Human papillomavirus (HPV) is now recognized to cause a subset of head and neck squamous cell carcinomas (HNSCC). Although excessive tobacco and alcohol use continue to be important risk factors for HNSCC, epidemiologic studies suggest that more than 25% of HNSCC are now caused by HPV. The incidence of HPV-related HNSCC is increasing, highlighting the need to understand the oral HPV infections causing these cancers. This article reviews the evidence for a causal association between HPV and HNSCC, examines the changing epidemiologic trends of HNSCC, and discusses what is currently known about oral HPV infection, natural history, and transmission.
- •
In contrast to other head and neck cancers, the incidence of oropharyngeal malignancies has been increasing since the late 1970s, especially among younger men.
- •
The proportion of oropharyngeal cancers caused by human papillomavirus (HPV) is increasing; in many industrialized countries, up to 80% of oropharyngeal cancers are now caused by HPV.
- •
HPV-related head and neck squamous cell carcinomas (HNSCC) are more likely than HPV-unrelated HNSCC to occur in whites (93% vs 82%), never-drinker/never-smokers (16% vs 7%), those who have had more than 6 lifetime oral sexual partners (46% vs 20%), and those have a younger median age at cancer diagnosis (54 vs 60 years).
- •
The natural history of oral HPV infection is not well understood.
Introduction
Head and neck cancer (HNC) is a heterogeneous group of neoplasms that share a common anatomic origin. Although malignancies may arise from any tissue in the head and neck region, most tumors in this region develop from within the mucosa that lines the upper aerodigestive tract and are classified as squamous cell carcinomas. Head and neck squamous cell carcinomas (HNSCCs) include cancers in the oral cavity, oropharynx, nasopharynx, larynx, and hypopharynx.
Research over the past 15 years has shown that human papillomavirus (HPV) causes a subset of HNSCC, primarily oropharyngeal squamous cell carcinomas (OSCC). Although most HNSCCs are still caused by excessive tobacco and alcohol use, the incidence of HPV-related HNSCC (HPV-HNSCC) is increasing. In some regions, HPV is now the primary cause of oropharyngeal cancer.
In this article, we describe the changing epidemiology of HNSCC, examine the evidence supporting a causal association between HPV and HNSCC, and discuss what is currently known about oral HPV infection and natural history.
Epidemiology of HNC
Overview of HNC Epidemiology
There are more than 600,000 incident cases of HNC worldwide each year, including ∼263,020 oral cavity, 213,179 thyroid gland, 150,677 larynx, 136,622 pharynx, and 84,441 nasopharynx cases per year. Nasopharyngeal cancers are often considered separately because of their distinct cause, related largely to infection with Epstein-Barr virus (EBV). Thyroid cancers are also often distinguished from other HNCs because they are associated with separate risk factors and different causal pathways.
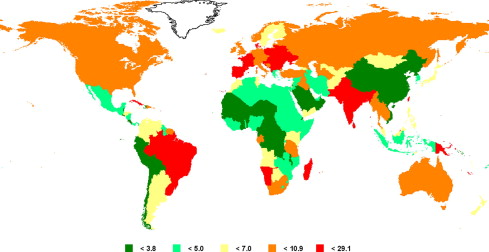
The incidence of oral cavity, larynx, and pharynx cancer varies widely by geographic region and gender ( Fig. 1 ).
- •
HNC, ∼90% of which are squamous cell carcinomas (HNSCC), has a 2-fold to 9-fold higher incidence among men than women.
- •
The age-standardized incidence of HNC is increased in South-Central Asia (14.1 per 100,000) and in Melanesia (a region in the western Pacific Ocean, 22.1 per 100,000), because of high rates of tobacco use in these areas.
- •
HNC incidence rates in the United States (9.9 per 100,000) and Europe (10.8 per 100,000) are lower than that observed in South-Central Asia and Melanesia, but remain notable.
- •
Compared with the United States, HNC incidence is significantly lower in Micronesia (1.8 per 100,000), Middle Africa (3.4 per 100,000), and Eastern Asia (3.5 per 100,000), as well as throughout Western Africa (3.9 per 100,000) and Central America (4.7 per 100,000).
