Lids: Thickened (tylosis), inflamed, irregular lid margins with telangectasias are common features. Infection of the base of the cilia may lead to deposition of fibrin, which eventually hardens and separates from the lid as a disc upon growth of the cilia. What results is the classic collarette, pierced by a cilium (Fig. 6-1). Collarettes are the hallmark of staphylococcal blepharitis and should be differentiated from the scaly, grayish sleeve that is associated with Demodex infestation. In addition, fine flakes of keratinized epithelium may surround the base and shaft of the lashes. This greasy crust is often referred to as scurf and may represent seborrheic disease. Deeper infection, within the cilia follicle, may result in poliosis (white lashes), madarosis (missing lashes), and trichiasis (misdirected lashes). Other findings may include ulcerated lid margins, meibomitis, plugging or pouting of the meibomian orifices, hordeola, chalazia, and/or preseptal cellulitis.
Cornea and Conjunctiva: Chronic inflammation of the lids may result in micropapillary conjunctivitis, with occasional exacerbations. Exotoxins produced by staphylococcal organisms are typically implicated in a toxic conjunctivitis, as well as the development of inflammatory infiltrates of the cornea (Figs. 6-2 and 6-3). Fine punctate keratopathy may be present in the inferior portions of the cornea. Subepithelial infiltrates are usually found adjacent to the limbus, most prominently superiorly and inferiorly and where the lid crosses the limbus (11, 2, 4, and 8 o’clock). An infiltrate may necrose, resulting in a sterile marginal ulcer. If the corneal involvement is chronic or recurrent, visually significant vascularization and scarring may occur. In addition, phlyctenules may form, which are immunologic reactions to bacterial exotoxins. Phlyctenules are typically raised lesions consisting of lymphocytes. They may be found on the cornea or conjunctiva but are most frequently seen in the limbal area. Phlyctenules may ulcerate with neutrophils appearing as necrosis occurs. (See section on Phlyctenulosis.)
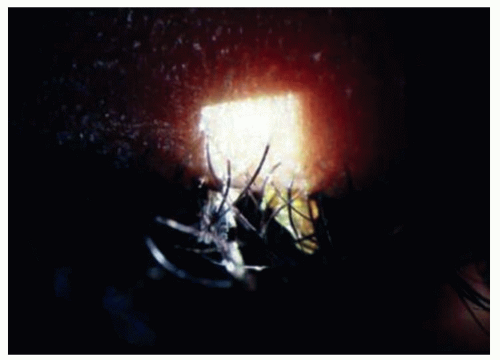 Figure 6-1. Bacterial blepharitis demonstrating classic sign collarettes. |
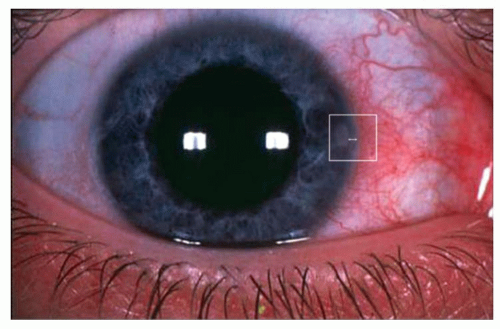 Figure 6-2. Marginal infiltrate secondary to bacterial blepharitis. Note the infliltrate present inside the box. The horizontal line delineates the area of clear cornea between the infiltrate and the limbus suggesting a noninfectious lesion. |
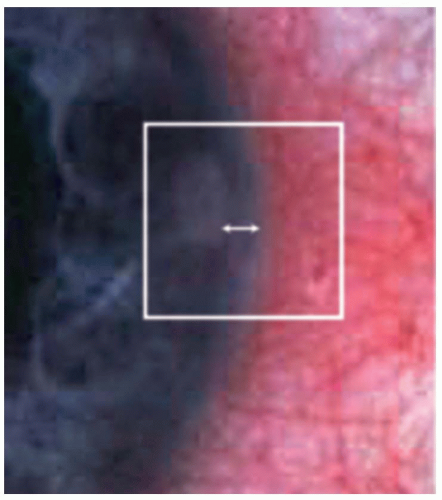 Figure 6-3. Higher magnification view of marginal infiltrate seen in image 2. Note the lucid area between limbus and lesion. |
should be gently drawn through the upper and lower cul-de-sacs (total contact time should be ˜5 seconds) and then applied to both blood and chocolate agar. A new swab should be used to wipe the inferior and superior lid margins and then applied to the same plates. The procedure should be repeated for the opposite eye using fresh swabs (Fig. 6-4).
