Fig. 5.1
First patient operated with the Ferrara ring (postkeratoplasty high astigmatism)
The excellent tolerance to the implant by the transplanted cornea gave us the necessary confidence to apply the technique in keratoconic corneas. Therefore, we decided, in 1996, to implant the rings in patients intolerant to contact lenses that’s had the penetrating keratoplasty indicated (Fig. 5.2).
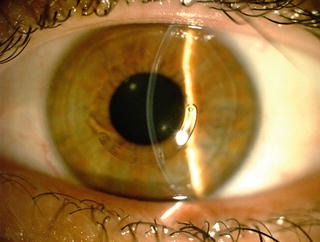
Fig. 5.2
Ferrara ring implanted in a patient with keratoconus
2.1 The Ferrara Ring Characteristics
The Ferrara ring has the following characteristics (Fig. 5.3):

Fig. 5.3
Flat basis (arrow) of the Ferrara ring
Total diameter (external) of 5.6 mm
Triangular section
600-micron base
Variable thickness
One or two 1,600 segments
One orifice in each extremity
Yellow PMMA
2.2 How the Ferrara Ring Works
The corneal ring complies with Barraquer and Blavatskaya postulates, according to those an addition in the cornea periphery results in its flattening, and the ring diameter determines how much the cornea will be flattened. Thus, the more tissue is added (increasing ring thickness), and the smaller the diameter, the greater will be the myopia correction obtained [20, 21].
Our study resulted in the additional observations presented below:
Central and peripheral flattening of the cornea, preserving its asphericity.
Decrease in the anterior chamber depth as shown in ultrasonic biomicroscopy.
Regularization of the corneal surface through a tilting movement caused by the flatness in the surface of the ring basis, making the cornea flattened at the areas corresponding to the segments extremities and making it curve at the ring’s body area.
Interruption or at least delay of keratoconus evolution, diminishing opacity on the cone apex, and reduction of related symptoms as itching, photophobia, and pain and/or ocular discomfort.
Lack of correspondence between visual acuity uncorrected after surgery and residual ametropia. Sometimes it can be observed with good vision coexisting with high residual refractive errors.
The prisma effect generated by the triangular section eliminates the halos and glare, which could result from the small diameter of the orthesis.
The yellow filter introduced in the plastic avoids the UV light to go into the eye reducing thus the halos and reflections at night.
2.3 Indications
The main indication for the Ferrara ring implantation is the keratoconus. In patients with keratoconus the Ferrara ring is indicated when there is evidence of progressive worsening of the disease, with gradual decrease of uncorrected visual acuity (UCVA) and best-corrected visual acuity (BCVA) and progressive corneal steepening. In patients with unsatisfactory BCVA with glasses and intolerance to contact lenses the Ferrara ring implantation is also indicated.
In post-LASIK corneal ectasia the Ferrara ring implantation is indicated when there is worsening of the condition. The main indications for the Ferrara ring implantation are listed in the Table 5.1.
Table 5.1
Ferrara ring indications
1. | Keratoconus |
2. | High irregular astigmatisms after penetrating or lamellar keratoplasty |
3. | Irregular astigmatisms after radial keratotomy |
4. | Pellucid marginal degeneration |
5. | Corneal ectasia after excimer laser |
2.4 Contraindications
The main contraindications for Ferrara ring implantation is the presence of apical opacities in very advanced keratoconus, usually with K readings above 75 D. The postoperative results in these cases are usually poor, and the best treatment for these cases is the lamellar or penetrating keratoplasty. The main contraindications for the Ferrara ring implantation are listed in the Table 5.2.
Table 5.2
Ferrara ring contraindications
1. | Very advanced keratoconus with curvatures over 75 diopters and significant apical opacity and scarring |
2. | Hydropsis |
3. | Thin corneas, with thickness below 300 microns in the ring track |
4. | Patients with intense atopia (these should be treated before the implant) |
5. | Any ongoing infectious process, local or systemic |
2.5 Nomogram
The nomogram has evolved as the knowledge about the predictability of results has grown. Initially, surgeons implanted a pair of symmetrical segments in every case. The incision was always placed on the steep meridian to take advantage of the coupling effect achieved by the rings.