In the United States, an estimated 49,260 new cases of HNC were diagnosed in 2010. Similar to worldwide differences in HNC by gender, the incidence of HNC in the United States is higher in men than women (15.9 vs 6.2 per 100,000). The median age at diagnosis of patients with HNC in the United States is in the seventh decade of life; however, the median age of onset is lower for cancers of the nasopharynx (55 years) and tonsil (57 years).
Temporal Trends in HNC Incidence
Much of the geographic variability in HNC incidence may be explained by differential exposure to the major risk factors for HNC. Tobacco and alcohol exposure remain the most important risk factors for HNC overall, and are responsible for ∼72% (95% confidence interval [CI]: 61%–79%) of HNC in the United States and Europe. As a result of successful tobacco control programs, many industrialized countries have observed a decrease in per-capita cigarette consumption over the past several decades, followed by a decrease in the overall incidence of HNC. In the United States, cigarette consumption peaked in the 1960s; current tobacco use has been declining among both men and women, although use remains more prevalent among men.
Following a decline in tobacco use, the incidence of cancer at many HNC sites has decreased in the United States. For example, between 1974 and 1999, there was a significant decrease in :
- •
Lip cancer (from 2.7 to 1.1 cases per 100,000 people; P <.05)
- •
Oral cavity cancer (from 3.6 to 2.7 per 100,000 people, P <.05)
- •
Hypopharyngeal cancer (from 1.0 to 0.8 cases per 100,000 people; P <.05)
- •
Laryngeal cancer (from 5.4 to 4.5 cases per 100,000 people; P <.05).
In contrast to these decreases, the overall incidence remained stable over the same period for :
- •
Nasopharyngeal: ∼6 per 100,000 cancers
- •
Oropharyngeal: ∼1.5 per 100,000 cancers.
In Europe, the incidence of oral cavity and oropharyngeal cancers has varied greatly by country and gender, with some countries experiencing increases in the age-standardized incidence rates over the last decade :
- •
Males: England, Wales, Czech Republic
- •
Females: France, Netherlands, England, Wales, Denmark.
Other countries have observed decreasing incidences in rates over the last decade :
- •
Males: Northern Ireland, Ireland, France, Finland, Norway, Slovenia, Spain
- •
Females: Malta.
Laryngeal cancer has been decreasing or remained stable in males and females from most European countries, with the exception of Swedish women, among whom it increased from 0.2 to 0.3 per 100,000 between 1994 and 2005.
Changing Oral Cancer Incidence & Mortality in Selected Populations
Beginning in the 1980s, numerous reports from the United States and Europe began to document an increase in the incidence and mortality of tongue malignancies (both oral tongue and base of tongue) primarily among men younger than age 45 years. An increase in tongue carcinoma incidence has now been noted in multiple countries, including Scandinavian, Finnish, and US populations. Furthermore, these increases are consistently shown to be most prominent among young (age 30–50 years) individuals. Among 30-year-old to 39-year-old men in the United States, the rate of mortality from tongue cancer increased 3-fold (0.3 vs 0.9, per 100,000 P<. 001) between 1973 and 1984.
Similarly, between 1973 and 2007, the incidence of oral tongue SCC increased in both male (annual percent change [APC] = +1.6, P<. 05) and female (APC = +4; P<. 05) patients younger than 44 years, although it was stable when not stratified by age and sex (APC = +0.1; P = not significant). The increasing incidence of oral cancers has been observed among multiple countries, always in the younger age groups. These increases are in stark contrast to the decreasing incidence of some other HNC subsites.
Tonsillar carcinoma incidence increasing
In the United States, data from the SEER (Surveillance, Epidemiology, and End Results) program showed that the incidence of tonsillar carcinomas increased significantly between 1973 and 1995 among both white (APC = +2.7) and black (APC = +1.9) men who were younger than age 60 years. The incidence of tonsillar cancer among US women in the same period remained the same or decreased. More recent analyses have reported similar increases. Between 1973 and 2001, the rate of tonsillar cancers increased significantly among 20-year-olds to 44-year-olds in the United States, from 0.18 to 0.25 per 100,000 (APC = +3.9; P <.001), whereas during the same period, the incidence at all other pharyngeal sites (excluding nasopharynx) remained constant or decreased. Comparable increasing trends in oropharyngeal cancer have been observed in other populations, including studies from Canada, Denmark, the United Kingdom, Finland, Sweden, and Slovakia.
