(1)
Alo Eye Care, Kolkata, India
Keywords
Benign tumorsSquamous papillomaSeborrheic keratosisKeratoacanthomaSebaceous gland tumorsSweat gland tumorsAdenomaMelanocytic nevusNeurofibroma haemangiomaVarixLymphangiomaCysts5.1 Benign Tumors of Epidermis
5.1.1 Squamous Papilloma
5.1.1.1 Introduction
Squamous papilloma is one of the most common benign eyelid lesions. It is not a specific clinicopathologic entity.
5.1.1.2 Age of Presentation
Squamous papilloma belongs to a group of conditions that usually present in middle or elderly age.
5.1.1.3 Clinical Features
Squamous papilloma may have various presentations, ranging from sessile to pedunculated, solitary or multiple, pigmented or of a color similar to that of the skin. A rough, irregular surface with keratinized crust formation is a common finding.
5.1.1.4 Prognosis
The growth pattern is very slow; if the lesions are growing rapidly, other conditions should be suspected.
5.1.1.5 Treatment Options
Shave excision is the best option. Other options include ablative carbon dioxide or argon laser application to the base of the tumor.
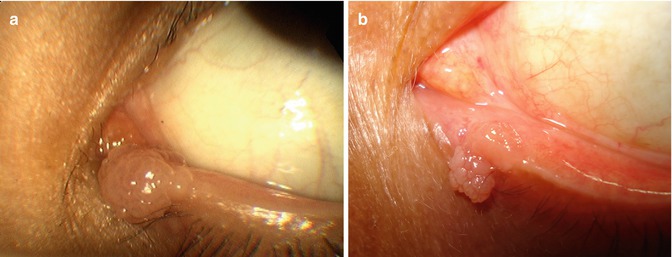

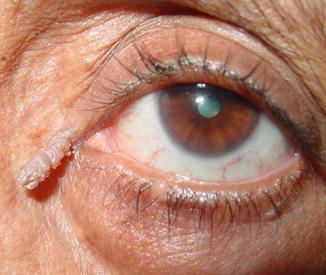

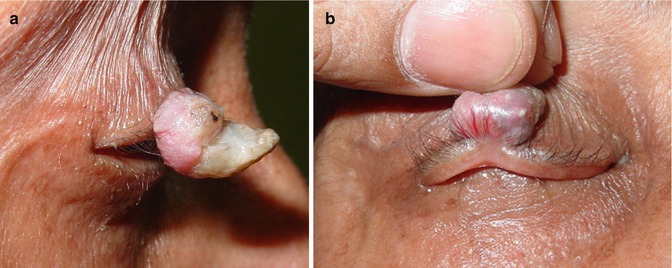


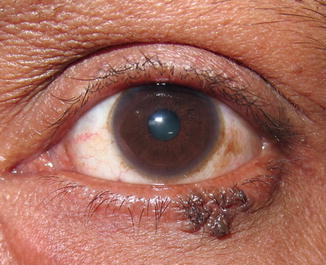


Fig. 5.1
(a) Small papillomatous growth over the inferior punctum. (b) Small papillomatous growth overlying the inferior punctum
Fig. 5.2
A large papillomatous growth from the lateral aspect of the lower lid
Fig. 5.3
A cutaneous horn formation
Fig. 5.4
A tubular squamous hyperplasia

Fig. 5.6
Another variant of cutaneous horn. Note the feeder vessel supplying nutrition to the lesion
Fig. 5.8
A pigmented papillomatous growth over the lateral periorbital skin

Fig. 5.10
A small pedunculated papillomatous mass in the lower lid

Fig. 5.12
A flat, pigmented papillomatous growth

Fig. 5.14
A pedunculated mass of viral origin

Fig. 5.16
The author’s small, flat upper-lid papillomatous lesion
5.1.2 Seborrheic Keratosis
5.1.2.1 Introduction
Seborrheic keratosis (basal cell papilloma, seborrheic warts) is a common benign lesion of the face and abdomen. It also may present on the lids of aging individuals.
5.1.2.2 Clinical Features
The lesions are well circumscribed, waxy, and friable and appear stuck to the skin. Some are covered by an adherent greasy-appearing scale and are raised above the surface of the skin. They may feel soft and greasy.
The lesions are round to oval, and multiple lesions may be aligned in the direction of the skin folds. They are very superficial and may be pigmented, from slight discoloration to a deep brown.
5.1.2.3 Prognosis
Seborrheic keratosis usually is asymptomatic but sometimes may cause pruritus and irritation.
5.1.2.4 Treatment Options
Treatment involves surgical excision or laser ablation.
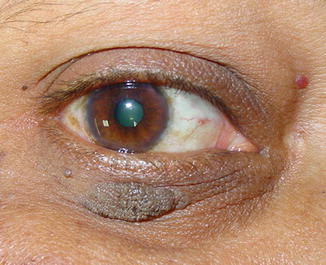









