental ocular malformations or syndromic disease. The cut-off values for hyperopia (≥8 diopters) and axial length (<20 mm) were arbitrarily chosen to be consistent with reported accepted values for posterior microphthalmos.
All diagnosed patients underwent complete ophthalmic examination including best-corrected Snellen visual acuity (or fixation patterns for preverbal children), intraocular pressure measurement by applanation tonometry (or Tonopen [Reichert Technologies, Depew, New York, USA] for young children), measurement of the horizontal and vertical corneal diameters with a caliper, slit-lamp examination of the anterior segment and of the posterior pole with a noncontact lens, indirect ophthalmoscopy, and cycloplegic refraction (following cyclogel 1%) by retinoscopy or autorefraction (Nidek ARK-700 Autorefractor-keratometer [Nidek, Gamagori, Japan]; Topcon KR 8800 Autokerato-refractometer [Topcon, Tokyo, Japan]). Only the horizontal corneal diameter was considered in the corneal diameter analysis. In addition, all diagnosed patients had the following ancillary testing: (1) standardized optical biometry (IOLMaster; Carl Zeiss Meditec AG, Jena, Germany) for axial length of the globe, central anterior chamber depth, lens thickness, vitreous compartment length, and ultrasound measurement of sclerochoroidal thickness; (2) manual keratometry (Nidek ARK-700 Autorefractor-keratometer, or Topcon KR 8800 Autokerato-refractometer) with averaging of the steep and flat corneal meridians for analysis; (3) simulated keratometry by the Orbscan IIz (Bausch and Lomb, Salt Lake City, Utah, USA); (4) central corneal thickness (CCT) measurement by ultrasound pachymetry (Pachymeter SP-3000; Tomey Corporation, Nagoya, Japan); and (5) CCT by Orbscan IIz. For final corneal power of each eye, the average corneal powers from the 2 methods (manual keratometry and Orbscan IIz) were averaged. For the final corneal thickness of each eye, corneal thickness values from the 2 methods (ultrasound and Orbscan IIz) were averaged.
Biometry statistics were performed for right eyes and left eyes separately using SPSS 14.0 (SPSS Inc, Chicago, Illinois, USA), with particular attention to the relation between axial length and corneal variables (ie, power, diameter, and thickness) (Pearson correlation coefficient).
Molecular Studies
We have previously described our attempt to map the disease gene in a number of families with autosomal recessive posterior microphthalmos before PRSS56 was identified by another group. In that study, we found that most patients mapped to the PRSS56 locus, 1 family had a pathogenic mutation in MFRP (Family 1), and another showed no linkage to the PRSS56 locus (Family 11). In this study, we screened the coding regions of PRSS56 ( NM_001195129.1 ) using PCR-based amplification followed by direct sequencing for those families that linked to PRSS56 . In addition, using similar techniques we assessed 5 newly identified families for mutations in PRSS56 and MFRP .
Genomic DNA was extracted from whole blood anti-coagulated with EDTA using the Puregene Gentra DNA Extraction Kit (Cat. # D-5000; Gentra Systems, Minneapolis, Minnesota, USA) according to the manufacturer’s instructions. The DNA was quantified spectrophotometrically and stored in aliquots at −20 C until required. Sequencing of MFRP and PRSS56 was as described before. Sequence analysis was performed using the SeqManII module of the Lasergene (DNASTAR Inc, Madison, Wisconsin, USA) software package using normal sequence for comparison.
Results
Clinical Features
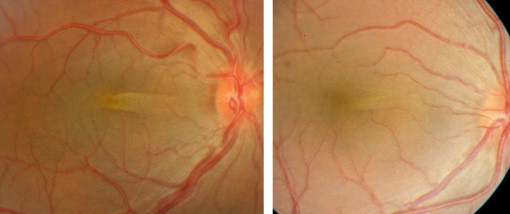
Twenty-five affected patients (2-47 years of age, 14 male and 11 female) from 13 families were enrolled. Linkage analysis for 7 of these families was previously reported. All families were Saudi Arabian except 1, which was South African of Indian descent (Family 1). Seven of the 12 Saudi Arabian families were consanguineous. With the exception of Family 4, all affected subjects had unaffected parents, whose eyes had no or very minor refractive errors. All patients had hyperopia of ≥8 D, axial length <20 mm, characteristic full-thickness retinal papillomacular folds (in 23 patients) or wrinkles (in 2 patients), a grossly normal anterior segment, and no developmental ocular malformations or syndromic disease ( Figure 1 ). No patient had night blindness or clinical signs of retinal degeneration.