First, only the grade of keratoconus was considered for the ring selection, which means that in keratoconus grade I, the more suitable Ferrara ring for implantation was that of 150 μm and in the keratoconus grade IV, the more appropriate ring was of 350 μm (Table 5.3). However, some cases of extrusion could be observed; as in keratoconus grade IV, the cornea usually is very thin and the thick ring segment sometimes was not properly fitted into the corneal stroma.
Table 5.3
Dr. Paulo Ferrara original (first generation) nomogram
Diameter 5.00 mm | Thickness diopters to be corrected |
|---|---|
Frustre 0.150 mm | −2.00 to −4.00 |
Cone I 0.200 mm | −4.25 to −6.00 |
Cone II 0.250 mm | −6.25 to −8.00 |
Cone III 0.300 mm | −8.25 to −10.00 |
Cone IV 0.350 mm | −10.25 to −12.00 |
The second generation of the nomogram considered the refraction for the ring selection, besides the distribution of the ectatic area on the cornea. Therefore, as the spherical equivalent increased, the selected ring thickness also increased. However, in many keratoconus cases the myopia and astigmatism could not be caused by the ectasia itself but by an increase in the axial length of the eye (axial myopia). In these cases, a hypercorrection by implanting a thick ring segment in a keratoconus in which a thinner segment was indicated was observed.
In the third and actual generation of the Ferrara ring nomogram, the ring selection depends on the type of keratoconus, its location in the cornea (Fig. 5.4), corneal asphericity (Q), topographic astigmatism (Tables 5.4, 5.5, and 5.6), and pachymetry [22–24].
Fig. 5.4
Distribution of the area of corneal ectasia. The ectatic area is symmetrically distributed on the cornea
Table 5.4
Segment thickness choice in symmetric bow tie keratoconus
Topographic astigmatism (D) | Segment thickness |
|---|---|
<1.00 | 150/150 |
1.25–2.00 | 200/200 |
2.25–3.00 | 250/250 |
>3.25 | 300/300 |
Table 5.5
Asymmetrical segment thickness choice in sag cones with 0/100 and 25/75 % of asymmetry index (Fig. 5.1)
Topographic astigmatism (D) | Segment thickness |
|---|---|
<1.00 | None/150 |
1.25–2.00 | None/200 |
2.25–3.00 | None/250 |
3.25–4.00 | None/300 |
4.25–5.00 | 150/250 |
6.25–6.00 | 200/300 |
Table 5.6
Asymmetrical segment thickness choice in sag cones with 0/100 and 33/66 % of asymmetry index (Fig. 5.1)
Topographic astigmatism (D) | Segment thickness |
|---|---|
<1.00 | None/150 |
1.25–2.00 | 150/200 |
2.25–3.00 | 200/250 |
3.25–4.00 | 250/300 |
For symmetric bow tie patterns of keratoconus, two equal segments are selected. For nipple cones, a single 210 μm segment is chosen based on the nomogram (Table 5.7). For peripheral cones, the most common form type, asymmetrical segments are selected. It is important to emphasize that the ring segment thickness cannot exceed 50 % of the thickness of the cornea on the track of the ring.
Table 5.7
Segment thickness choice in nipple cones (210/m ring)
Spherical equivalent (D) | Segment thickness |
|---|---|
Up to 2.00 | 150 |
2.25–4.00 | 200 |
4.25–6.00 | 250 |
>6.25 | 300 |
Table 5.8
Ferrara ring nomogram: step by step
1. | Define the keratoconus type: sag, bow tie or nipple |
2. | Distribution of the ectatic area in the cornea: 0/100, 25/75, 50/50, and 33/66 |
3. | Corneal asphericity (Q) |
4. | Topographic astigmatism |
5. | Pachymetry at incision site and ring track |
The first step in ring selection is to define the type of keratoconus of the patient: sag, bow tie, or nipple. After, it is determined the distribution of the keratoconus in the cornea: central (nipple and bow tie) or paracentral (asymmetric) (0/100, 25/75, and 33/66; Fig. 5.2). The next step is to evaluate the preoperative corneal asphericity value (Q), which is desirable but not indispensable, as most corneal topographers do not show this data. However, preliminary data shows that the corneal asphericity may be linked to the quality of vision; therefore, when possible, this data should be obtained by corneal topographers (Orbscan and Pentacam) to achieve the best possible visual results. We have described (unpublished study) that for each ring segment there is a correspondent Q value reduction (Fig. 5.4). A target postoperative Q value closest possible of −0.23 is the goal after Ferrara ring implantation.
