Purpose
To investigate binocular interaction of visual acuity (VA) in patients with intermittent exotropia and its relationship with accommodative responses during binocular vision.
Design
Prospective pilot study.
Methods
setting: Institutional. patient: Sixty-three patients with intermittent exotropia between 8 and 15 years of age. observation: Binocular VA and monocular VA were measured in sequence. Accommodative responses of both eyes were measured using the WAM-5500 autorefractor/keratometer (GrandSeiko) during binocular and monocular viewing conditions at 6 m. Accommodative responses during binocular vision were calculated using the difference between the refractive errors of binocular and monocular vision. main outcome measures: Binocular interactions of VA were categorized as binocular summation, equivalency, or inhibition. The prevalence of the 3 patterns of binocular interaction was investigated. Accommodative responses were correlated with differences between binocular VA and better monocular VA.
Results
Most patients (38 patients; 60.3%) showed binocular equivalency. Binocular summation and inhibition were noted in 19 (30.2%) and 6 (9.5%) patients, respectively. Linear regression analysis revealed a significant correlation between binocular interaction and accommodative responses during binocular vision ( P < .001). Accommodative responses significantly correlated with the size of exodeviation at distance (P = .010).
Conclusions
In patients with intermittent exotropia, binocular interaction is associated with accommodative response during binocular vision and the size of exodeviation, suggesting that accommodative convergence is a mechanism that maintains ocular alignment. Therefore, binocular interaction, especially binocular inhibition, can be a good indicator of diminishing fusional control in intermittent exotropia.
Binocular visual acuity (VA) has been used rarely in clinical practice, although binocular VA better represents the state in which a person usually functions. Binocular vision can differ from monocular vision in terms of VA, contrast sensitivity, and peripheral visual field. A few epidemiologic studies investigating binocular vision have revealed that binocular interactions, such as summation and inhibition, occur in a small proportion of normal healthy people.
One previous study revealed that binocular inhibition is noted much more frequently in patients with intermittent exotropia than in the normal population (41.7% compared with 2%). Accommodative convergence may be used to maintain ocular alignment as fusional convergence becomes insufficient in patients with intermittent exotropia. Such increased accommodation efforts may result in decreased distance binocular VA, which was noted in 41.7% of patients with intermittent exotropia. However, the relationship between accommodative convergence and binocular inhibition has not been proven by directly measuring accommodative responses in patients with intermittent exotropia.
In this study, we aimed to evaluate binocular VA in patients with intermittent exotropia. In addition, accommodative response and its relationship with binocular VA in patients with intermittent exotropia were assessed by objective measurement of accommodation using the WAM-5500 autorefractor/keratometer (GrandSeiko, Fukuyama, Japan).
Methods
This prospective study included consecutive patients between 8 and 15 years of age with intermittent exotropia at distance or near between July 2010 and July 2011. The minimum age for participation was limited to 8 years to obtain accurate measurements of accommodation and ocular deviation by ensuring fixation, capability of discriminating the superiority of binocular VA from monocular VA, and ability to understand and answer the questionnaire items on psychosocial symptoms and functions associated with strabismus. Patients were excluded if they declined to participate in the study or had any history of neurologic or systemic disorders that can affect vision. Patients with BCVA worse than 20/20 in both eyes, a previous history of strabismus surgery or ocular disease other than strabismus, amblyopia (≥ 2 lines corrected VA difference), anisometropia of more than 2 diopters, vertical deviation of more than 5 prism diopters, and occlusion therapy within 6 months, A- or V-pattern strabismus, dissociated vertical deviation, or paralytic or restrictive exotropia were also excluded.
Ophthalmologic Examination
All patients underwent a complete ophthalmologic examination performed by 1 pediatric ophthalmologist (J.-M.H.). The alternate cover test with prisms was performed in all patients to measure the angle of exodeviation. The Distance Randot stereotest (Stereo Optical Co Inc, Chicago, Illinois, USA) was performed to evaluate stereoacuity by trained examiners. A stereoacuity of 100 arc seconds or better was considered good. Refractive errors were measured by cycloplegic refraction with 1% cyclopentolate hydrochloride.