Best-corrected Snellen visual acuity ranged from 20/30 to 20/160. Intraocular pressure was normal in all eyes. The spherical equivalent of refractive errors ranged from +9.88 to +18.75 D (average +15.09) in the right eye (OD) and from +9.13 to +18.88 D (average +15.09) in the left eye (OS).
Biometrically, the 2 eyes of a given individual were similar. Patient data for the right eye are detailed in Table 1 and summarized below. Data for the left eye were similar and are available in Supplemental Table 1 (available at AJO.com ).
| Family-Pt. # | Age (y)/Sex (M/F) | Hyperopia Spherical Equivalent (D) | Horiz Corneal Diameter (mm) | Keratometry | Pachymetry | A-Scan | Papillomacular Fold | Genetic Mutation | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Manual K Average (D) | Orbscan K Average (D) | Overall K Average (D) | Corneal Thickness Average (μm) | Central AC Depth (mm) | Lens Thickness (mm) | Axial Vitreous Length (mm) | Globe AL (mm) | ||||||
| F1-P1 | 11/M | 12.38 | 11.50 | 50.00 | 49.50 | 49.75 | 547 | 2.99 | 4.27 | 9.30 | 16.56 | Moderate | MFRP |
| F2-P2 | 5/M | 17.63 | 10.00 | 50.63 | 51.70 | 51.16 | 537 | 2.64 | 4.39 | 7.81 | 15.21 | Thick | PRSS56 |
| F3-P3 | 21/F | 13.00 | 11.50 | 48.38 | 49.77 | 49.07 | 556 | 3.11 | 4.20 | 9.04 | 16.35 | Moderate | PRSS56 |
| F3-P4 | 23/F | 12.88 | 12.25 | 47.48 | 47.40 | 47.44 | 502 | 2.87 | 4.67 | 9.36 | 16.90 | Moderate | PRSS56 |
| F3-P5 | 21/F | 15.13 | 12.00 | 49.06 | 49.80 | 49.43 | 528 | 3.06 | 4.60 | 7.92 | 15.58 | Moderate | PRSS56 |
| F3-P6 | 20/M | 14.00 | 12.25 | 47.60 | 48.40 | 48.00 | 611 | 3.31 | 4.47 | 9.29 | 17.07 | Moderate | PRSS56 |
| F3-P7 | 13/F | 13.88 | 12.00 | 47.82 | 47.63 | 47.73 | 571 | 3.56 | 4.07 | 9.04 | 16.67 | Moderate | PRSS56 |
| F4-P8 | 14/M | 15.00 | 12.00 | 49.82 | na | 49.82 | na | 3.30 | na | na | 16.50 | Thick | PRSS56 |
| F5-P9 | 21/F | 17.00 | 11.00 | 50.38 | 50.50 | 50.44 | 593 | 2.93 | 4.34 | 8.05 | 15.32 | Moderate | PRSS56 |
| F5-P10 | 12/M | 16.50 | 12.00 | 49.00 | 47.75 | 48.37 | 573 | 3.44 | 3.99 | 8.47 | 15.90 | Thick | PRSS56 |
| F5-P11 | 8/F | 14.13 | 11.00 | 49.64 | 49.20 | 49.42 | 563 | 3.24 | 4.00 | 8.55 | 15.79 | Moderate | PRSS56 |
| F6-P12 | 25/M | 14.50 | 11.50 | 47.62 | 48.00 | 47.81 | 620 | 3.35 | 4.20 | 9.00 | 16.55 | Thick | PRSS56 |
| F7-P13 | 47/M | 9.88 | 12.00 | 44.25 | 44.30 | 44.28 | 514 | 2.99 | 4.54 | 12.35 | 19.88 | Wrinkles | Not detectable |
| F8-P14 | 23/M | 17.75 | 10.75 | 48.02 | 47.85 | 47.94 | 562 | 3.18 | 4.14 | 8.73 | 16.05 | Thick | PRSS56 |
| F8-P15 | 18/F | 16.75 | 10.50 | 50.20 | 50.35 | 50.27 | 597 | 3.37 | 4.07 | 8.42 | 15.86 | Thick | PRSS56 |