The topographic astigmatism defines the thickness of the rings to be implanted (Tables 5.4, 5.5, and 5.6). The only type of keratoconus that does not depend on the topographic astigmatism for ring selection is the nipple conus. In this case the spherical equivalent defines the thickness of the ring to be implanted, which should be a 210-arc ring, which is indicated exclusively for this type of keratoconus [20].
The pachymetry at the incision site (steep axis of the cornea) must be determined. The incision depth must be 80 % of the cornea thickness at the incision site. The pachymetry should be measured in all ring tracks to avoid superficial rings, which could lead to future extrusion.
2.6 Surgical Technique
2.6.1 Manual Technique
The surgery is performed under topical anesthesia after miosis achieved with 2 % pilocarpine. An eyelid speculum is used to expose the eye, and a 2.5 % povidone–iodine eyedrops is instilled into the cornea and conjunctival cul-de-sac. The visual axis is marked by pressing the Sinskey hook on the central corneal epithelium while asking the patient to fixate on the corneal light reflex of the microscope light. Using a marker tinted with gentian-violet, a 5.0 mm optical zone and incision site are aligned to the desired axis in which the incision will be made. This site can be the steepest topographic axis of the cornea (in case of implantation of two segments) or 900 (in case of implantation of only one segment—one of the tips of the ring must be located on the steepest axis).
The depth of a 1.0 mm square diamond blade is set at 80 % of corneal thickness at the incision site, and this blade is used to make the incision. Using a “stromal spreader,” a pocket is formed in each side of the incision. Two (clockwise and counterclockwise) 2,700 semicircular dissecting spatulas are consecutively inserted through the incision and gently pushed with some, quick, rotary “back and forth” tunneling movements. Following channel creation, the ring segments are inserted using a modified McPherson forceps. The rings are properly positioned with the aid of a Sinskey hook.
2.6.2 Femtosecond Laser Technique
The femtosecond laser (IntraLase Corp.) has been recently introduced in clinical practice whose surgical effect via photodisruption can be used as an alternative to traditional mechanical techniques. Several recent papers [25–28] have reported its efficacy and safety for tunnel creation and intrastromal rings implantation. The femtosecond laser can easily and quickly create a predetermined depth and channel size.
There is controversy over channel size nomograms with the technique. Some authors conclude that more effects can be achieved by making the stromal channels narrower than the ring size, leading to faster visual results [29].
The use of the femtosecond laser in corneal tunnel creation made the procedure faster, easier (especially for inexperienced surgeons), and more comfortable for the patient. However, the main advantage of IntraLase-assisted channel creation over the mechanical technique seems to be the precise depth of implantation. The only advantage of this technique is the cost of the equipment, which is high.
The technique: tunnel depth is set at 80 % of the thinnest corneal thickness on the tunnel location in the femtosecond laser. Special attention must be given in centralizing the disposable suction ring to mark the central point to minimize decentration. The channel’s inner diameter is set to 4.4 mm, the outer diameter 5.6 mm, the entry cut thickness is 1 m (at the steepest topographic axis), the ring energy used for channel creation is 1.30j, and the entry cut energy is 1.30j. Channel creation timing with the femtosecond laser is 15 s. The intracorneal ring segments are implanted immediately after channel creation before the disappearance of the bubbles, which reveals the exact tunnel location. The segments are placed in the final position with a Sinskey hook through a dialing hole at both ends of the segment.
The postoperative regimen, for both techniques, consists of moxiloxacin 0.5 % (Vigamox®, Alcon, USA) and dexamethasone 0.1 % (Maxidex®, Alcon, USA) eyedrops four times daily for two weeks. The patients were instructed to avoid rubbing the eye and to use preservative-free artificial tears frequently—Polyethylene Glycol 400 0.4 % (Oftane®, Alcon, USA).
