This article outlines the biology of human papillomavirus (HPV) infection of human mucosa and the cellular pathways that are altered through viral infection. The article provides a conceptual framework with which to understand the 2 major immunologic strategies to address HPV-related diseases: (1) prevention of primary HPV infection through the use of prophylactic vaccines and (2) treatment of established infection and diseases through therapeutic vaccines. Nonimmunologic therapy that targets cellular dysregulation induced by HPV infection is also discussed. The challenges in actualizing these conceptually attractive therapies on both a societal and biological level are examined.
- •
Human papillomavirus (HPV)–related cancers result from the failure of the immune system to recognize and eliminate virus-infected cells.
- •
The lifetime exposure risk of HPV infection is high, but most individuals are able to clear the infection within 2 years.
- •
HPV-16 is one of the viral types to be cleared the slowest in men and is responsible for more than 90% of HPV-related head and neck cancers in the United States.
- •
Established HPV infections are naturally cleared through T-cell–mediated immune responses (CD4+ and CD8+ T cells) rather than humoral antibody responses.
- •
Therapeutic DNA vaccines induce T-cell responses against HPV-infected cells and, therefore, may play an important role in treating patients with established HPV-related diseases.
Incidence of human papillomavirus infection
| ACIP | Advisory Committee on Immunization Practices |
| CDC | Centers for Disease Control |
| CIN | Cervical intraepithelial neoplasia |
| CTL | Cytotoxic T lymphocyte |
| IFN | Interferon |
| IL | Interleukin |
| IRF | Interferon Regulatory Factor |
| mAb | Monoclonal antibody |
| MHC | Major histocompatibility complex |
| VLP | Viral like proteins |
| RRP | Recurrent respiratory papillomatosis |
Most HPV infections are cleared by the immune system within 2 years, defined as an absence of HPV DNA detection on follow-up serial swabs after detection of the initial infection. At 12 months, 66% of infections are cleared; this increases to 90% at 24 months. However, in men, HPV-16 has been identified as one of the slowest viral types to be cleared, and takes nearly 2 times longer to be cleared than other high-risk viral types. This is an interesting finding because HPV-16 is the viral type that accounts for more than 90% of HPV-related oropharyngeal cancers in the United States, and this disease is more prevalent in men than in women, suggesting possible gender differences in the ability to mount immunologic responses against this viral type.
Persistent oral HPV infection is a risk factor for the development of HPV-related oropharyngeal cancers. The prevalence of any HPV type in the oral cavity for both men and women is approximately 6.9%. However, when separated by gender, it is significantly higher in men (10%) than in women (3.6%). Oral HPV infection is associated with certain sexual behaviors, with risk increasing with the number of lifetime oral sex partners. In healthy individuals, the clearance rate for oral HPV infection at 6 months is approximately 40%.
Biology of HPV infection
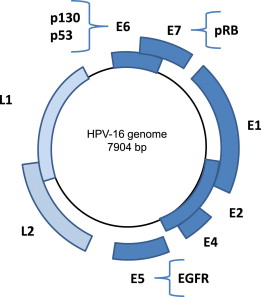
HPVs are small, nonenveloped DNA viruses with a double-stranded genome that encodes 6 early proteins (E1, E2, E3, E4, E5, E6, and E7) and 2 late proteins (L1 and L2), which are named based on their temporal expression pattern in the viral life cycle ( Fig. 1 ).