| F8-P16 | 16/F | 18.75 | 10.50 | 48.29 | 51.00 | 49.64 | 556 | 3.31 | 3.87 | 8.48 | 15.66 | Moderate | PRSS56 |
| F8-P17 | 3.5/M | 16.13 | 11.50 | 48.78 | 50.50 | 49.64 | 624 | na | na | na | 15.24 | Thick | PRSS56 |
| F9-P18 | 33/F | 10.75 | 13.25 | 42.13 | 41.70 | 41.91 | 531 | 3.12 | 4.34 | 11.91 | 19.37 | Wrinkles | Not detectable |
| F10-P19 | 10/F | 17.00 | 11.50 | 48.67 | na | 48.67 | na | 3.09 | na | na | 15.69 | Thick | PRSS56 |
| F10-P20 | 2/M | 14.00 | 11.60 | 50.57 | na | 50.57 | na | 2.79 | na | na | 15.65 | Thick | PRSS56 |
| F11-P21 | 9/M | 13.50 | 10.60 | 52.34 | 50.65 | 51.50 | 572 | 3.16 | 3.94 | 9.06 | 16.16 | Moderate | Not detectable |
| F11-P22 | 5/M | 17.50 | 11.25 | 52.25 | na | 52.25 | 469 | 3.18 | na | na | 14.88 | Thick | Not detectable |
| F12-P23 | 26/M | 16.50 | 11.00 | 48.11 | 47.65 | 47.88 | 571 | 3.05 | 4.72 | 8.58 | 16.16 | Moderate | PRSS56 |
| F12-P24 | 20/F | 16.50 | 11.00 | 49.85 | 49.35 | 49.60 | 580 | 2.94 | 4.56 | 8.18 | 15.68 | Moderate | PRSS56 |
| F13-P25 | 10/M | 16.25 | 11.10 | 49.49 | 49.90 | 49.69 | 613 | 3.19 | 4.15 | 8.30 | 15.64 | Thick | MFRP |
| Mean | 16.66 | 15.09 | 11.42 | 48.81 | 48.71 | 48.89 | 563 | 3.13 | 4.28 | 8.99 | 16.25 | ||
| Median | 16.00 | 15.13 | 11.50 | 49.00 | 49.35 | 49.43 | 567 | 3.14 | 4.24 | 8.66 | 15.90 | ||
Horizontal corneal diameter ranged from 10.00 to 13.25 mm OD (mean 11.42 mm) (normal values for corneal diameters are 11.71 ± 0.42 mm ). Vertical corneal diameter was generally 0.25 to 0.5 mm shorter than the horizontal counterpart. For a given individual, corneal diameters were fairly symmetrical. For a given family, affected members had similar corneal diameters, although some intra-familial variation existed.
Axial length data were similar between the 2 eyes of a given individual ( Table 1 , Supplemental Table 1 ). The globe axial length ranged from 14.88 to 19.88 mm OD (mean 16.25 mm). Limited attention precluded measurement of the anterior chamber depth and/or lens thickness in some of the younger patients (Patients 2, 8, 17, 19, 20, 22). Central anterior chamber depth was normal or slightly subnormal, ranging from 2.79 to 3.56 mm OD (mean 3.13 mm, 24 eyes) (normal anterior chamber depth values are 3.14-3.6 mm ). Axial lens thickness was 3.87 to 4.72 mm OD (mean 4.28 mm, 20 eyes), which fell within normal dimensions when correlated for age. The short vitreous chamber ranged from 7.81 to 12.35 mm OD (mean 8.99 mm, 20 eyes). The sclerochoroidal thickness ranged from 1.35 to 2.20 mm OD (mean 1.75 mm, 19 eyes).