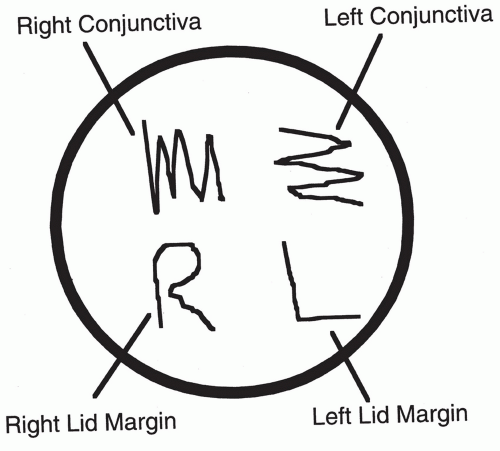 Figure 6-4. Staphylococcus epidermidis is commonly found on normal patients, although heavy growth is more significant. Any growth of S. aureus maybe significant, but is isolated in over 50% of patients. Sensitivity testing should be performed in cases resistant to emperic treatment. |
Tetracycline (do not use in pregnant women or children under age 8, also photosensitizing effects may occur with sun exposure), 250 mg q.i.d., p.o. × 2 to 4 months.
Erythromycin, 250 mg q.i.d. p.o. × 2 to 4 months.
Doxycycline or minocycline, 50 to 100 mg b.i.d. p.o. × 1 month and then tapered and used for several additional months. Lower doses of doxycycline have also been shown to be effective (e.g., Oracia—doxycylcline capsules 40, 30 mg Immediate Release, and 10 mg Delayed Release beads) and help to reduce the common GI side effects associated with higher doses.
If a penicillinase resistant antibiotic is necessary, consider cloxacillin:
Greater than 20 kg—250 mg q6h p.o. × 10 days or
Less than 20 kg—50 mg/kg/d in equally divided doses q6h p.o. × 10 days
Flaxseed oil has been shown to thin the meibomian gland secretions, while medical grade fish oil has a profound anti-inflammatory effect. A combination of the two oils (e.g., TheraTears Nutrition) can be very effective and convenient for the patient with meibomitis and dry eye.
Onset is usually within 12 hours of exposure and is rapidly progressive.
The patient reports irritation, redness, pain, and copious, thick, creamy purulent discharge. The eyelids may be adherent upon awakening. Infection may start in one eye and migrate to the other eye because of hand-to-eye contact or fomites.
TABLE 6-1 Common Conjunctival Bacterial Pathogens in Adults | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Redness, irritation, grittiness, and mucopurulent discharge with mattering that causes the lids to stick together on awakening are common symptoms. Pain is usually absent.
Visual acuity is typically unaffected.
The infection usually starts unilaterally but often spreads to the fellow eye within a few days due to hand-to-eye contact.
TABLE 6-2 Differential Diagnosis of Acute Conjunctivitis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Symptoms include mild, chronic redness and irritation of the conjunctiva and lids.
Visual acuity is usually unaffected.
Discharge may be mucoid or watery.
The classic presentation is a severely injected, chemotic conjunctiva with copious purulent discharge. Marked lid edema, tenderness, and redness are common.
PA nodes are often enlarged and tender to palpation.
Corneal involvement may occur, resulting in SPK or frank corneal ulceration (e.g., Neisseria may invade an intact cornea). Peripheral ring
infiltrates and ulcers may be seen in gonococcal keratitis, resulting in corneal perforation if left untreated.
Conjunctival pseudomembranes may be evident.
Neisseria meningitidis may gain access to the central nervous system through infection of the conjunctiva via hematogenous spread, resulting in infectious meningitis. Other concomitant infections may involve the genitourinary tract and/or the pharynx if Neisseria gonorrhoeae is responsible for the underlying infection. The genital symptoms usually precede the ocular symptoms by a week or two. Rarely, urethritis may be absent due to direct inoculation of the organism into the eye.
Other potential ocular and systemic complications of gonococcal conjunctivitis include iritis, lid abscess, dacryoadenitis, and septicemia.
The principle causes of acute bacterial conjunctivitis are two Gram-positive organisms, Staphylococcus aureus and Streptococcus pneumoniae, and two Gram-negative bacteria, N. gonorrhoeae and Haemophilus species (Figs. 6-5 and 6-6)
The typical presentation is a mild to moderate diffuse or segmental, bulbar, and tarsal conjunctival injection with canthal involvement.
There is usually minimal eyelid involvement and no PA lymphadenopathy, except in very severe cases.
A papillary conjunctival tissue reaction is common.