Replication Cycle
The replication cycle of HPV has been well studied in the epithelium of the cervix, and has been found to be tightly linked to the differentiation of the epithelium that it infects. After infection of the undifferentiated epithelial cells within the basal cell layer, the E1 and E2 proteins are expressed and regulate viral replication and expression of the other early viral genes. As the infected cell migrates toward the superficial layers of the squamous epithelium, the E6 and E7 oncogenes are expressed and modify the cell cycle to retain the differentiating host keratinocyte in a state that is favorable for amplification of the viral genome. The E6 oncoprotein ubiquitinates p53, thereby flagging it for proteosomal degradation via the ubiquitin-proteasome pathway. The E7 protein competes for binding with E2F to the hypophosphorylated active form of the retinoblastoma tumor suppressor gene product, pRB, thus releasing the transcription factor E2F to bind and activate its targets to facilitate cell cycle progression. The binding affinity of E6 and E7 to p53 and pRB, respectively, differentiates the low and high risk types of HPV, which is based on the risk of the infected cell progressing to malignant transformation.
Expression of Late Proteins
On cellular differentiation to the granular epithelial layer, the late proteins, L1 and L2, which consist of the major and minor capsid proteins respectively, are expressed and encapsulate the newly synthesized viral genomes. L1 spontaneously forms pentamers that assemble with the L2 protein to form the viral capsule. These capsid proteins are linked by disulfide bonds to provide structural stability and protection against environmental insults when the virus is shed from the superficial epithelium. The L2 protein is highly conserved among viral types, and is exposed during binding to a cell surface receptor during initial infection, which completes the viral lifecycle.
Infection of Tonsils
In the head and neck region, HPV infects the basal cell layer of the reticulated squamous epithelium of the deep crypts within the lingual and palatine tonsils. The reticulated epithelium is a modified form of stratified squamous epithelium, which contains lymphocytes, plasma cells, macrophages, and interdigitating cells that migrate between the reticulated epithelium and underlying lymphoid stroma. Therefore, the basement membrane of the squamous epithelium lining the deep crypts is disrupted to allow for passage of lymphocytes and antigen-presenting cells from the external environment of the oropharynx to the tonsillar lymphoid tissue. Based on the function of the tonsil, its microanatomy leaves the basal cell layer vulnerable to HPV infection.
Biology of HPV infection
HPVs are small, nonenveloped DNA viruses with a double-stranded genome that encodes 6 early proteins (E1, E2, E3, E4, E5, E6, and E7) and 2 late proteins (L1 and L2), which are named based on their temporal expression pattern in the viral life cycle ( Fig. 1 ).
Replication Cycle
The replication cycle of HPV has been well studied in the epithelium of the cervix, and has been found to be tightly linked to the differentiation of the epithelium that it infects. After infection of the undifferentiated epithelial cells within the basal cell layer, the E1 and E2 proteins are expressed and regulate viral replication and expression of the other early viral genes. As the infected cell migrates toward the superficial layers of the squamous epithelium, the E6 and E7 oncogenes are expressed and modify the cell cycle to retain the differentiating host keratinocyte in a state that is favorable for amplification of the viral genome. The E6 oncoprotein ubiquitinates p53, thereby flagging it for proteosomal degradation via the ubiquitin-proteasome pathway. The E7 protein competes for binding with E2F to the hypophosphorylated active form of the retinoblastoma tumor suppressor gene product, pRB, thus releasing the transcription factor E2F to bind and activate its targets to facilitate cell cycle progression. The binding affinity of E6 and E7 to p53 and pRB, respectively, differentiates the low and high risk types of HPV, which is based on the risk of the infected cell progressing to malignant transformation.
Expression of Late Proteins
On cellular differentiation to the granular epithelial layer, the late proteins, L1 and L2, which consist of the major and minor capsid proteins respectively, are expressed and encapsulate the newly synthesized viral genomes. L1 spontaneously forms pentamers that assemble with the L2 protein to form the viral capsule. These capsid proteins are linked by disulfide bonds to provide structural stability and protection against environmental insults when the virus is shed from the superficial epithelium. The L2 protein is highly conserved among viral types, and is exposed during binding to a cell surface receptor during initial infection, which completes the viral lifecycle.
