6 BACTERIAL INFECTIOUS DISEASES
Bacterial Blepharitis
Marcus G. Piccolo and Victor Malinovsky
ICD-9: 373.01—BLEPHARITIS, ULCERATIVE
 THE DISEASE
THE DISEASE
Pathophysiology
Blepharitis occurs when there is colonization and infection of the lid margin, lid glands, or cilia follicle by bacterial pathogens. The liberation of bacterial enzymes (lipases and esterases) and exotoxins may result in inflammation and potential morphological/anatomical changes to the lid, cilia, conjunctiva, and cornea. Inflammatory changes of the external adnexa and alteration of the sebaceous secretions may also produce various ocular surface disorders (OSD).
Etiology
The most common pathogens responsible for bacterial blepharitis are Staphylococcus aureus, Staphylococcus epidermidis, Propionibacterium acnes, and Moraxella spp. Other causes of infectious blepharitis should be excluded (i.e., herpes simplex, herpes zoster, Candida spp. vaccinia, and molluscum).
The Patient
Clinical Symptoms
Chronic itching, redness, dryness, burning, tearing, foreign body sensation, photophobia, conjunctival injection, red lids, and lash crusting, with intermittent exacerbations, are common features. Symptoms are typically worse in the morning, and the diurnal variation of burning often differentiates meibomitis from common dry eye.
Clinical Signs
- Lids: Thickened (tylosis), inflamed, irregular lid margins with telangectasias are common features. Infection of the base of the cilia may lead to deposition of fibrin, which eventually hardens and separates from the lid as a disc upon growth of the cilia. What results is the classic collarette, pierced by a cilium (Fig. 6-1). Collarettes are the hallmark of staphylococcal blepharitis and should be differentiated from the scaly, grayish sleeve that is associated with Demodex infestation. In addition, fine flakes of keratinized epithelium may surround the base and shaft of the lashes. This greasy crust is often referred to as scurf and may represent seborrheic disease. Deeper infection, within the cilia follicle, may result in poliosis (white lashes), madarosis (missing lashes), and trichiasis (misdirected lashes). Other findings may include ulcerated lid margins, meibomitis, plugging or pouting of the meibomian orifices, hordeola, chalazia, and/or preseptal cellulitis.
- Cornea and Conjunctiva: Chronic inflammation of the lids may result in micropapillary conjunctivitis, with occasional exacerbations. Exotoxins produced by staphylococcal organisms are typically implicated in a toxic conjunctivitis, as well as the development of inflammatory infiltrates of the cornea (Figs. 6-2 and 6-3). Fine punctate keratopathy may be present in the inferior portions of the cornea. Subepithelial infiltrates are usually found adjacent to the limbus, most prominently superiorly and inferiorly and where the lid crosses the limbus (11, 2, 4, and 8 o’clock). An infiltrate may necrose, resulting in a sterile marginal ulcer. If the corneal involvement is chronic or recurrent, visually significant vascularization and scarring may occur. In addition, phlyctenules may form, which are immunologic reactions to bacterial exotoxins. Phlyctenules are typically raised lesions consisting of lymphocytes. They may be found on the cornea or conjunctiva but are most frequently seen in the limbal area. Phlyctenules may ulcerate with neutrophils appearing as necrosis occurs. (See section on Phlyctenulosis.)

Figure 6-1. Bacterial blepharitis demonstrating classic sign collarettes.
Figure 6-2. Marginal infiltrate secondary to bacterial blepharitis. Note the infliltrate present inside the box. The horizontal line delineates the area of clear cornea between the infiltrate and the limbus suggesting a noninfectious lesion.
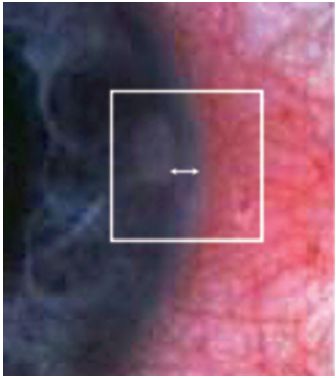
Figure 6-3. Higher magnification view of marginal infiltrate seen in image 2.Note the lucid area between limbus and lesion.