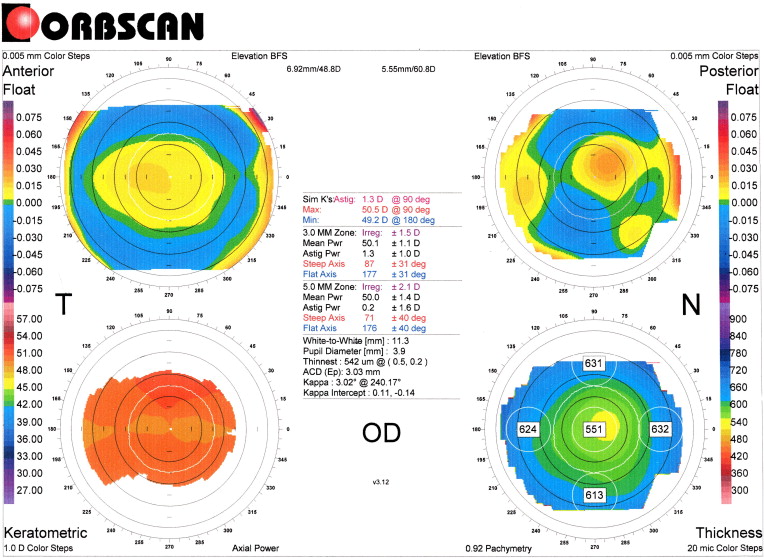
Reliable manual keratometry results were available bilaterally in all patients ( Table 1 , Supplemental Table 1 ). Most eyes had steep corneas (>43 D, average normal corneal power being 41.5 D for subjects 5-10 years, 42.5 D for those 11-30 years, and 43 to 44 D for those 31-50 years ). Manual keratometry reading ranges were 42.13 to 52.34 D OD (mean 48.81 D). Orbscan keratometry results were available bilaterally in 21 patients and similarly showed increased corneal curvature in almost all eyes ( Figure 2 ). Corneal power by Orbscan ranged from 41.70 to 51.70 D OD (mean 48.71 D). When the results of the manual and Orbscan keratometry were added and averaged for each eye, the corneal power in this series ranged from 41.91 to 52.25 D OD (mean 48.89 D).
Central corneal thickness measurements were available bilaterally in 22 patients ( Table 1 , Supplemental Table 1 ). Central corneal thickness values, measured by averaging 3 ultrasound pachymetric readings, ranged from 505 to 617 μm OD (mean 565 μm). Central corneal thickness as measured by the Orbscan was very similar, ranging from 498 to 624 μm OD (mean 564 μm). For the statistical analysis, a single “combined” corneal thickness obtained by averaging the ultrasound pachymetric and the Orbscan values was used. This value ranged from 469 to 624 μm OD (mean 563 μm), which is within the normal range for nonmyopic eyes.
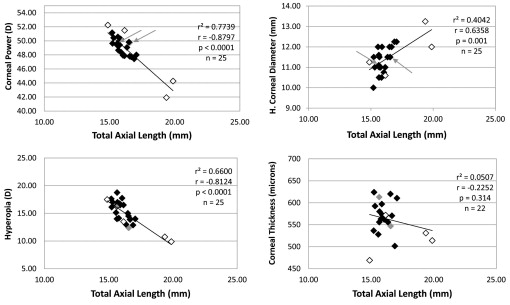
Statistical analysis for the right eye revealed total axial length to have a strong negative correlation with average corneal power (Pearson coefficient −0.88, P < .0001), a positive correlation with horizontal corneal diameter (Pearson 0.64, P = .001), and lack of significant correlations with corneal thickness (Pearson −0.23, P = .314), lens thickness (Pearson 0.26, P = .263), central anterior chamber depth (Pearson 0.05, P = .815), or sclerochoroidal layer thickness (Pearson −0.33, P = .169) ( Figure 3 ). Total axial length also had a strong positive correlation with length of the vitreous compartment (Pearson 0.99, P < .0001) and a negative correlation with degree of hyperopia (Pearson −0.81, P < .0001) ( Figure 3 ). Results of statistical analysis for left eye were similar ( Supplemental Figure , available at AJO.com ).