Why is there an increasing incidence of oral cancers?
The increased incidence in oral tongue and oropharyngeal carcinoma is observed only for younger patients, with increasing rates noted especially among people born after 1950, although some studies have also suggested that people born between 1910 to 1950 have higher HNC rates than earlier generations. Reasons for this cohort effect are not known. It has been suggested that changes in exposure to environmental carcinogens, such as smokeless tobacco products, might contribute to the increase in tongue cancers ; however, in the United States smokeless tobacco consumption has been declining among both adults and adolescents, so is unlikely to explain this pattern. As discussed later, recent evidence suggests that an increasing proportion of these oropharyngeal cancers are caused by HPV. Changes in sexual behavior, leading to increased oral HPV infection, likely contribute to the increased incidence of oropharyngeal cancer.
Epidemiology of HNC
Overview of HNC Epidemiology
There are more than 600,000 incident cases of HNC worldwide each year, including ∼263,020 oral cavity, 213,179 thyroid gland, 150,677 larynx, 136,622 pharynx, and 84,441 nasopharynx cases per year. Nasopharyngeal cancers are often considered separately because of their distinct cause, related largely to infection with Epstein-Barr virus (EBV). Thyroid cancers are also often distinguished from other HNCs because they are associated with separate risk factors and different causal pathways.
The incidence of oral cavity, larynx, and pharynx cancer varies widely by geographic region and gender ( Fig. 1 ).
- •
HNC, ∼90% of which are squamous cell carcinomas (HNSCC), has a 2-fold to 9-fold higher incidence among men than women.
- •
The age-standardized incidence of HNC is increased in South-Central Asia (14.1 per 100,000) and in Melanesia (a region in the western Pacific Ocean, 22.1 per 100,000), because of high rates of tobacco use in these areas.
- •
HNC incidence rates in the United States (9.9 per 100,000) and Europe (10.8 per 100,000) are lower than that observed in South-Central Asia and Melanesia, but remain notable.
- •
Compared with the United States, HNC incidence is significantly lower in Micronesia (1.8 per 100,000), Middle Africa (3.4 per 100,000), and Eastern Asia (3.5 per 100,000), as well as throughout Western Africa (3.9 per 100,000) and Central America (4.7 per 100,000).
In the United States, an estimated 49,260 new cases of HNC were diagnosed in 2010. Similar to worldwide differences in HNC by gender, the incidence of HNC in the United States is higher in men than women (15.9 vs 6.2 per 100,000). The median age at diagnosis of patients with HNC in the United States is in the seventh decade of life; however, the median age of onset is lower for cancers of the nasopharynx (55 years) and tonsil (57 years).
Temporal Trends in HNC Incidence
Much of the geographic variability in HNC incidence may be explained by differential exposure to the major risk factors for HNC. Tobacco and alcohol exposure remain the most important risk factors for HNC overall, and are responsible for ∼72% (95% confidence interval [CI]: 61%–79%) of HNC in the United States and Europe. As a result of successful tobacco control programs, many industrialized countries have observed a decrease in per-capita cigarette consumption over the past several decades, followed by a decrease in the overall incidence of HNC. In the United States, cigarette consumption peaked in the 1960s; current tobacco use has been declining among both men and women, although use remains more prevalent among men.
Following a decline in tobacco use, the incidence of cancer at many HNC sites has decreased in the United States. For example, between 1974 and 1999, there was a significant decrease in :
- •
Lip cancer (from 2.7 to 1.1 cases per 100,000 people; P <.05)
- •
Oral cavity cancer (from 3.6 to 2.7 per 100,000 people, P <.05)
- •
Hypopharyngeal cancer (from 1.0 to 0.8 cases per 100,000 people; P <.05)
- •
Laryngeal cancer (from 5.4 to 4.5 cases per 100,000 people; P <.05).
