Bag-in-the-Lens
Marie-José Tassignon
Modern-day cataract surgeons have struggled to address the most common postoperative complication, posterior capsule opacification (PCO). In cases where the posterior capsule has been kept intact, the term PCO is used. However, in cases where a primary posterior continuous curvilinear capsulorhexis (PPCCC) has been performed (which is considered standard in cataract surgery of babies and infants), the term visual axis opacification (VAO) or visual axis reproliferation (VAR) is used. Even after PPCCC, the incidence of VAO has been reported ranging from 8% to 80%.1,2 The highest incidences occur when the child presents with associated ocular anomalies and is operated at <6 months of age. VAO occurs very quickly postoperatively, within the first 6 months, however the incidence of VAO does not increase very much after the first postoperative year.
Traditionally, the intraocular lens (IOL) is placed within the capsular bag. This approach can be thought of as a lens-in-the-bag (LIB) implantation. A new concept of lens implantation was introduced in the early 2000s, called the bag-in-the-lens (BIL) implantation technique (Fig. 27.1A; Table 27.1). The BIL technique has been routinely implanted by the author in adults since 2004. The BIL technique requires a slightly adapted surgical approach. Compared to the traditional LIB technique, all surgical steps in the BIL procedure need more precision, particularly sizing of the anterior and posterior capsulorhexis. This requirement for precision is the reason that from its conception, some surgeons have felt that it was too difficult in theory to perform. Now that results of BIL have been published, this stigma is decreasing. The outcome results of BIL show it to be superior to other techniques in preventing VAO, which are as low as 0% in adult eyes3,4 provided the lens could be implanted in the appropriate way. Pediatric ophthalmologists were less resistant to the BIL technique because they commonly perform PPCCC, a procedure that is done routinely by only a few high-volume adult cataract surgeons worldwide.
The BIL involves the use of a twin capsulorhexis IOL design (see Fig. 27.1B and C) requiring anterior and posterior capsulorrhexes that are matched in size. The term matching is used rather than congruent on purpose, since it is more important to have similar capsulorhexis sizes than shapes. The idea behind the BIL technique is that if both capsules are stretched around the 5-mm central optic diameter as currently proposed (though larger diameters are available if needed), the lens epithelial cells (LECs) will be captured within the remaining peripheral space of the capsular bag, and their proliferation will be limited to this space, so that the visual axis will remain clear.5,6,7,8,9
The BIL is manufactured by the Morcher, Germany, under references 89 A/D/F (see Table 27.1). It is made of hydrophilic Coacryl biomaterial with 28% water content. The 89A reference is the standard type of BIL with an overall length of 7.5 mm and a biconvex optic of 5.0 mm. The company proposes to use the A-constant of 118.2. Based on our clinical experience, I prefer to use 118.0 for the A-constant. The 89D type of BIL is mainly used for very small eyes. It has the same design but with 4.5 mm optic. The 89F type is an adaptation of the BIL at the request of Claus Eckhart from Germany, who desired a larger anterior haptic with an overall diameter of 8.5 mm to be used in his combined cataract-vitrectomy surgeries with gas or silicone tamponade. This larger haptic design precludes the incidence of iris capture postoperatively.
Since the anterior capsule in children is highly elastic, an anterior continuous curvilinear capsulorhexis (ACCC) is more challenging to perform even more so in babies. Different solutions have been proposed in the literature to increase the performance of this surgical step.10,11,12 Our approach was to design a ring caliper made of polymethyl methacrylate, which can be cut in a ring of 0.2 mm of cross-sectional thickness and variable inner overall diameter matching the size of the desired capsulorhexis. This ring caliper presents properties of flexibility and memory that are ideal for the intended purpose
(Table 27.2; Fig. 27.2). The caliper ring was introduced in 2006.13 The device can be inserted into the anterior chamber through a 1.2-mm corneoscleral opening by means of a caliper ring positioner (see Table 27.2) and is stabilized on top of the anterior capsule by means of a 1% sodium hyaluronate solution with high viscosity. This ophthalmic viscosurgical device (OVD) has the advantage of flattening the anterior capsule, making it easier for the surgeon to perform an ACCC in a reproducible and controlled fashion. I personally use Healon® GV for this purpose (Advanced Medical Optics [AMO], Santa Ana, CA). Capsular staining by means of trypan blue 0.1% (VisionBlue, Dutch Ophthalmic Research Center)14 is in our hands only used for treating white cataracts or congenital anterior capsule disorders. In the latter cases, the staining will enable careful dissection of the embryologic remnants of the anterior part of the tunica vasculosa from the underlying anterior capsule (Fig. 27.3).
