Currently, the main application of endoscopic surgery relies on the middle ear cholesteatoma surgical treatment. However, in the natural evolution of the technique there are the steps toward of lateral skull base surgery and treatment of pathologic conditions of pertous bone. The endoscopic approaches to lateral skull base are (1) a transcanal exclusively endoscopic approach or (2) combined approaches (microscopic endoscope-assisted), including transotic, infralabyrinthine, and suprameatal translabyrinthine.
Key points
- •
The endoscopic approach to lateral skull base can be classified as a transcanal exclusively endoscopic approach or as combined approaches (microscopic endoscope-assisted): transotic, infralabyrinthine, and suprameatal translabyrinthine.
- •
The transcanal exclusive endoscopic approach allows eradication of pathologic conditions involving the petrous apex, internal ear canal fundus, with extension limited to the intracochlear, intravestibular, and pericartoid regions. If the pathologic state involves the mastoid, an exclusive approach is not feasible.
- •
The transotic endoscope-assisted approach allows the removal of big lesions, which completely involve the petrous bone, with hearing loss compromised (ie, cholesterol granulomas). In particular, endoscope introduction is indicated for the control of the paraclival region and for the control of the carotid artery at the level of the clivus and the petrous apex.
- •
The infralabyrinthine endoscope-assisted approach is indicated for lesions extending inferiorly to the labyrinth. This approach allows removal of pathologic matter without loss of hearing.
- •
The suprameatal translabirinthine endoscope-assisted approach is indicated for pathologic conditions (mainly cholesteatomas) involving the labyrinthine tract of the facial nerve with or without internal auditory canal extension facial nerve tract with or without internal auditory canal extension.
Introduction
Endoscopic instrumentation, techniques, and knowledge have improved during the last few years and the authors believe that, in the future, endoscopic surgical techniques will gain increasing importance in otologic surgery. The authors’ experience in endoscopic ear surgery leads to the belief that most of the spaces considered to be difficult to access with the microscopic technique could be easily visualized by endoscope-assisted surgery or by exclusively endoscopic approaches. Moreover, the authors think that new anatomic, physiologic, and surgical concepts should be introduced for this purpose.
A gradual introduction of endoscopic techniques to treatment of pathologic conditions of the middle ear began in the 1990s. Endoscopies were primarily used for the visualization of hidden areas such as the posterior epitympanum during classic microscopic tympanoplasty. Gradually, endoscopies were used also in an operative fashion, to substitute for the microscope as a main tool during middle ear operations. At present, the main application of endoscopic surgery is in middle ear cholesteatoma surgery but, in the natural evolution of the technique, there are the steps forward of lateral skull base surgery. In recent years, the authors began to notice that the internal ear and the whole temporal bone could be accessed in an endoscopic-assisted fashion or by an exclusive endoscopic approach. The only problem would be codifying, as much as possible, the landmarks and the procedures, and integrating them to classic microscopic approaches. At present some experiences of endoscopic ear surgery of the lateral skull base have already been made, both on cadaver dissection and in living patients. The codification of the initial exclusively endoscopic approaches was based on cadavers. The first steps of the procedures were attempted for cholesteatoma treatment or for exploration and study of middle ear. The codification of the endoscopic approaches in combination with microscopic approaches come, on the other hand, from clinical experiences in which endoscopes were used as an aid for microscopic-based approaches to internal ear or petrous treatment of pathologic conditions of bone.
Summarizing these concepts, the approaches can be classified as follows:
- A.
Transcanal exclusively endoscopic approach
- B.
Combined approaches: microscopic endoscope-assisted
- •
Intralabyrinthine ( Fig. 1 A)
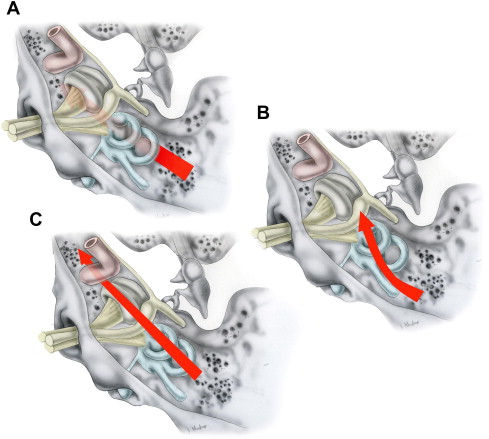
Fig. 1
( Left ear ) The combined approaches to the inner ear. Arrows indicate direction of procedures. ( A ) Infralabyrinthine. ( B ) Suprameatal translabyrinthine. ( C ) Transotic.
- •
Suprameatal translabyrinthine (see Fig. 1 B)
- •
Transotic (see Fig. 1 C).
- •
The aim of this article is to analyze the morphology and surgical and anatomic findings of the approach to lateral skull base surgery, petrous apex, internal ear, and internal auditory canal by using exclusive or combined endoscopic techniques.
Introduction
Endoscopic instrumentation, techniques, and knowledge have improved during the last few years and the authors believe that, in the future, endoscopic surgical techniques will gain increasing importance in otologic surgery. The authors’ experience in endoscopic ear surgery leads to the belief that most of the spaces considered to be difficult to access with the microscopic technique could be easily visualized by endoscope-assisted surgery or by exclusively endoscopic approaches. Moreover, the authors think that new anatomic, physiologic, and surgical concepts should be introduced for this purpose.