In contrast to these decreases, the overall incidence remained stable over the same period for :
- •
Nasopharyngeal: ∼6 per 100,000 cancers
- •
Oropharyngeal: ∼1.5 per 100,000 cancers.
In Europe, the incidence of oral cavity and oropharyngeal cancers has varied greatly by country and gender, with some countries experiencing increases in the age-standardized incidence rates over the last decade :
- •
Males: England, Wales, Czech Republic
- •
Females: France, Netherlands, England, Wales, Denmark.
Other countries have observed decreasing incidences in rates over the last decade :
- •
Males: Northern Ireland, Ireland, France, Finland, Norway, Slovenia, Spain
- •
Females: Malta.
Laryngeal cancer has been decreasing or remained stable in males and females from most European countries, with the exception of Swedish women, among whom it increased from 0.2 to 0.3 per 100,000 between 1994 and 2005.
Changing Oral Cancer Incidence & Mortality in Selected Populations
Beginning in the 1980s, numerous reports from the United States and Europe began to document an increase in the incidence and mortality of tongue malignancies (both oral tongue and base of tongue) primarily among men younger than age 45 years. An increase in tongue carcinoma incidence has now been noted in multiple countries, including Scandinavian, Finnish, and US populations. Furthermore, these increases are consistently shown to be most prominent among young (age 30–50 years) individuals. Among 30-year-old to 39-year-old men in the United States, the rate of mortality from tongue cancer increased 3-fold (0.3 vs 0.9, per 100,000 P<. 001) between 1973 and 1984.
Similarly, between 1973 and 2007, the incidence of oral tongue SCC increased in both male (annual percent change [APC] = +1.6, P<. 05) and female (APC = +4; P<. 05) patients younger than 44 years, although it was stable when not stratified by age and sex (APC = +0.1; P = not significant). The increasing incidence of oral cancers has been observed among multiple countries, always in the younger age groups. These increases are in stark contrast to the decreasing incidence of some other HNC subsites.
Tonsillar carcinoma incidence increasing
In the United States, data from the SEER (Surveillance, Epidemiology, and End Results) program showed that the incidence of tonsillar carcinomas increased significantly between 1973 and 1995 among both white (APC = +2.7) and black (APC = +1.9) men who were younger than age 60 years. The incidence of tonsillar cancer among US women in the same period remained the same or decreased. More recent analyses have reported similar increases. Between 1973 and 2001, the rate of tonsillar cancers increased significantly among 20-year-olds to 44-year-olds in the United States, from 0.18 to 0.25 per 100,000 (APC = +3.9; P <.001), whereas during the same period, the incidence at all other pharyngeal sites (excluding nasopharynx) remained constant or decreased. Comparable increasing trends in oropharyngeal cancer have been observed in other populations, including studies from Canada, Denmark, the United Kingdom, Finland, Sweden, and Slovakia.
Why is there an increasing incidence of oral cancers?
The increased incidence in oral tongue and oropharyngeal carcinoma is observed only for younger patients, with increasing rates noted especially among people born after 1950, although some studies have also suggested that people born between 1910 to 1950 have higher HNC rates than earlier generations. Reasons for this cohort effect are not known. It has been suggested that changes in exposure to environmental carcinogens, such as smokeless tobacco products, might contribute to the increase in tongue cancers ; however, in the United States smokeless tobacco consumption has been declining among both adults and adolescents, so is unlikely to explain this pattern. As discussed later, recent evidence suggests that an increasing proportion of these oropharyngeal cancers are caused by HPV. Changes in sexual behavior, leading to increased oral HPV infection, likely contribute to the increased incidence of oropharyngeal cancer.
Role of HPV in HNSCC
Evidence that HPV Causes a Subset of Oropharyngeal Cancers
Several different oncogenic HPV types have been identified in case series of HNSCC tumors ; however, greater than 90% of these HPV-HNSCC are associated with a single HPV type, HPV-16. Estimates of the proportion of HNSCC that are caused by HPV have varied widely, in part because of differences in case subsite composition, calendar year, country of study, and differences in tumor HPV detection methods. A systematic review of studies found that 26% of HNSCC have HPV DNA detected using polymerase chain reaction, although this prevalence differs substantially by head and neck subsite.