Binocular Interaction of Visual Acuity
A trained examiner recorded distance visual acuities with the Snellen chart at 6 m. Binocular VA was recorded initially to avoid disruption of fusion, and monocular VAs of both eyes were checked after occluding the other eye in random sequence. Patients were requested to read randomly chosen letters on the Snellen chart to exclude any learning effect attributed to previous examinations. For patients who did not wear glasses, binocular VA and monocular VA were assessed without correction if both monocular VAs were 20/25 or better and refractive errors were between +1.50 and −0.75 diopters. Otherwise, binocular VA and monocular VA were assessed with corrective lenses. The logarithm of the minimal angle of resolution (logMAR) difference between binocular VA and the better monocular VA was calculated, and patients’ binocular interactions were classified as follows : summation (logMAR binocular VA minus logMAR better monocular VA ≤ −0.10), equivalency (−0.10 < difference < 0.10), or inhibition.
Accommodative Response
Accommodative responses of both eyes were measured using the WAM-5500 binocular autorefractor/keratometer while the patient was wearing distance correction glasses ( [CR] ). This device adopts an open-view window, so patients can see a distant object through the window in binocular status. Because the measurement of refractive error does not obstruct the vision in any eye, patients can maintain binocularity during the measurement. Binocular viewing was assessed first to avoid disruption of fusion, and assessment was performed using the same examination as for distance VA. Trained examiners confirmed maintenance of ocular alignment during measurements. Afterward, the left and right eyes were examined randomly by occluding the opposite eye. The spherical equivalent of the refractive errors during binocular vision was subtracted from the values obtained during monocular vision in the better eye, yielding an accommodative response during binocular vision.
Visual Function and Quality-of-Life Questionnaire
The Adult Strabismus Questionnaire (AS-20) was used to evaluate the discomfort caused by strabismus and its impact on the patient’s quality of life. The overall AS-20 score is calculated as an average of all 20 item scores. Patients or their parents also were asked if the frequency or extent of exotropia recently had increased. The correlation between the accommodative response and visual discomfort was evaluated by linear regression between the overall AS-20 score and accommodative response during binocular vision.
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 18.0 (SPSS, Inc, Chicago, Illinois, USA). The Kruskal-Wallis test was performed to compare baseline characteristics among the 3 groups separated on the basis of binocular interaction. Linear regression analysis was performed to assess the relationship between binocular interaction (the difference between binocular VA and better monocular VA) and (1) accommodative responses during binocular vision and (2) questionnaire scores. P values of less than .05 were considered statistically significant.
Results
A total of 63 patients 8 to 15 years of age (mean ± standard deviation, 10.7 ± 2.0 years) were included. Table 1 presents the clinical characteristics in patient groups separated on the basis of binocular interaction.
| Total (n = 63) | Binocular Interaction | ||||
|---|---|---|---|---|---|
| Summation (n = 19) | Inhibition (n = 6) | Equivalency (n = 38) | P Value | ||
| Mean age ± SD (range), year | 10.7 ± 2.0 (8 to 15) | 10.5 ± 1.6 (9 to 15) | 11.7 ± 2.7 (9 to 15) | 10.7 ± 2.0 (8 to 15) | .706 |
| Male gender, no. (%) | 36 (57.1) | 11 (58) | 5 (83) | 20 (53) | .412 |
| Mean exodeviation at distance ± SD (range), PD | 19.3 ± 9.2 (2 to 50) | 15.6 ± 7.7 (2 to 30) | 29.3 ± 13.4 (16 to 50) | 19.6 ± 8.1 (4 to 35) | .040 |
| Mean exodeviation at near ± SD (range), PD | 17.3 ± 9.8 (0 to 35) | 15.4 ± 9.2 (2 to 35) | 20.0 ± 13.1 (2 to 35) | 17.8 ± 9.7 (0 to 35) | .504 |
| Good distance stereoacuity, no. (%) | 12 (19) | 5 (26) | 0 | 7 (18) | .389 |
| Refractive errors in better eye (range), diopters | −1.57 ± 2.3 (−6.0 to 5.0) | −1.76 ± 3.3 (−6.0 to 5.0) | −1.56 ± 1.6 (−3.75 to −0.13) | −1.47 ± 1.7 (−5.5 to 2.75) | .896 |
| Patients with myopia, no. (%) | 51 (81) | 14 (74) | 6 (100) | 31 (82) | .389 |
| Recent aggravation in exodeviation a | 9 (14) | 2 (11) | 3 (50) | 4 (11) | .071 |
a Recent aggravation in exodeviation was assessed based on patients’ or their parents’ descriptions of recent increases in frequency or degree of exodeviation.