2.7 Clinical Results: Long-Term Follow-Up in Keratoconus [21]
We retrospectively reviewed patient records of 94 eyes of 76 patients, which were consecutively operated (Ferrara ring implantation). There were 33 females and 61 males. The average age of the patients was 28.1 years. All procedures were performed by the same surgeon (PF), between June of 1996 and September of 2007. Patients included in the study presented clear cornea and a minimal corneal thickness of 300 μm at the ring track. Patients were intolerant to contact lens and/or showed progression of the ectasia.
Fifty-eight subjects underwent to a single eye treatment, whereas 18 subjects had both eye treated. Seventy-three eyes had a 2-year follow-up, 66 eyes had a 3-year follow-up, 48 eyes had a 4-year follow-up, and 34 eyes had a 5-year follow-up. All patients completed at least a 2-year follow-up. No intraoperative complications occurred during the procedures. All patients returned for ocular examination on day one, 1 week, and a month after the surgery and then 3, 6, and 12 months. Thereafter, the following eye examinations occurred yearly.
Preoperative and postoperative UCVA, BSCVA, and keratometry data were collected from all patients. The mean UCVA at the preoperative period was 0.12, and the mean BSCVA was 0.41. At the first month, the mean UCVA improved to 0.25, and the mean BSCVA improved to 0.56. At the second-year follow-up, the mean UCVA improved from 0.12 preoperatively to 0.29. At the third-year follow-up, the mean UCVA improved to 0.34; at the fourth-year follow-up, the mean UCVA improved to 0.42; and at the fifth-year follow-up, the mean UCVA decreased to 0.31 postoperatively. The mean BSCVA, at the 1st month, improved to 0.56. At the second-year follow-up, the mean BSCVA improved from 0.41 preoperatively to 0.68. At the third-year follow-up, the mean BSCVA decreased to 0.63; at the fourth-year follow-up, the mean BSCVA improved to 0.65; and at the fifth-year follow-up, the mean BSCVA decreased to 0.59 postoperatively (Fig. 5.5).
Fig. 5.5
Q (asphericity) variation according to ring thickness
Mean keratometry decreased significantly from the preoperative to the last postoperative follow-up. Preoperative mean keratometry was 50.36, which de creases to 47.29 at 1st month postoperative follow-up. The mean keratometry follow-up along the second to fifth years was 45.96, 45.83, 46.44, and 46.24, respectively. The topography showed a decrease in the corneal steepening at the postoperative period, flattening of the central cornea, and displacement of the central cornea.
As showed in previous studies the intrastromal ring flattens the cornea and keeps this effect for a long period of time. There is no significant re-steepening of the cornea over time.
The present study showed that the Ferrara ring, despite the small sample of patients, can be a valuable tool to provide topographic and visual stability, delay the progression of keratoconus, and postpone a corneal grafting surgery to a more physiological position.
2.8 Clinical Results: The 210 Ferrara Ring [20]
The 210° of arc Ferrara intrastromal ring (210-FICR), which is a novel FICR, has three major advantages over the conventional ring: (1) minimal astigmatic induction, (2) corneal flattening, and (3) implantation of a single segment. This ring is especially useful for the nipple type of keratoconus. The 210-FICR is an efficient method for keratoconus correction, significantly decreasing the keratometric values and spherical equivalent and improving UCVA and BCVA.
We retrospectively reviewed patient records of 80 eyes of 76 patients, which were consecutively operated, in which the 210-FICR was implanted. Statistical analysis included preoperative and postoperative uncorrected visual acuity (UCVA), best-corrected visual acuity (BCVA), spherical equivalent, and keratometry.
The mean follow-up time was 6.65 months. The mean UCVA increased from 20/350 to 20/136 (p = 0.001). The mean BCVA increased from 20/125 to 20/55 (p = 0.0001). The mean preoperative spherical equivalent decreased from −5.22 D, preoperative, to −2.26 D (p = 0.050), postoperative.