A gradual introduction of endoscopic techniques to treatment of pathologic conditions of the middle ear began in the 1990s. Endoscopies were primarily used for the visualization of hidden areas such as the posterior epitympanum during classic microscopic tympanoplasty. Gradually, endoscopies were used also in an operative fashion, to substitute for the microscope as a main tool during middle ear operations. At present, the main application of endoscopic surgery is in middle ear cholesteatoma surgery but, in the natural evolution of the technique, there are the steps forward of lateral skull base surgery. In recent years, the authors began to notice that the internal ear and the whole temporal bone could be accessed in an endoscopic-assisted fashion or by an exclusive endoscopic approach. The only problem would be codifying, as much as possible, the landmarks and the procedures, and integrating them to classic microscopic approaches. At present some experiences of endoscopic ear surgery of the lateral skull base have already been made, both on cadaver dissection and in living patients. The codification of the initial exclusively endoscopic approaches was based on cadavers. The first steps of the procedures were attempted for cholesteatoma treatment or for exploration and study of middle ear. The codification of the endoscopic approaches in combination with microscopic approaches come, on the other hand, from clinical experiences in which endoscopes were used as an aid for microscopic-based approaches to internal ear or petrous treatment of pathologic conditions of bone.
Summarizing these concepts, the approaches can be classified as follows:
- A.
Transcanal exclusively endoscopic approach
- B.
Combined approaches: microscopic endoscope-assisted
- •
Intralabyrinthine ( Fig. 1 A)
Fig. 1
( Left ear ) The combined approaches to the inner ear. Arrows indicate direction of procedures. ( A ) Infralabyrinthine. ( B ) Suprameatal translabyrinthine. ( C ) Transotic.
- •
Suprameatal translabyrinthine (see Fig. 1 B)
- •
Transotic (see Fig. 1 C).
- •
The aim of this article is to analyze the morphology and surgical and anatomic findings of the approach to lateral skull base surgery, petrous apex, internal ear, and internal auditory canal by using exclusive or combined endoscopic techniques.
Transcanal exclusive endoscopic approach
This endoscopic approach allows eradication of pathologic matter involving petrous apex, internal ear canal fundus, with extension limited to the intracochlear, intravestibular, and pericartoid regions. If the pathologic condition involves the mastoid, an exclusive approach is not feasible.
Possible indications are
- •
Mesotympanic cholesteatomas with medial extension toward inner ear structures
- •
Cholesterol granulomas of the petrous apex
- •
Small symptomatic or growing acoustic neuromas with exclusive extension to internal ear canal fundus
- •
Cochlear schwannomas with or without internal ear canal fundus extension
- •
Facial nerve schwannomas involving timpani tract and geniculate ganglion.
Clinical application of this approach is currently limited, although preliminary experiences and results following initial attempts are promising. Even indications for surgery in some of the pathologic conditions treated by these approaches could change in the future as a result of these minimally invasive operations, compared with the extensive bony tissue removal that microscopic techniques require.
Preliminary Surgical Steps
Using a transcanal endoscopic approach, a circumferential incision of the external ear canal skin is made approximately 3 cm from the annulus by a 0° degree endoscope.
Tympanic membrane and external ear canal skin are then removed en bloc to obtain the widest exposition of the middle ear. Using a 0° degree endoscope, a circumferential drilling is made to further increase the view and to facilitate maneuvering of surgical instruments.
Next, it is fundamental to identify the great vessels that have close relationships to the middle ear (ie, the jugular bulb and carotid artery). The first is found at the level of hypotympanum and the second at the level of protympanum, close to the eustachian tube. In some cases, an extensive drilling at those levels are required, in other cases the vessels are clearly identified without drilling any bony tissue.
Next, the incus and the malleus are removed. This allows the surgeon better access to the tympani tract of the facial nerve, to the geniculate ganglion region, and to the greater petrosal nerve, which is located anteriorly.
The tympanic tract of the facial nerve and the greater petrosal nerve are then skeletonized. The cochleariform process should be removed, uncovering the underlying tensor tympani muscle. This step could be performed in a posterior to anterior direction using a microcurette because the bone at this level is very thin. In some cases the muscle need to be cauterized due to the bleeding that these procedures might provoke. When cauterizing, pay attention to the proximity of the geniculate ganglion at this level.
Once the tensor tympani canal has been removed, dissection of the muscle itself is done, displacing it anteriorly. In this way an adequate space is achieved to enable surgery directed to the geniculate ganglion and greater petrosal nerve. The relationship between the superior and lateral border of the tensor tympani canal and the facial nerve (in particular the geniculate ganglion in its posterior and inferior aspect) is apparent.
If the pathologic matter extends anteriorly to the pericartoid region, an increased skeletonization of the greater petrosal nerve should be made in a posterior to anterior direction, by also identifying the dura of the middle cranial fossa, which at this level is situated very close to the geniculate ganglion. The greater petrosal nerve represents a fundamental landmark for this procedure because it has an almost parallel course to the horizontal tract of the carotid artery.
If the lesion has an intracochlear or intravestibular extension with or without extension to the fundus of internal ear canal, the identification of the labyrinthine tract of the facial nerve should be performed. The nerve should be followed from geniculate ganglion to its entry into the internal auditory canal with either a transvestibular or a transcochlear approach.
The choice of the approach will depend on which lesion is being removed and, in particular, will depend on the internal auditory canal involvement and the bone erosion provoked by the pathologic state.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