Binocular Interaction of Visual Acuity
Most patients (38 patients; 60.3%) showed binocular equivalency. Binocular summation was noted in 19 (30.2%) of 63 patients, whereas binocular inhibition was noted in 6 (9.5%) of 63 patients. There was no significant difference in patient characteristics, refractive errors, or percentage of patients showing good stereoacuity among patients with binocular summation, inhibition, and equivalency. However, the mean angle of exodeviation at distance was significantly different among the 3 groups, and the deviation was largest in patients with binocular inhibition (29.3 ± 13.4 compared with 15.6 ± 7.7 in the summation group and 19.6 ± 8.1 in the equivalency group). A recent increase in frequency or degree of exodeviation was noted more frequently in patients with binocular inhibition (50%), which was marginally significant among the 3 groups ( P = .071). The correlation between binocular VA and better monocular VA was significant in patients with intermittent exotropia (coefficient of regression, r = 0.369; P = .003).
Relationship Between Binocular Visual Acuity Minus Monocular Visual Acuity Difference and Accommodation
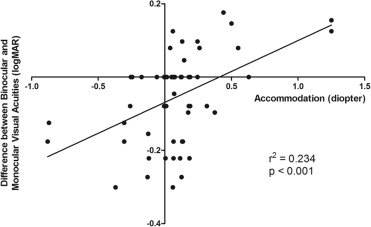
The difference between binocular VA and better monocular VA correlated significantly with accommodative response during binocular vision ( r = 0.484; P < .001; Figure 1 ). The positive r value indicates that the difference between binocular VA and monocular VA (logMAR) increases as accommodation increases, suggesting that binocular VA worsens as the accommodative response increases during binocular vision.
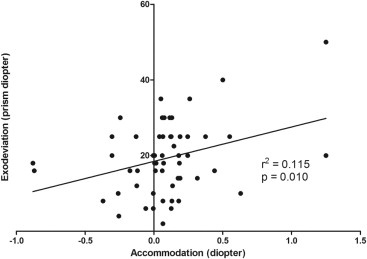
Relationship Between Accommodation and the Size of Exodeviation
As the angle of exodeviation at distance increases in patients with intermittent exotropia, the accommodative response increases. This is evident in the positive value of the coefficient of linear regression between the two ( r = 0.339; P = .010; Figure 2 ).
Relationship Between Binocular Interaction and Distance Stereoacuity
Table 1 presents the frequency of patients with good stereoacuity according to binocular interaction. All patients with binocular inhibition had poor distance stereoacuity. One of 6 (16.7%) patients with binocular inhibition had 400 arc seconds of stereoacuity, and the others had nil stereoacuity. The presence of good distance stereoacuity was higher in patients with binocular summation or equivalency, but this was not statistically significant ( P = .389, 2 × 3 Fisher’s exact test).
Relationship Between Quality-of-Life Questionnaire and Binocular Visual Acuity Minus Monocular Visual Acuity Difference or Accommodation
Linear regression analysis was performed to evaluate the correlation between overall AS-20 score and binocular VA − monocular VA difference; the correlation coefficient was −0.208, which did not reach statistical significance ( P = .160). The same analysis was performed to evaluate the relationship between quality of life and accommodation, but it failed to reveal any significant relationship ( P = .194).
Relationship Between Age and Binocular Interaction
Table 2 demonstrates the comparison of binocular interaction and accommodative response between 2 different age groups (8 to 10 years vs 11 to 15 years). In the younger age group, the percentage of patients showing binocular summation was higher than that in the older age group (32.3% vs 27.6%), whereas that showing binocular inhibition was lower than that in the older age group (5.9% vs 13.8%). The difference, however, was not statistically significant ( P = .596). Differences between binocular and better monocular VA and accommodative response during binocular vision were not significantly different between the 2 age groups ( P = .694 and P = .654, respectively).