(Table 27.2; Fig. 27.2). The caliper ring was introduced in 2006.13 The device can be inserted into the anterior chamber through a 1.2-mm corneoscleral opening by means of a caliper ring positioner (see Table 27.2) and is stabilized on top of the anterior capsule by means of a 1% sodium hyaluronate solution with high viscosity. This ophthalmic viscosurgical device (OVD) has the advantage of flattening the anterior capsule, making it easier for the surgeon to perform an ACCC in a reproducible and controlled fashion. I personally use Healon® GV for this purpose (Advanced Medical Optics [AMO], Santa Ana, CA). Capsular staining by means of trypan blue 0.1% (VisionBlue, Dutch Ophthalmic Research Center)14 is in our hands only used for treating white cataracts or congenital anterior capsule disorders. In the latter cases, the staining will enable careful dissection of the embryologic remnants of the anterior part of the tunica vasculosa from the underlying anterior capsule (Fig. 27.3).
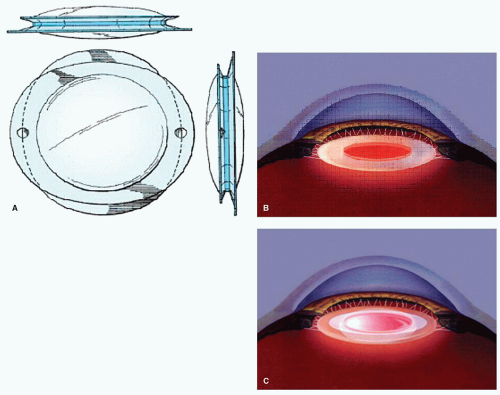 Figure 27.1. Bag-in-the-lens. A: Front and side view of the technical drawing of the BIL. B: Schematic drawing of the position of the capsular bag after having done a sized and centered anterior and posterior capsulorhexis. C: Schematic drawing of the BIL in the proper position within the anterior chamber. |
Table 27.1 TECHNICAL PROPERTIES OF THE BIL | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
In children, a caliper ring of 4.5-mm internal diameter (4 L Tassignon ring caliper, Morcher, Germany) is preferred instead of a 5-mm internal caliper (5 Tassignon caliper ring, Morcher, Germany) as used in adults (see Table 27.2). By using slightly smaller caliper rings in babies and children, the surgeon includes a safety margin of 0.5 mm for the ACCC to compensate for the highly elastic properties of the capsular bag. Before starting the puncture of the anterior capsule, the ring
caliper is centered on top of the anterior capsule using the first and fourth Purkinje reflex images (Fig. 27.4) of the light of our microscope (we use the Zeiss Microscope S8, Germany) present in the anterior segment of the eye (Purkinje I reflex corresponds to the anterior face of the cornea, and Purkinje IV reflex comes from the back surface of the lens). The pupillary center can also be used for centering when the iris is optimally dilated and regular in shape, though this is not always the case, especially not in eyes with associated anomalies. The anterior capsule puncture is performed preferably with a 30-gauge needle in very young children. In children older than 3 years, the anterior capsule can be punctured by means of the angulated tip of a microforceps. The microforceps I preferably use are the Ikeda capsulorhexis microforceps with 30-degree angulation of the grasping tips (FR-2268, EyeTech, UK) (see Table 27.2). The anterior capsulorhexis is performed by frequent grasping and regrasping and by following the internal border of the caliper ring as a guide



caliper is centered on top of the anterior capsule using the first and fourth Purkinje reflex images (Fig. 27.4) of the light of our microscope (we use the Zeiss Microscope S8, Germany) present in the anterior segment of the eye (Purkinje I reflex corresponds to the anterior face of the cornea, and Purkinje IV reflex comes from the back surface of the lens). The pupillary center can also be used for centering when the iris is optimally dilated and regular in shape, though this is not always the case, especially not in eyes with associated anomalies. The anterior capsule puncture is performed preferably with a 30-gauge needle in very young children. In children older than 3 years, the anterior capsule can be punctured by means of the angulated tip of a microforceps. The microforceps I preferably use are the Ikeda capsulorhexis microforceps with 30-degree angulation of the grasping tips (FR-2268, EyeTech, UK) (see Table 27.2). The anterior capsulorhexis is performed by frequent grasping and regrasping and by following the internal border of the caliper ring as a guide
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