Infection of Tonsils
In the head and neck region, HPV infects the basal cell layer of the reticulated squamous epithelium of the deep crypts within the lingual and palatine tonsils. The reticulated epithelium is a modified form of stratified squamous epithelium, which contains lymphocytes, plasma cells, macrophages, and interdigitating cells that migrate between the reticulated epithelium and underlying lymphoid stroma. Therefore, the basement membrane of the squamous epithelium lining the deep crypts is disrupted to allow for passage of lymphocytes and antigen-presenting cells from the external environment of the oropharynx to the tonsillar lymphoid tissue. Based on the function of the tonsil, its microanatomy leaves the basal cell layer vulnerable to HPV infection.
Cellular progression to dysplasia and cancer
Many HPV infections are either cleared by the immune system or result in latent infections of the basal cell layer, with low viral copy numbers maintained indefinitely, or until injury or immunosuppression induces active infection. Integration of viral DNA into the host genome is a strong predictor of risk of progression from viral infection to neoplastic disease. Late genes (L1 and L2) and some early genes (E1 and E2) are commonly deleted with viral integration and, with the disruption of E2 expression, there is unregulated expression of the E6 and E7 oncoproteins. Concurrently, E5 upregulates the expression of epidermal growth factor receptor (EGFR) within the cell, which leads to the overexpression of proto-oncogenes and repression of p21 (cyclin-dependent kinase inhibitor 1A) expression, a regulatory protein that controls cell apoptosis and differentiation. The interruption of cellular mechanisms that regulate apoptosis and the cell cycle results in dysregulated cell cycle proliferation, delayed cellular differentiation, increased frequency of spontaneous and mutagen-induced mutations, and increased chromosomal instability. Thus, the overexpression of the viral oncoproteins, E6 and E7, drives and maintains the neoplastic process.
Immune system and HPV
Several lines of evidence highlight the importance of a functioning immune system in controlling HPV infection and its associated neoplasms:
- 1.
Foremost is the observation that most immune-competent individuals infected with HPV are able to clear the infection without any clinical manifestation, and it is only 10% of infected individuals who develop HPV-related lesions.
- 2.
Histologic examination of spontaneously regressing HPV-related lesions shows infiltration of CD4+ and CD8+ T cells, whereas these immune cells are lacking in the lesions of patients with persistent disease. Immunocompromised individuals such as organ transplant recipients on immunosuppressive medications and patients infected with human immunodeficiency virus (HIV) have been documented to have significantly increased rates of HPV infections and of HPV-related diseases. Once these individuals stop their immunosuppressive medications or recover their immune cell counts, they are able to clear the infection and associated lesions.
- 3.
Preclinical studies have reported that animals immunized with vaccines that elicit HPV-specific CD8+ T cells show regression of established HPV-related cancers.
Humoral Immune Response
Clinically, systemic immune responses against HPV infection are often detected as humoral responses generated against the configured L1 pentamer, but this response is weak, inconsistent, and may not protect against future reinfection. For high-risk types, the seroconversion rate is only 30% to 50% following documented infection and, in patients with HPV-associated cancer, 30% to 50% have detectable antibody levels against the L1 protein from the causative viral type. If present, the antibody titers can persist for many years even after the infection is cleared, so seropositivity is a useful marker for past infection rather than current infection.
Humoral immune responses to the early viral proteins have also been detected. Patients with cervical cancer can have detectable antibodies to E7 and patients who have HPV-related head and neck cancer have detectable antibodies to E6 (Dr Sara Pai, unpublished data, 2012). Serum analysis for antibodies against the full viral proteome therefore has promise as a screening method for HPV-associated oropharyngeal cancer. However, patients with pure hypogammaglobulinemia seem to be at no higher risk of developing HPV-related diseases than patients with normal immune function, suggesting that humoral responses do not play a major role in clearing established HPV infections.