Pseudomembranes or small subconjunctival hemorrhages may be present (Streptococcus and Haemophilus).
Mucopurulent discharge may be mild to moderate and may seal the eyelids upon awakening.
The cornea is usually uninvolved; however, a mild, inferior punctate keratitis may be present.
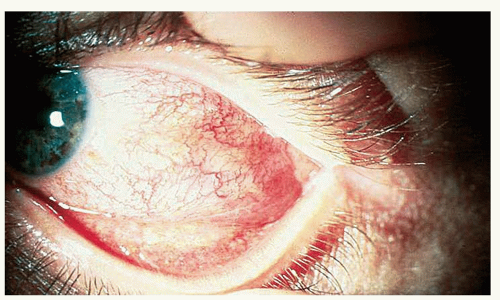 Figure 6-5. Streptococcal bacterial conjunctivitis. Note the purulence in the cul-de-sac. |
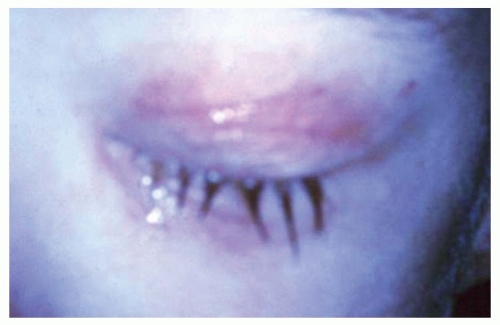 Figure 6-6. Haemophilus blepharoconjunctivitis in a young child. Note the bluish/purple lid coloration which is common in Haemophilus infection. |
This disorder has the same clinical presentation as acute conjunctivitis, with the addition of pseudomembranes or membranes and markedly swollen lids.
Pseudomembranes (fibrinous exudate on the conjunctival surface without deep attachments that can be removed without significant bleeding) in bacterial conjunctivitis are most commonly caused by Neisseria or Streptococcus pyogenes; true membranes (fibrin strands project into the conjunctiva between epithelial cells, causing bleeding when removed) are most often caused by Corynebacterium diphtheriae.
Pain is a prominent feature of membranous conjunctivitis.
Any severe bacterial conjunctivitis can cause a pseudomembrane.
Membranous conjunctivitis may be associated with corneal ulceration and/or permanent loss of goblet cells, which could result in OSDs, palpebral scarring, and chronic dry eye. Palpebral scars may be present as a result of resolved membranes. Viral conjunctivitis is more commonly associated with membranous conjunctivitis.
Staphylococcus
The lids may show signs of crusting and formation of collerettes with associated madarosis and trichiasis. In addition, the skin of the lids may show an eczematous-type reaction. The bulbar conjunctiva may be mildly to moderately injected with or without the presence of phlyctenules. The palpebral conjunctiva usually demonstrates a papillary reaction. The cornea may be involved with inferior punctate keratitis, marginal infiltrates, or micropannus as a result of the presence of bacterial exotoxins. (See Bacterial Blepharitis.)
Moraxella
Moraxella may cause mild to moderate papillary conjunctivitis without corneal involvement. It may also result in angular blepharoconjunctivitis (Staphylococcus has also been implicated as a common cause in this presentation). On occasion, Moraxella may cause a chronic follicular conjunctivitis with corneal involvement, including punctate keratitis, subepithelial infiltrates, and preauricular lymphadenopathy. This latter presentation could be confused with adenovirus or chlamydial infections.
Cytology
PMN response with intracellular bacteria.
Gram stain
Gram-negative intracellular, diplococci, with many PMNs—Neisseria.
Gram-negative bacilli or coccobacilli—H. influenzae.
Cultures
Purulent discharge should be streaked on blood and chocolate agar and incubated at 37° in 10% CO2 or on a Thayer-Martin plate. Antibiotic sensitivities should also be performed.
Cytology
PMN response.
Gram stain
Presence of bacteria. The clinician should note the morphology of the organism (e.g., rod, club, or cocci) as well as other characteristic features of the organism (e.g., clusters, chains).
Cultures
Cultures are necessary in persistent infections that do not respond to empiric treatment and should include plating on blood and chocolate agar as well as thioglycolate broth. Antibiotic sensitivities should also be requested.
Cytology
PMN response.
Gram stain
Gram-positive cocci arranged in chains or pairs (S. pyogenes).
Gram-positive pleomorphic rods that appear drumstick shaped (C. diphtheriae).
Gram-negative diplococci (Neisseria).
Cultures
Beta-hemolysis on blood agar (S. pyogenes).
Loeffler’s blood serum (C. diphtheriae).
Cytology
PMN response.