Corneal tomography (Pentacam^) showed corneal flattening in all eyes.
The mean K1 decreased from 51.49 D to 47.40 D (p = 0.00014), and the mean K2 decreased from 54.33 D to 49.14 D (p = 0.00022). The mean keratometric astigmatism decreased from 3.65 D (preoperative) to 2.69 D (postoperative) (p = 0.0001).
2.9 Clinical Results: Post-Refractive Surgery Corneal Ectasia [30]
Twenty-five eyes of 20 patients with corneal ectasia (13 males [15 eyes] and 7 females [10 eyes]) who underwent Ferrara intracorneal ring segments (ICRS) implantation were included in this study.
The mean follow-up time was 39.8 ± 21.1 months (Table 5.1). All patients were implanted only one segment of ICRS in l8 eyes and the 210° of arc (210—ICRS) ring was implanted in 7 eyes.
The mean UDVA increased from 20/185 to 20/66 (p = 0.005). The mean CDVA increased from 20/125 to 20/40 (p = 0.008) (Fig. 5.4). The mean asphericity values decreased from −0.95, preoperatively, to −0.23 (p = 0.006), postoperatively.
The mean pachymetry at the apex of the cornea increased from (mean) 457.7 ± 48.7^m (range 361–542) to 466.2 ± 49.8^m (range 381–559) (p = 0.025), and the pachymetry at thinnest point of the cornea increased from 436.3 ± 46.2^m (range 348–533) to 453.9 ± 49.3^m (range 370–548) (p = 0.000). A significant reduction in keratometric values was found at the last follow-up examination; mean preoperative keratometry was decreased from 45.41 ± 5.63 D (range 37.3–55.5) and changed significantly to 42.88 ± 4.44D (range 31.2–54.1) (p = 0.000) (Fig. 5.5).
Our postoperative results show a significant improvement in UDVA and CDVA. Moreover, there was significant increase in corneal thickness. This can be explained by a theoretically cornea collagen remodeling induced by the implantation of ICRS.
We found a significant decrease in asphericity values after implantation of ICRS in this study. Interestingly, the mean postoperative value was −0.23, which is considered the “normal” value for the general population. This value means that the normal physiologic asphericity of the cornea shows a significant individual variation ranging from mild oblate to moderate prolate. In an unpublished study, where we evaluated the corneal asphericity changes induced by the ICRS in keratoconus, we found that the Ferrara intrastromal ring implantation significantly reduced the mean corneal asphericity from −0.85 to −0.32. It is well known that most corneas after ablation laser procedures tend to become oblate, and when the ectasia develops, these corneas usually become prolate. However, the excess of prolatism usually found in keratoconus (primary) is usually of a much larger amount that one found in post-refractive surgery ectasia. That is the probable reason the Q value after FICR becomes much closer to “normal” values than when the ring is used for keratoconus. As the asphericity is one of the markers of visual quality, turning it “normal” can be a predictor of improvement of visual quality.
The keratometry values reduced significantly in all eyes. It can be realized that the mean preoperative values are usually lower than the ones found in keratoconus (primary). This can be explained somewhat by the corneal flattening induced by the refractive procedure, usually in an optic zone of greater extent than the location of the ectasia.
Most of the implanted ICRS were 160-FICR, the “conventional” ring. The remainder of the eyes received the 210-ICRS. The latter is usually reserved for central cones of nipple type. Some ectasia assumes the same topographical pattern of nipple cones, in which we usually use the 210-FICR with excellent results [17]. This ring is reserved for cases with low astigmatism, in which we desire to flatten the cornea with minimal astigmatic induction.
The potential advantages of ICRS implantation over keratoplasty in eyes with post-LASIK ectasia are many. First, it avoids further laser treatment, eliminating central corneal wound healing. This leaves the optical center of the cornea untouched, enhancing the refractive outcome. Second, the technique is reversible in cases of unsatisfactory refractive or clinical outcomes, and minimal postoperative care is required. Third, adjustment can be performed using thinner or thicker rings. In cases of unexpected corneal shape changes, 1 segment can be removed or exchanged. Fourth, it avoids the complications of intraocular surgery.