Over the past decade, it has become clear that the increasing incidence of oropharyngeal cancers in developed nations is being driven by a new cause. There is clear molecular and epidemiologic evidence supporting a causal role for HPV in a subset of HNSCC. HPV is detected in the tumor cell nuclei, where it is transcriptionally active, clonal, and not found in the surrounding benign tissue. In addition, case-control studies have shown that cases are more likely than matched controls to have current HPV DNA detected in their exfoliated oral cells, to have a higher number of lifetime oral sex partners (a surrogate for oral HPV exposure), and to have antibodies for HPV oncogenes.
Studies have consistently shown that most HNSCC with HPV detected in tumor are from the oropharynx. The virus has an affinity for the lymphoepithelium of the Waldeyer ring, and in studies of HNSCC patients has been detected most frequently in oropharyngeal cancers. Most oropharyngeal cancers in the United States and Europe are now caused by HPV infection, although there is wide variation in the proportions reported by different US (36%–73%) and European (14%–93%) studies.
The proportion of oropharyngeal cancers caused by HPV seems to have increased over the past 30 years, suggesting HPV is driving the increasing incidence of oropharyngeal cancer recently observed. A large Swedish study reported the prevalence of HPV detected in tonsil cancer increased from 23% in the 1970s, to 68% in 2000 ( P <.001). Additional increases of oropharyngeal cancers in Sweden being associated with HPV have been observed in the past 10 years :
- •
68%: 2000 to 2002
- •
77%: 2003 to 2005
- •
93%: 2006 to 2007.
Similar trends have been reported in several other studies, including a study of US SEER tissues which showed that only 16% of US oropharyngeal cases had HPV detected in 1984 to 1989 compared with 73% during 2000 to 2004, a 4-fold increase in only 2 decades. This study further suggested that the annual number of HPV-related oropharyngeal cancers in the United States is projected to surpass the number of incident invasive cervical cancer cases in the United States by 2020.
Does HPV Cause Cancer at Nonoropharyngeal HNC Sites?
A causal role for HPV among oropharyngeal cancers is now established, but it is less clear whether HPV may cause HNSCC at other sites. Case-control studies evaluating the association of HPV DNA in oral exfoliated cells and odds of oral cavity or other nonoropharyngeal HNSCCs have most commonly been null or small in magnitude, unlike the strong associations observed for oropharyngeal cancers. However, a role for HPV in a small subset of these cancers cannot be excluded because the etiologic heterogeneity of these nonoropharyngeal HNSCC sites would be more difficult to observe and some studies have suggested an association. Initial studies have reported HPV detection in a subset of oral cavity, laryngeal, and nasopharyngeal cancers, but the consistency and strength of evidence implicating HPV at these sites are notably less than in the oropharynx.
HPV in laryngeal cancers
HPV DNA has been detected in 0% to 31% of laryngeal cancers in recent US studies, whereas studies from populations in Europe, Asia, and elsewhere have reported higher prevalence estimates. In addition to the data provided by these case series, a temporal relationship between HPV and the development of laryngeal cancer was suggested by 1 nested study of 76 laryngeal cases and 411 controls; this study showed that after adjusting for cotinine (a marker of nicotine exposure), individuals with serum HPV-16 antibodies were 2.4 times more likely than HPV-16– seronegative individuals to develop laryngeal cancer within 9 years from date of blood collection in the study. Furthermore, a systematic review of the literature found that patients with laryngeal cancers were more likely than matched controls to have had exposure to HPV (odds ratio [OR] = 2.0; 95% CI 1.0, 4.2). However, many of the individual studies had null results and they differed in their definition of exposure, for example :
- •
Presence of HPV DNA in biopsy specimens
- •
Presence of HPV DNA in oral exfoliated cells
- •
Presence of serum antibodies against high-risk HPV.