Fig. 5.17
Lower-lid seborrheic keratosis
Fig. 5.18
Lower-lid seborrheic keratosis extending up to the lid margin
Fig. 5.19
A pigmented localized seborrheic keratosis lesion
Fig. 5.20
A huge variant of lower-lid seborrheic keratosis. The patch appears to stick to the skin surface
Fig. 5.21
Another large patch of seborrheic keratosis
Fig. 5.22
Magnified view of a seborrheic keratosis patch. Note the waxy coloration. The lesion seems to be stuck to the skin, as if it can be peeled off
Fig. 5.23
Note the adherent greasy-appearing scale-like character of a seborrheic keratosis patch
Fig. 5.24
Scattered seborrheic keratosis may appear as a crop
Fig. 5.25
Patient in Fig. 5.24 from the left lateral aspect. Note the geographic distribution of the seborrheic keratosis
Fig. 5.26
Another interesting geographic distribution of seborrheic keratosis
5.1.3 Inverted Follicular Keratosis
5.1.3.1 Introduction
Inverted follicular keratosis is a benign cutaneous lesion almost similar in character to seborrheic keratosis. The term inverted follicular keratosis is a misnomer, as it was thought that these lesions arose from hair follicles. However, recent studies suggest that they basically are an irritated form of seborrheic keratosis.
5.1.3.2 Age of Presentation
Inverted follicular keratosis appears in middle age.
5.1.3.3 Clinical Presentation
Inverted follicular keratosis may present as nodular, papillomatous, or pigmented lesions. It is differentiated from seborrheic keratosis by its rapid growth pattern.
5.1.3.4 Treatment
Treatment consists of surgical removal.


Fig. 5.27
Pigmented, plaque-like follicular keratosis

Fig. 5.29
Pedunculated variant of follicular keratosis
5.1.4 Keratoacanthoma
5.1.4.1 Introduction
Keratoacanthoma is a form of pseudocarcinomatous hyperplasia. It recently was reclassified as a low-grade form of squamous carcinoma.
5.1.4.2 Age of Presentation
Keratoacanthoma usually occurs in middle age.
5.1.4.3 Clinical Features
The clinical appearance of keratoacanthoma is similar to that of a noduloulcerative type of basal cell carcinoma. It grows rapidly over a period of 2–6 months.
5.1.4.4 Treatment Options
Treatment options range from observation, to cryoapplication, to surgical resection. There have been some reports of spontaneous regression.




Fig. 5.30
Nodulated lesion with a flat surface: very classic of keratoacanthoma
Fig. 5.31
Close-up of Fig. 5.30. Note the flat lesion, with some amount of ulceration at the base. It sometimes is very difficult to differentiate this from the noduloulcerative variety of basal cell carcinoma. Only excision biopsy will confirm the exact pathology
Fig. 5.32
Keratoacanthoma over the cheek
Fig. 5.33
Keratoacanthoma over the upper lid margin
5.1.5 Actinic Keratosis
5.1.5.1 Introduction
Actinic keratosis, also called solar keratosis, is associated with chronic sun exposure. Actinic keratoses are significant because they are recognized as precursors of squamous cell carcinoma.
5.1.5.2 Age of Onset
Actinic keratosis is encountered commonly in patients older than 50 years who have fair skin.
5.1.5.3 Clinical Features
Clinically, the keratoses usually appear as nondescript, reddish-brown scaly patches in sun-exposed areas of the lids and are 3–10 mm in diameter.
5.1.5.4 Treatment Options
Isolated actinic keratoses may be treated with cryotherapy or curettage. However, because these lesions often are precancerous, excision with biopsy of larger lesions may be advisable.
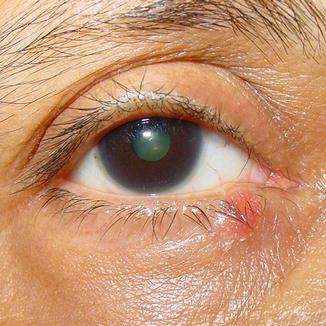


Fig. 5.34
Rough, red patches on the lid margin
Fig. 5.35
Reddish patches over the sun-exposed part of the upper lid margin
Fig. 5.36
Rough brown scaly patches on the inferior lid
5.2 Benign Sebaceous Gland Tumors
5.2.1 Sebaceous Gland Hyperplasia and Adenoma
5.2.1.1 Introduction
The sebaceous glands of the eyelid include the meibomian glands of the tarsal plate, the gland of Zeiss of the cilia, and the sebaceous gland of the caruncle. Tumors arising in these glands may be either benign (adenoma) or malignant (adenocarcinoma).
5.2.1.2 Clinical Presentation
Hyperplasia and adenoma of the sebaceous glands appear almost similar clinically; they appear as a yellowish nodule of the lid with a smooth surface. The caruncular variety is slightly more irregular in appearance.
5.2.1.3 Age of Presentation
Hyperplasia and adenoma of the sebaceous glands may present at any age but are more common in young adulthood.
5.2.1.4 Treatment
Benign tumors of the sebaceous gland of the lid usually never turn malignant. They may be observed, or a simple surgical excision may be planned.
5.2.1.5 Systemic Association
A systemic association with Muir-Torre syndrome has been reported. This syndrome is an autosomal dominant condition in which patients with cutaneous sebaceous tumors, basal cell carcinoma, or keratoacanthoma have a high incidence of visceral malignancy, especially colon cancer. Almost 70 % of these patients have a positive family history.
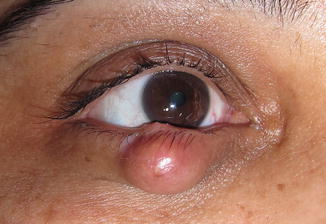