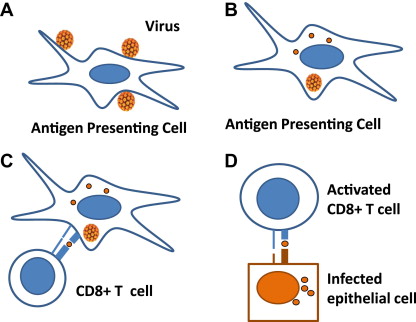
Cell-Mediated Immune Response
It is the cell-mediated immune responses, or HPV-specific CD4+ and CD8+ T cells, that are most critical in clearing established lesions ( Fig. 2 ). The virus-specific CD4+ and CD8+ T cells coordinate to clear chronic viral infections, and patients with evidence of previously cleared HPV-16 infections have strong detectable T-cell responses to viral proteins. Deficits in T-cell response have been documented in patients with cervical cancer and in patients with cervical intraepithelial neoplasia. The relative contributions to this lack of T-cell response from inherent host genetic factors and/or viral mechanisms to escape immune recognition are not known.
Viral mechanisms to evade the immune system
HPV has evolved multiple mechanisms to evade host immunologic responses, thereby leading to successful establishment of HPV-related lesions.
Coordination of Viral Replication to Cellular Differentiation
The first adaptive mechanism for escaping immune surveillance is the coordination of viral replication to cellular differentiation.
In the uterine cervix, within the organization of stratified squamous epithelium, the degree of immune surveillance decreases considerably in the superficial, keratinized layers. HPV takes advantage of this organization by tightly regulating its own replication with differentiation of the keratinocyte. The virus evades cytotoxic T lymphocyte (CTL) responses by expressing a minimal level of viral gene products in the keratinocytes of the basal cell layer and upregulates expression of viral gene products with differentiation and upward migration of keratinocytes, away from areas of active immune surveillance. In addition, HPV does not cause lysis of keratinocytes; virions are released through the mechanical breakage of surface epithelium and thereby minimize any associated inflammatory response. In this way, HPV replication is a local phenomenon with minimal systemic immune activation.
In the tonsil, HPV infects the reticulated epithelium lining the deep tonsillar crypts. Recent data suggest that the deep crypts of tonsils may be immune-privileged sites that can inhibit the effector function of HPV-specific T cells and thereby facilitate immune evasion at the time of initial HPV infection. This mechanism provides a biologic explanation of how a virus can infect a lymphoid organ, such as the tonsil and base of tongue, but still evade immune recognition and clearance (Lyford-Pike and colleagues, in preparation).
Inhibitory Effects of Viral Proteins
In addition to the local immunosuppressive microenvironment that HPV infects, the viral proteins also have local inhibitory effects on inflammatory cytokines to dampen both innate and adaptive immune responses. The HPV E5 and E7 proteins downregulate expression of the major histocompatibility complex (MHC) class I molecules, which inhibits viral antigen presentation to the immune system. E6 and E7 have also been shown to reduce expression of Toll-like receptor 9 and cytokines, such as interleukin (IL)-8 and IL-18, which are all potent proinflammatory molecules. A blunted response to interferon (IFN)-α and IFN-γ has also been observed in HPV infections. One mechanism for the blunted response is a reduction in the expression of IFN regulatory factor 1 (IRF-1), which is a transcription factor that mediates IFN responses. Because IFN signaling is a critical component in the activation of many aspects of both the innate and adaptive immune responses, as well as a potent antiproliferative agent, HPV thus disables a major mechanism of immune surveillance to oncogenic transformation.
Prevention of HPV infection through vaccination
Because the immune system is so important in controlling HPV infections and the lesions associated with these viruses, in the past decade vaccination programs against HPV have been initiated in the United States and other parts of the world.
Vaccines for the Prevention of Cancer
The discovery that the L1 viral proteins self-assemble into viral-like proteins (VLPs) in the absence of viral DNA was the critical first step in developing preventative vaccines. Recombinant techniques could then be used to produce hollow VLPs that could induce protective L1 antibody levels that can protect against new HPV infection without the risk of being exposed to an infectious virus ( Fig. 3 ).