Genetic Features
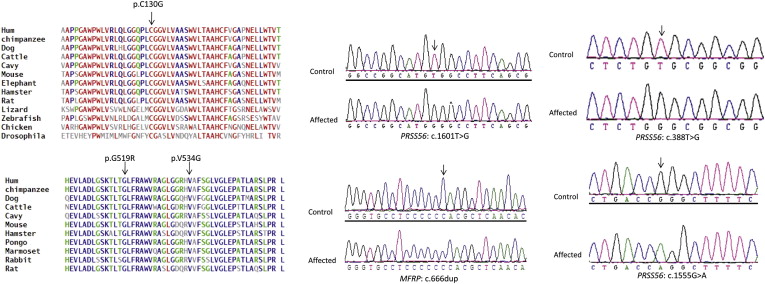
A homozygous PRSS56 mutation was present in 8 of 13 families (19 patients) ( Table 2 ). A previously reported PRSS56 truncating mutation c.1066dupC (p.Q356pfsX152) was detected in 5 unrelated families (Families 2, 4, 5, 8, and 10). The other 3 PRSS56 mutations were novel and found in 3 unrelated families: p.G519R (c.1555G>A, in Family 3), p.C130G (c.388T>G, in Family 6), and p.V534G (c.1601T>G, in Family 12) ( Table 2 ). These missense mutations were not identified in 96 normal Saudi control DNA samples (192 chromosomes). Polyphen-2 and SIFT analysis predicted these variants to be probably damaging (Polyphen-2 score 0.95) and affecting protein function, respectively. The protein alignments affected by all 3 changes showed very strong conservation among different species ( Figure 4 , Left). A homozygous mutation in MFRP was present in each of 2 families: the previously reported mutation in the Indian family (Family 1) and a novel truncating mutation (c.666dup, p.T223H fs X16) in 1 Saudi family (Family 13) ( Figure 4 , Right). In the remaining 3 families (Families 7, 9, and 11) no pathogenic variants were identified in either PRSS56 or MFRP ( Table 2 ).
| Family Number-Patient Number | Genetic Mutation | Type of Mutation | Novel vs Previously Reported Mutation | Where the PRSS56 or MFRP Mutation was Determined for This Patient | Additional Information |
|---|---|---|---|---|---|
| F1-P1 | MFRP: c.[1549C>T];[1549C>T], p.[R517W];[R517W] | Missense | Aldahmesh et al | Aldahmesh et al | Polyphen-2 prediction: probably damaging with a score of 1.0 |
| F2-P2 | PRSS56: c.[1066dupC];[1066dupC],p.[Gln356ProfsX152];[Gln356ProfsX152] | Frameshift | Gal et al | This study | |
| F3-P3,4,5,6,7 | PRSS56: c[c.1555G>A];[ c.1555G>A], p.[G519R];[G519R] | Missense | Novel | This study | Polyphen-2 prediction: probably damaging with a score of 0.95 |
| F4-P8 | PRSS56: c.[1066dupC];[1066dupC],p.[Gln356ProfsX152];[Gln356ProfsX152] | Frameshift | Gal et al | This study | |
| F5-P9,10,11 | PRSS56: c.[1066dupC];[1066dupC],p.[Gln356ProfsX152];[Gln356ProfsX152] | Frameshift | Gal et al | This study | |
| F6-P12 | PRSS56: c.[c.388T>G];[c.388T>G], p.[C130G];[C130G] | Missense | Novel | This study | Polyphen-2 prediction: probably damaging with a score of 0.95 |
| F7-P13 | No detectable mutation in MFRP or PRSS56 | – | – | – | No overlapping ROH with PRSS56 or MFRP |
| F8-P14,15,15,17 | PRSS56: c.[1066dupC];[1066dupC],p.[Gln356ProfsX152];[Gln356ProfsX152] | Frameshift | Gal et al | This study | |
| F9-P18 | No detectable mutation in MFRP or PRSS56 | – | – | – | No overlapping ROH with PRSS56 or MFRP |