Fig. 5.37
Nodulated lower-lid meibomian gland hyperplasia
Fig. 5.38
Everted view of the case shown in Fig. 5.37. Note the well-encapsulated lesion under the tarsal conjunctiva
Fig. 5.39
Irregular sebaceous gland hyperplasia over the lid margin
Fig. 5.40
Everted view of the case shown in Fig. 5.39. Note the lesion under the tarsal conjunctiva, with some overlying vascularization and scarification
Fig. 5.41
Tiny sebaceous gland hyperplasia over the lid margin
5.3 Sweat Gland Tumors
5.3.1 Syringoma
Syringomas are benign tumors of the eccrine sweat glands around the lid and adnexae.
5.3.1.1 Age of Presentation
Syringomas are common in young females but may present at any age.
5.3.1.2 Clinical Presentation
Syringomas appear as subtle yellowish small nodulated elevations in the periorbital region. They may appear singly or in clusters.
5.3.1.3 Treatment
Because syringomas are benign in nature, simple observation is sufficient. If they become large or cosmetically undesirable, surgical excision is the treatment of choice. Other options include ablative carbon dioxide or argon laser resurfacing.
5.3.1.4 Prognostic Factors
The prognosis is good, with practically no chance of malignant transformation.



Fig. 5.42
Scattered, subtle, yellowish, small nodulated elevations in the periorbital region, a presentation of eyelid syringoma

Fig. 5.44
Yellowish cluster of tiny nodules over the nasal bridge and medial portion of the cheek, suggesting syringoma
Fig. 5.45
Tiny yellowish nodular cluster of syringomas in the periorbital region
5.3.2 Eyelid Pleomorphic Adenoma
Pleomorphic adenoma (also referred to as benign mixed tumor or chondroid syringoma) is among the rarest of the adenomas and adenocarcinomas of the eyelids. Pleomorphic adenomas may arise from the sweat glands in the dermis of the eyelid skin. This rare cutaneous neoplasm may arise from eccrine or apocrine glands.
5.3.2.1 Age of Presentation
Pleomorphic adenoma usually affects the elderly.
5.3.2.2 Clinical Presentation
Pleomorphic adenoma usually presents as a nodulated lump on the upper or lower eyelid margin, which has been slowly increasing in size. Clinical differentiation from other, similar nodulated growths is very difficult.
5.3.2.3 Treatment
Treatment is surgical excision followed by reconstruction (similar to the management of basal cell carcinoma).



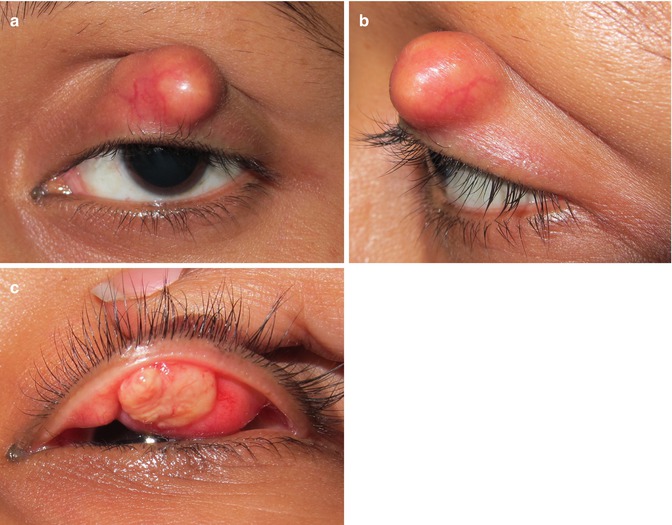
Fig. 5.46
Slightly irregular nodulated lump over the lower eyelid margin, which has been slowly increasing in size
Fig. 5.47
Lid marginal growth of pleomorphic adenoma
Fig. 5.48
Well-localized circular nodule over the medial canthus. It turned out to be pleomorphic adenoma of the eyelid
Fig. 5.49




(a) Large pleomorphic adenoma, which has been growing over the upper lid. (b) Lateral view of the same lesion. (c) Everted view of the same lesion
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