Gram stain
Gram-positive cocci in clusters (Staphylococcus).
Gram-negative diplobacilli usually arranged in pairs (Moraxella).
Cultures
Staphylococcus: Blood agar with coagulase testing (S. aureus—positive; S. epidermidis—negative) and mannitol fermentation to differentiate S. aureus from S. epidermidis; sensitivities should be performed because of propensity toward resistance.
Moraxella: Enriched media such as Loeffler’s medium.
All cases of Neisseria infection must be reported to the Center for Disease Control (CDC)
Systemic treatment is mandatory in this condition; topical treatment is only adjunctive.
Hospitalization is not uncommon, especially if keratitis exists.
The patient and sexual partners must be promptly referred for venereal aspects of N. gonorrheae and coinfection with other sexually transmitted diseases (STDs) such as HIV, syphilis, and/or chlamydia to avoid significant morbidity. Care should be taken to protect patient confidentiality.
Topical therapy (inadequate as the only form of treatment)
Warm saline rinses q.i.d. until the discharge has resolved.
Erythromycin, tobramycin, or bacitracin ung q.i.d.
Fluoroquinolones (FQs) (ciprofloxacin, levofloxacin, ofloxacin, moxifloxacin, or gatifloxacin) q2h × 4 to 7 days.
Systemic therapy
No keratitis present
ceftriaxone 250 mg to 1g IM or IV as a single dose in adults
Keratitis present
ceftriaxone 1 g IV q12-24h × 3 days or until symptoms subside and there is an appropriate clinical response.
Treatment for a concomitant chlamydial infection includes erythromycin, tetracycline, or sulfacetamide ointment two to three times per day plus:
azithromycin 1 g p.o. (single dose) preferred treatment, or
doxycycline 100 mg b.i.d. p.o. × 1 to 2 weeks
C. diphtheriae
C. diphtheriae antitoxin 10,000 to 100,000 units parenterally
Erythromycin, penicillin, or
Clindamycin, or
Topical penicillin (must be compounded by pharmacy)
S. pyogenes
Topical: bacitracin or erythromycin ung b.i.d.-q.i.d.
Topical
Lid hygiene with a commercial lid scrub preparation (diluted baby shampoo may be substituted but may be more irritating to the eye). Warm compresses may also facilitate management.
Topical bacitracin, Polysporin, or erythromycin ointment applied to the lids and lashes hs × 3 to 4 weeks and then tapered to a maintenance dose.
Topical antibiotic/steroid gtts may be helpful for bulbar conjunctival and corneal involvement:
Maxitrol drops (neomycin/polymyxin B/dexamethasone) 1 gtt. t.i.d. × 7 to 10 days, or
TobraDex (tobramycin/dexamethasone) 1 gtt. t.i.d. × 7 to 10 days, or
Zylet (loteprednol etabonate 0.5%/tobramycin) 1 gtt. t.i.d. × 7 to 10 days
Patients who do not respond to therapy may be carriers and require culturing of the nasopharynx, ear canal, and skin, as well as systemic treatment.
Systemic:
Tetracycline (do not use tetracycline in pregnant women or children under age 8 and be aware of photosensitizing effects of drug) or erythromycin 250 mg q.i.d. p.o. × 2 to 4 months or
Doxycycline or minocycline 50 to 100 mg b.i.d. p.o. × 1 month and then tapered and used for several additional months or
If penicillinase resistant antibiotic is necessary, consider cloxacillin:
Greater than 20 kg—250 mg q6h p.o. × 10 days or
Less than 20 kg—50 mg/kg/d in equally divided doses q6h p.o. × 10 days
Candida albicans, Chlamydia spp., H. aegyptius, herpes simplex virus (HSV), and various nematodes.
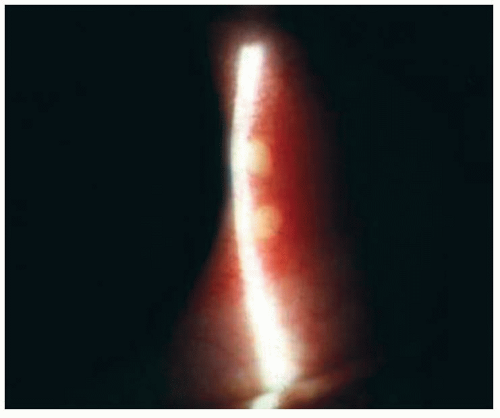 Figure 6-7. Phlyctenulosis secondary to bacterial blepharitis in a 12-year-old Hispanic female. Note the elevated lesions at the limbus. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