| F10-P19,20 | PRSS56: c.[1066dupC];[1066dupC],p.[Gln356ProfsX152];[Gln356ProfsX152] | Frameshift | Gal et al | This study | |
| F11-P21,22 | No detectable mutation in MFRP or PRSS56 | – | – | – | No overlapping ROH with PRSS56 or MFRP |
| F12-P23,24 | PRSS56: c.[1601T>G];[1601T>G],p.[V534G];[V534G] | Missense | Novel | This study | Polyphen-2 prediction: probably damaging with a score of 0.95 |
| F13-P25 | MFRP: c.[666dup];[666dup], p.[T223HfsX16];[T223HfsX16] | Frameshift | Novel | This study |
Genotype and Phenotype
Although minor intra-familial variations did occur, the 5 families with the truncating mutation in PRSS56 exhibited shorter mean axial length (15.72 mm [15.21-16.50]), higher mean corneal power (49.63 D [47.94-51.16]), smaller mean corneal diameter (11.12 mm [10.00-12.00]), and higher mean hyperopia (+16.42 D [14.00-18.75]) than the eyes in this cohort with a PRSS56 missense mutation (16.37 mm, 48.37 D, 11.69 mm, and +14.55 D, respectively) or no identified mutation (17.57 mm, 47.48 D, 11.78 mm, and +12.91 D, respectively) (summarized data are for the right eye and are shown in Table 3 ). Eyes with PRSS56 truncating mutations (axial lengths 15.21-16.50 mm) also tended to exhibit thicker papillomacular folds. The 3 families with missense PRSS56 mutations had biometry values within the middle ranges of our cohort (OD mean AL of 16.37 mm, mean corneal power of 48.37 D, mean corneal diameter of 11.69 mm, and mean hyperopia of +14.55 D) and most had moderately thick papillomacular folds ( Table 3 ). The Indian patient with missense MFRP mutation had axial lengths, corneal diameters, and powers that fell in the middle range of our cohort, with a moderate papillomacular fold, whereas the Saudi patient with the truncating MFRP mutation exhibited a severe phenotype indistinguishable from those attributable to PRSS56 truncating mutations in terms of biometry and thickness of papillomacular folds ( Table 3 ). Two of the 3 families without identifiable mutation had either a mild phenotype (Families 7 and 9) with longer axial length (mean 19.55 mm), lower corneal power (mean 43.09 D), larger corneal diameter (mean 12.55 mm), lower degrees of hyperopia (mean 10.25 D), and only fine papillomacular wrinkles. The third had a severe phenotype (Family 11) with short axial length (mean 15.52 mm), steeper cornea (mean 51.88 D), smaller corneal diameter (mean 10.93 mm), higher hyperopia (mean 15.50 D), and a thick papillomacular fold ( Table 3 ). The results for left eye were similar and are shown in Supplemental Table 2 (available at AJO.com ).