Altogether, these studies suggest that HPV may be associated with laryngeal cancer, but it currently seems unlikely to cause a large proportion of cases in the general population. However, a special population of patients with recurrent respiratory papillomatosis (RRP) may be more susceptible to HPV-related oncogenesis in the larynx and other portions of the respiratory tract. RRP is typically associated with HPV types 6 and 11, which are considered to be low-risk types in the anogenital tract. However, data from clinical cases have documented instances in which low-risk HPV (typically HPV-11)-related RRP can undergo malignant transformation. Nonetheless, even in this population, malignant transformation seems to be an uncommon outcome, with 3% to 5% of patients with adult-onset RRP and less than 1% of patients with juvenile-onset RRP developing carcinomas.
HPV in oral cavity cancers
HPV DNA has been detected in ∼25% of oral cavity cancers, although the results of individual studies have varied greatly ( Fig. 2 ). It is likely that these are overestimates, because some HPV-related oral cavity cancers show clear oropharyngeal involvement and some of these oral cavity cancers are extensions from base-of-tongue primaries ; thus the proportion of oral cavity cancers that are HPV-related is currently unknown. Several case-control studies have evaluated the association of HPV antibodies, biopsy specimens, or HPV DNA in oral epithelial cells. The results of these studies have been varied, with some reporting a significant association between HPV and increased odds of oral cavity cancer, whereas others studies found no significant association. Therefore, it remains unclear whether HPV is a cause of a subset of oral cavity carcinomas.
For continuity with above formatting, we suggest you insert a subheading here with the following title “HPV in nasopharyngeal carcinomas.” Recent studies have also begun to explore a potential role of HPV in nasopharyngeal carcinomas (NPCs). NPCs have classically been associated with EBV, but HPV has also been detected in a subset (5%–83%) of NPC. However, the few studies that have investigated HPV infections in normal nasopharyngeal epithelium have reported similar HPV estimates in benign nasopharyngeal tissues. A recent study by Maxwell and colleagues found that among 5 patients with NPC from a North American population, 4 harbored detectable HPV DNA and high p16 expression but lacked EBV-encoded RNA. These findings are consistent with a potential role for HPV in a subset of NPC from this population, but do not prove a causal relationship. In another recent investigation, Huang and colleagues performed a case-control study and found no association between HPV and NPC in Taiwan. Therefore, there is insufficient evidence to support a causal association between HPV and NPC. Further studies are necessary to investigate this potentially important association. Nonetheless, given the potential for tonsillar carcinomas to extend into the nasopharynx, misclassification remains a challenge for these studies.
Role of HPV in the Changing Incidence of HNSCC
Given the strong role of HPV in oropharyngeal cancer and the small role of HPV in other HNSCC subsites, several studies have evaluated incidence trends after stratifying head and neck sites into those sites most likely to be HPV-related (subsites of the Waldeyer ring, including soft palate, palatine, and lingual tonsils) and those HNSCC sites where an HPV cause is unlikely (oral cavity, oral tongue). Chaturvedi and colleagues found that between 1973 and 2004, the US incidence of HPV-HNSCC increased significantly (APC = +0.80, P<. 001), especially among younger males (US incidence trends are depicted in Fig. 3 ). In contrast, the incidence of HPV-unrelated HNSCC decreased significantly during this same period (APC = –1.85, P<. 001).
In a similar study from 15 population-based European cancer registries, incidence trends of HPV-related HNC increased significantly between 1988 and 2002 (APC = +3.37, P<. 05). HPV-unrelated HNC incidence in Europe also increased from 1988 until 1998 (APC = +1.73; 95% CI 1.2, 2.3), but seemed to plateau after 1998 (APC = –0.8; 95% CI –3.0, 1.5). Studies using Canadian and Australian cancer registries also have observed increases in oropharyngeal cancer incidence.
Oral HPV infection and natural history
Oral HPV Infection
There are more than 100 different types of HPV, distinguished by variations in their genetic sequence, and more than 15 HPV types that have been associated with human cancers. HPV types are separated into high-risk oncogenic HPV types, including HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, and 73; the remaining types are classified as low-risk or nononcogenic. The carcinogenicity of HPV has been well described in the lower genital tract, where HPV is a necessary, but not sufficient, cause of invasive cervical cancer. Although it is clear that HPV is an important cause of oropharyngeal cancer, infection with HPV is neither a necessary nor a sufficient cause of oropharyngeal cancer (oropharyngeal cancer can occur in the absence of HPV and not all oral HPV infections lead to malignant transformation).