Demographics
Bacterial blepharitis may occur in all ages, including children. Bilaterality is the rule, although unilateral involvement may rarely occur. Women are more frequently affected than men.
Significant History
Dry eyes and tear deficiencies may be contributing factors. Other conditions found in association with bacterial blepharitis include acne vulgaris, ocular rosacea, seborrheic dermatitis, eczema, impetigo, and other infectious skin diseases.
Ancillary Tests
The diagnosis of bacterial blepharitis is usually based on clinical findings; however, cultures of the conjunctival cul-de-sac and lid margins should be performed and plated on chocolate and blood agar in patients who do not respond to empiric therapy. Testing tear insufficiency is often appropriate because of the frequent association with dry eyes/OSD.
Technique for culture: A calcium alginate swab, moistened with a liquid medium such as thioglycolate broth, should be gently drawn through the upper and lower cul-de-sacs (total contact time should be ~5 seconds) and then applied to both blood and chocolate agar. A new swab should be used to wipe the inferior and superior lid margins and then applied to the same plates. The procedure should be repeated for the opposite eye using fresh swabs (Fig. 6-4).
Figure 6-4. Staphylococcus epidermidis is commonly found on normal patients, although heavy growth is more significant. Any growth of S. aureus maybe significant, but is isolated in over 50% of patients. Sensitivity testing should be performed in cases resistant to emperic treatment.
The Treatment
Topical
Three basic disorders need to be evaluated and treated in patients who have meibomitis: inflammation, bacterial overgrowth, and thickened meibomian gland secretions.
Warm compresses followed by a commercial lid scrub, such as SteriLid (diluted baby shampoo may be substituted but may be more irritating to the eye), are the mainstay of therapy. Gentle lid margin scrubs may be required several times per day depending on the severity of the disease and then tapered to a maintenance schedule as the condition improves. Warm compresses and lid scrubs decrease the bioload on the lids and also serve to thin and stimulate the flow of the meibomian glands. In some cases, the use of artificial tears may be necessary for further management of the associated OSD.
Azithromycin 1% (AzaSite) gtts, 1 gtt. b.i.d. × 2 days and then 1 gtt. q.d. × 28 days, has been shown to be an effective antibiotic and may also help to restore the lipid complex to a more normal state. Patients should be reminded to rub the azithromycin drop into the base of the lashes with a clean finger. As an alternative, topical bacitracin or erythromycin ointment applied to the lids and lashes qhs × 3 to 4 weeks and then tapered to a maintenance dose may also be effective. Alternating topical antibiotics may reduce the tendency of developing resistant organisms.
Topical steroid/antibiotic drops may be helpful for bulbar conjunctival and corneal involvement:
Maxitrol drops (neomycin/polymyxin B/dexamethasone) 1 gtt. q.i.d. × 7 to 10 days, or
Zylet (tobramycin/loteprednol etabonate 0.5%) 1 gtt. q.i.d. × 7 to 10 days, or
Tobradex (tobramycin/dexamethasone) 1 gtt. q.i.d. × 7 to 10 days
Unresponsive patients may be carriers and require culturing of the nasopharynx, ear canal, and skin, as well as systemic antibiotic therapy.
Systemic
Oral antibiotics are not primarily used in this condition for their antibacterial effect, but rather for their anti-inflammatory properties and by inhibiting bacterial enzymes that cause saponification of meibomian gland secretions. Suggested regimens include
- Tetracycline (do not use in pregnant women or children under age 8, also photosensitizing effects may occur with sun exposure), 250 mg q.i.d., p.o. × 2 to 4 months.
- Erythromycin, 250 mg q.i.d. p.o. × 2 to 4 months.