| Truncating PRSS56 Mutations 5 Families/11 Patients (n = 11) | Missense PRSS56 Mutations 3 Families/8 Patients (n = 8) | MFRP Mutations 2 Families/2 Patients (n = 2) | No Detectable PRSS56 or MFRP Mutations (Severe Phenotype) 1 Family/2 Patients (n = 2) | No Detectable PRSS56 or MFRP Mutations (Mild Phenotype) 2 Families/2 Patients (n = 2) | |
|---|---|---|---|---|---|
| Refractive error (D) (range) mean | (14.00-18.75) 16.42 | (12.88-16.50) 14.55 | (12.38-16.25) 14.31 | (13.50-17.50) 15.50 | (09.88-10.75) 10.31 |
| Corneal power (D) (range) mean | (47.94-51.16) 49.63 | (47.44-49.60) 48.37 | (49.75-49.69) 49.72 | (51.50-52.25) 51.88 | (41.91-44.28) 43.09 |
| Corneal diameter (mm) (range) mean | (10.00-12.00) 11.12 | (11.00-12.25) 11.69 | (11.50-11.10) 11.30 | (10.60-11.25) 10.93 | (12.00-13.25) 12.63 |
| Axial length (mm) (range) mean | (15.21-16.50) 15.72 | (15.58-17.07) 16.37 | (16.56-15.64) 16.10 | (14.88-16.16) 15.52 | (19.37-19.88) 19.63 |
Results
Clinical Features
Twenty-five affected patients (2-47 years of age, 14 male and 11 female) from 13 families were enrolled. Linkage analysis for 7 of these families was previously reported. All families were Saudi Arabian except 1, which was South African of Indian descent (Family 1). Seven of the 12 Saudi Arabian families were consanguineous. With the exception of Family 4, all affected subjects had unaffected parents, whose eyes had no or very minor refractive errors. All patients had hyperopia of ≥8 D, axial length <20 mm, characteristic full-thickness retinal papillomacular folds (in 23 patients) or wrinkles (in 2 patients), a grossly normal anterior segment, and no developmental ocular malformations or syndromic disease ( Figure 1 ). No patient had night blindness or clinical signs of retinal degeneration.
Best-corrected Snellen visual acuity ranged from 20/30 to 20/160. Intraocular pressure was normal in all eyes. The spherical equivalent of refractive errors ranged from +9.88 to +18.75 D (average +15.09) in the right eye (OD) and from +9.13 to +18.88 D (average +15.09) in the left eye (OS).
Biometrically, the 2 eyes of a given individual were similar. Patient data for the right eye are detailed in Table 1 and summarized below. Data for the left eye were similar and are available in Supplemental Table 1 (available at AJO.com ).
| Family-Pt. # | Age (y)/Sex (M/F) | Hyperopia Spherical Equivalent (D) | Horiz Corneal Diameter (mm) | Keratometry | Pachymetry | A-Scan | Papillomacular Fold | Genetic Mutation | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Manual K Average (D) | Orbscan K Average (D) | Overall K Average (D) | Corneal Thickness Average (μm) | Central AC Depth (mm) | Lens Thickness (mm) | Axial Vitreous Length (mm) | Globe AL (mm) | ||||||
| F1-P1 | 11/M | 12.38 | 11.50 | 50.00 | 49.50 | 49.75 | 547 | 2.99 | 4.27 | 9.30 | 16.56 | Moderate | MFRP |