Several cross-sectional and case-control studies have sought to characterize the prevalence of oral HPV infections in the general population. In a recent systematic review of 18 published studies, 4.5% (95% CI 3.9, 5.1) of 4070 healthy individuals had HPV DNA detected in oral exfoliated cells. The oral HPV prevalence was similar in men (4.6%) and women (4.4%). High-risk oral HPV was detected in 3.5% of participants and oral HPV-16 infection was detected in 1.3% of all study individuals, representing approximately 28% of all oral HPV infections that were detected. A recent large multinational study of healthy men reported slightly lower prevalence of :
- •
Any high-risk oral HPV infection (1.3%; 95% CI 0.8%, 2.0%)
- •
HPV-16 (0.6%; 95% CI 0.2%, 1.1%) infection.
Higher oral HPV prevalence has been reported among select groups, such as:
- •
Individuals infected with the human immunodeficiency virus (HIV) (33%)
- •
Current smokers (10%)
- •
People with more than 5 lifetime sexual partners (7.4%).
Natural History of Oral HPV Infection
Although the natural history of anogenital HPV infections and its transmission are well understood, there have been few studies investigating the natural history of oral HPV infection. Initial studies suggest that some oral HPV infections may persist after more than 2 years, although the studies had limited power or did not include analysis by HPV type. D’Souza and colleagues investigated the 6-month natural history of oral HPV infections in a high-risk longitudinal cohort of 136 HIV-positive and 63 at-risk HIV-negative individuals. In this population, prevalent oral HPV infections detected at baseline were as likely as cervical infections to persist to 6 months among HIV-negative and HIV-positive individuals. Factors that were associated with increased oral HPV persistence included :
- •
Current smoking status
- •
Older age
- •
Lower current CD4 cell count
- •
Use of highly active antiretroviral therapy (HAART) therapy
- •
Duration of HAART therapy.
These factors differed from those that predicted cervical HPV persistence at 6 months. For example, tobacco use was found to significantly increase the odds of oral HPV persistence, but not cervical persistence. Although this study population differs from the general population, it suggests that the oral HPV natural history or risk factors for persistence may differ in some ways from cervical HPV infection.
The long-term natural history of oral HPV infection has not been evaluated; however, initial studies suggest that, as with genital HPV infection, many infected people may clear their oral HPV infections quickly. Further studies on oral HPV transmission, median time to clearance, and risk factors for persistence and progression are needed.
Risk factors for HPV-HNSCC
Epidemiologic studies show that there are several notable differences in the demographics of patients who develop HPV-HNSCC compared with HPV-unrelated HNSCC patients ( Table 1 ). Patients who have HPV-related cancers are on average :
- •
Younger
- •
More likely to have a higher socioeconomic status
- •
More likely to have a higher education
- •
More likely to have more lifetime sexual partners
- •
Associated with white race.
| HPV-HNSCC | HPV-Unrelated HNSCC | |
|---|---|---|
| Incidence trend | Increasing | Decreasing/stable |
| Anatomic location | Primarily tonsil and base of tongue | All head and neck sites |
| Median age (y) at diagnosis | 54 | 60 |
| Socioeconomic status | Higher | Lower |
| Primary risk factors | Sexual exposure to oral HPV | Tobacco and alcohol exposure |
| Survival | ||
| 3-y oropharyngeal survival (%) | Better 82 | Worse 57 |
More specifically, the proportion of HNSCCs that are HPV-associated is significantly less in black compared with white patients (4% of black HNSCC vs 34% of white HNSCC in a recent study).
Patients with HPV-HNSCC are:
- •
More likely to have an oropharyngeal primary tumor, to be diagnosed at a late stage, and to have better survival than those with HPV-unrelated HNSCC.
- •
Less likely to have a history of extensive tobacco and alcohol use.