2.10 Clinical Results: Endothelium Evaluation [31]
We retrospectively reviewed patient records of 102 eyes of 81 patients, which were followed for a period of at least 1 year (mean follow-up, 45.7 months; SD, 16.4 months; range, 13–71 months). All patients had the diagnosis of keratoconus, post-LASIK ectasia, or pellucid degeneration. Statistical analysis included preoperative and postoperative keratometry and endothelial characteristics (cell count, average cell size, and coefficient of variation).
All patients completed at least 1 year of follow-up (range 13–71 months). Mean age was 30.5 ± 8 years. The mean cell count decreased from (mean ± SD) 2,714 ± 372 to 2,562 ± 406 cells/mm2 (p < 0.001). The calculated exponential cell loss rate over the mean interval follow-up (4 years) was l.4 % per year. The average cell size increased from (mean ± SD) 375 ± 56 μ2 to 399 ± 61/2 (p < 0.001). The coefficient of variation increased from (mean ± SD) 0.22 ± 0.075 to 0.26 ± 0.010 (p = 0.001). All corneas remained clear during the follow-up period.
The mean maximum cell size increased from (mean ± SD) 529 ± 116 to 639 ± 225 μ2 (p < 0.001). The mean minimum cell size varied from (mean ± SD) 225 ± 36 to 226 ± 54 μ2 (p = 0.936).
There was significant corneal flattening as showed by keratometry changes. The mean K decreased from 47.70 ± 2.29 (range 43.70–53.80) to 44.86 ± 2.02 (range 41.20–51.20) (p = 0.0001).
In our study we found a 1.4 % loss of endothelial cells per year. Considering that most of the studied patients were young, the rate of endothelial cell loss was slightly higher than in normal eyes (1.1 %). Moreover, there is no study in the current literature that shows the profile of the “normal” endothelial loss in keratoconus corneas, which could be higher than in normal corneas. The only report in the literature regarding the endothelium profile of keratoconus is non-prospective and studied only 12 eyes [32].
Endothelial cell loss after penetrating keratoplasty is known to be an ongoing process even years after surgery. It is well known that the cell loss is higher in the early time course after surgery and decreases 3–5 years after surgery. There is a great variation of rates of cell loss after PK, ranging from 4.2 [33] to 9.4 % [34] per year, at the long-term follow-up. Even after DALK, which is a surgical technique that spares the receptor endothelium, cell loss has been reported [19]. In one study, a decrease in average endothelial cell count from preoperative of approximately 200 cells/mm2 was observed during the first 12 months after surgery.
The only study [35], which assessed the endothelial after intrastromal rings (Intacs, Addition Technology Inc) implantation reported that at 24 months after surgery, all corneal regions had a slight decrease in cell density. In all eyes, the mean central and peripheral endothelial cell counts remained above 2,495 cells/mm2. Our results are similar; we obtained a higher average postoperative cell count (2,562 cells/mm2), and we had a longer follow-up (4 years).
Woolensak et al. [36] in a collagen cross-linking study in keratoconus showed that the corneal transparency and the endothelial cell density (p = 0.45) remained unchanged. The follow-up was 23 months, and the sample was only 23 eyes. The same author, in an experimental study in rabbits [27], showed that riboflavin-UVA treatment should be safe as long as the dose is less than the endothelial cytotoxic dose of 0.65 J/cm2. In human corneas the endothelial cytotoxic UVA dose is reached in corneas thinner than 400, which is not uncommon in keratoconus patients. Moreover, the data obtained from normal corneas of rabbit cannot be extrapolated to human keratoconic corneas, which can have a different metabolism and response to cross-linking. The study has a limitation of measuring the endothelial toxicity only at 4 and 24 h after treatment. The long-term endothelial cytotoxicity was not evaluated by the study.
Our study suggests that some endothelial changes occur after Ferrara ring implantation. However, these changes are minimal and nonclinically significant, since the endothelial cell loss rate is not much higher than the normally expected for normal corneas. In contrast, the long-term endothelial cell loss after other therapies for keratoconus is much higher (as in PK, or even DALK, in which the receptor endothelium is spared) or unknown (as in cross-linking).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