| F2-P2 | 5/M | 17.63 | 10.00 | 50.63 | 51.70 | 51.16 | 537 | 2.64 | 4.39 | 7.81 | 15.21 | Thick | PRSS56 |
| F3-P3 | 21/F | 13.00 | 11.50 | 48.38 | 49.77 | 49.07 | 556 | 3.11 | 4.20 | 9.04 | 16.35 | Moderate | PRSS56 |
| F3-P4 | 23/F | 12.88 | 12.25 | 47.48 | 47.40 | 47.44 | 502 | 2.87 | 4.67 | 9.36 | 16.90 | Moderate | PRSS56 |
| F3-P5 | 21/F | 15.13 | 12.00 | 49.06 | 49.80 | 49.43 | 528 | 3.06 | 4.60 | 7.92 | 15.58 | Moderate | PRSS56 |
| F3-P6 | 20/M | 14.00 | 12.25 | 47.60 | 48.40 | 48.00 | 611 | 3.31 | 4.47 | 9.29 | 17.07 | Moderate | PRSS56 |
| F3-P7 | 13/F | 13.88 | 12.00 | 47.82 | 47.63 | 47.73 | 571 | 3.56 | 4.07 | 9.04 | 16.67 | Moderate | PRSS56 |
| F4-P8 | 14/M | 15.00 | 12.00 | 49.82 | na | 49.82 | na | 3.30 | na | na | 16.50 | Thick | PRSS56 |
| F5-P9 | 21/F | 17.00 | 11.00 | 50.38 | 50.50 | 50.44 | 593 | 2.93 | 4.34 | 8.05 | 15.32 | Moderate | PRSS56 |
| F5-P10 | 12/M | 16.50 | 12.00 | 49.00 | 47.75 | 48.37 | 573 | 3.44 | 3.99 | 8.47 | 15.90 | Thick | PRSS56 |
| F5-P11 | 8/F | 14.13 | 11.00 | 49.64 | 49.20 | 49.42 | 563 | 3.24 | 4.00 | 8.55 | 15.79 | Moderate | PRSS56 |
| F6-P12 | 25/M | 14.50 | 11.50 | 47.62 | 48.00 | 47.81 | 620 | 3.35 | 4.20 | 9.00 | 16.55 | Thick | PRSS56 |
| F7-P13 | 47/M | 9.88 | 12.00 | 44.25 | 44.30 | 44.28 | 514 | 2.99 | 4.54 | 12.35 | 19.88 | Wrinkles | Not detectable |
| F8-P14 | 23/M | 17.75 | 10.75 | 48.02 | 47.85 | 47.94 | 562 | 3.18 | 4.14 | 8.73 | 16.05 | Thick | PRSS56 |
| F8-P15 | 18/F | 16.75 | 10.50 | 50.20 | 50.35 | 50.27 | 597 | 3.37 | 4.07 | 8.42 | 15.86 | Thick | PRSS56 |
| F8-P16 | 16/F | 18.75 | 10.50 | 48.29 | 51.00 | 49.64 | 556 | 3.31 | 3.87 | 8.48 | 15.66 | Moderate | PRSS56 |
| F8-P17 | 3.5/M | 16.13 | 11.50 | 48.78 | 50.50 | 49.64 | 624 | na | na | na | 15.24 | Thick | PRSS56 |
| F9-P18 | 33/F | 10.75 | 13.25 | 42.13 | 41.70 | 41.91 | 531 | 3.12 | 4.34 | 11.91 | 19.37 | Wrinkles | Not detectable |
| F10-P19 | 10/F | 17.00 | 11.50 | 48.67 | na | 48.67 | na | 3.09 | na | na | 15.69 | Thick | PRSS56 |
| F10-P20 | 2/M | 14.00 | 11.60 | 50.57 | na | 50.57 | na | 2.79 | na | na | 15.65 | Thick | PRSS56 |
| F11-P21 | 9/M | 13.50 | 10.60 | 52.34 | 50.65 | 51.50 | 572 | 3.16 | 3.94 | 9.06 | 16.16 | Moderate | Not detectable |
| F11-P22 | 5/M | 17.50 | 11.25 | 52.25 | na | 52.25 | 469 | 3.18 | na | na | 14.88 | Thick | Not detectable |
| F12-P23 | 26/M | 16.50 | 11.00 | 48.11 | 47.65 | 47.88 | 571 | 3.05 | 4.72 | 8.58 | 16.16 | Moderate | PRSS56 |
| F12-P24 | 20/F | 16.50 | 11.00 | 49.85 | 49.35 | 49.60 | 580 | 2.94 | 4.56 | 8.18 | 15.68 | Moderate | PRSS56 |
| F13-P25 | 10/M | 16.25 | 11.10 | 49.49 | 49.90 | 49.69 | 613 | 3.19 | 4.15 | 8.30 | 15.64 | Thick | MFRP |
| Mean | 16.66 | 15.09 | 11.42 | 48.81 | 48.71 | 48.89 | 563 | 3.13 | 4.28 | 8.99 | 16.25 | ||
| Median | 16.00 | 15.13 | 11.50 | 49.00 | 49.35 | 49.43 | 567 | 3.14 | 4.24 | 8.66 | 15.90 | ||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