However, despite these differences, most patients with HPV-HNSCC do have some tobacco or alcohol use; nonsmoker nondrinkers constitute less than 20% of patients with HPV-HNSCC. HPV-HNSCC incidence rates are ∼3-fold higher in men compared with women, similar to the 3-fold higher incidence of HPV-unrelated HNSCC in men compared with women. Although increased male tobacco and alcohol use likely explains the higher incidence of HPV-unrelated HNSCC in men, reasons for the higher incidence of HPV-HNSCC in men are less clear.
Given the different cause of HPV-related versus HPV-unrelated HNSCC, it is not surprising that the risk factors for these cancers are different as well. Increased sexual behavior (a surrogate for oral HPV exposure) has consistently been associated with increased odds of developing an HPV-HNSCC cancer. Because sexual behaviors are colinear (people who have a higher number of partners for 1 sexual act tend to have a higher number of partners for other sexual acts as well), the associations with increased odds of HPV-HNSCC have been observed for various measures of sexual behavior, including:
- •
Earlier age of sexual debut
- •
Higher number of lifetime vaginal sex partners
- •
Higher number of lifetime oral sex partners.
Given the colinearity of these behaviors, it is difficult to differentiate which sexual behaviors are associated with oral HPV transmission from these data. The strong association of sexual behavior with increased odds of HPV-HNSCC is not observed for HPV-unrelated HNSCC, which are primarily caused by alcohol and tobacco use.
As HPV-HNSCC has become more common, the demographic profile of patients with HNSCC has begun to change from the traditionally older man who consumes tobacco and alcohol. Given the differences in patients with HPV-related and HPV-unrelated HNSCC, it might be tempting to assume that a younger, nonsmoking HNSCC patient is HPV-related or conversely that an older patient with a history of heavy tobacco use might be HPV-unrelated. However, a study exploring the predictive usefulness of age, race, tobacco use, and sexual history showed that these factors have only a moderate predictive value for true tumor HPV status. These factors had moderate predictive value among patients with oropharyngeal cancer (positive predictive value [PPV] = 55%, negative predictive value [NPV] = 68%) as well as when used among all patients with HNSCC (PPV = 75%, NPV = 65%). Therefore, despite substantial differences in population characteristics, clinical HPV tumor testing is critical for determining whether the cause of the disease is related to HPV.
Current controversies and nuances to HNSCC epidemiology
There are several nuances and underappreciated aspects to the epidemiology of HPV-HNSCC.
Mischaracterization of Patients with HPV-HNSCC
Patients with HPV-HNSCC are sometimes mischaracterized by the press as highly sexual or promiscuous. Although the average number of sexual partners is larger among those with HPV-related versus HPV-unrelated HNSCC, the histories of individual patients vary greatly, and it is common for patients with HPV-related tumors to report a low number (<6) of lifetime sexual partners. It is similarly important to note that only some patients with HPV-related tumors are nonsmokers/nondrinkers. Given evidence suggesting that smoking predicts higher risk of disease recurrence and distant metastasis in HPV-HNSCC, counseling for smoking cessation should remain a priority for clinicians.
Race
Racial disparities in HNSCC incidence and survival remain striking. Because HPV-HNSCCs have been shown to have improved survival compared with HPV-unrelated carcinomas, and a lower proportion of black patients diagnosed with HNSCC are HPV-related, racial differences in HNSCC survival may be in part or entirely explained by this difference in cause. Although initial studies support this possibility, suggesting survival of black and white patients with HPV-unrelated HNSCC is similar, further investigation of these disparities is needed to understand whether there are differences in oral HPV acquisition or clearance.
Tumor Biology and Classification
There is some limited evidence to suggest that HPV may be associated with a small subset of HNSCC outside the oropharynx, although the results of these studies are far from clear. Furthermore, although HPV tumor status is clearly associated with improved survival among patients with oropharyngeal carcinomas, consensus around optimal biomarker profiles for HNSCC survival has not been established. Even more unclear is how to define patients with tumors who are HPV-negative but p16-positive. Because p16 overexpression is used by some institutions as a surrogate marker for HPV infection, are these tumors HPV-related despite the lack of detection of HPV DNA with the current assays? Further understanding of the biology of these tumors and how to classify them needs to be addressed.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