- Doxycycline or minocycline, 50 to 100 mg b.i.d. p.o. × 1 month and then tapered and used for several additional months. Lower doses of doxycycline have also been shown to be effective (e.g., Oracia—doxycylcline capsules 40, 30 mg Immediate Release, and 10 mg Delayed Release beads) and help to reduce the common GI side effects associated with higher doses.
- If a penicillinase resistant antibiotic is necessary, consider cloxacillin:
1. Greater than 20 kg—250 mg q6h p.o. × 10 days or
2. Less than 20 kg—50 mg/kg/d in equally divided doses q6h p.o. × 10 days
This regimen is most likely used in more serious conditions such as preseptal cellulitis.
- Flaxseed oil has been shown to thin the meibomian gland secretions, while medical grade fish oil has a profound anti-inflammatory effect. A combination of the two oils (e.g., TheraTears Nutrition) can be very effective and convenient for the patient with meibomitis and dry eye.
- Doxycycline or minocycline, 50 to 100 mg b.i.d. p.o. × 1 month and then tapered and used for several additional months. Lower doses of doxycycline have also been shown to be effective (e.g., Oracia—doxycylcline capsules 40, 30 mg Immediate Release, and 10 mg Delayed Release beads) and help to reduce the common GI side effects associated with higher doses.
In general, blepharitis is a chronic condition, and treatment is aimed at control rather than cure. It is likely that some form of maintenance therapy, such as daily lid hygiene, will be required lifelong.
Bacterial Conjunctivitis
Marcus G. Piccolo and Victor Malinovsky
ICD-9: 372.0—CONJUNCTIVITIS, ACUTE, UNSPECIFIED
ICD-9: 372.11—CONJUNCTIVITIS, CHRONIC, SIMPLE
ICD-9: 098.49—GONOCOCCAL, EYE INFECTION, OTHER
ICD-9: 098.4—CONJUNCTIVITIS, GONOCOCCAL, NEONATORUM
ICD-9: 372.04—CONJUNCTIVITIS, MEMBRANOUS
 THE DISEASE
THE DISEASE
Pathophysiology
Bacterial conjunctivitis results from infection of the conjunctival tissue with bacterial pathogens. The resultant inflammatory process may present with a wide range of severity and clinical appearances.
Etiology
Bacterial conjunctivitis results when a bacterial inoculation overcomes the natural defense mechanisms of the conjunctiva. The pathogens may be normal flora of the conjunctiva or lids (e.g., silent dacryocystitis) or may be the result of inoculation from adjacent sites of infection, hand-to-eye contact, or airborne respiratory droplets. The defense mechanisms of the conjunctiva include the mechanical actions of the lids and tears; tear enzymes such as lysozyme, lactoferin, and B-lysin; immunoglobulins (IgA and IgG) present in the tears; conjunctival-associated lymphoid tissue; and an intact conjunctival epithelial barrier.
Bacterial conjunctivitis can be classified as hyperacute, acute, pseudomembranous/membranous, and chronic (Table 6-1).
TABLE 6-1 Common Conjunctival Bacterial Pathogens in Adults

The Patient
Clinical Symptoms
Hyperacute Conjunctivitis
TABLE 6-2 Differential Diagnosis of Acute Conjunctivitis
From: JD Lanier.
- Onset is usually within 12 hours of exposure and is rapidly progressive.
- The patient reports irritation, redness, pain, and copious, thick, creamy purulent discharge. The eyelids may be adherent upon awakening. Infection may start in one eye and migrate to the other eye because of hand-to-eye contact or fomites.
- Visual acuity is unaffected if the cornea is not involved and if the discharge can be irrigated from the corneal surface. Vision can be potentially affected by adherent discharge and by lid swelling, but if discharge is removed from the cornea, then visual acuity should improve.
Acute Conjunctivitis (Table 6-2).
- Redness, irritation, grittiness, and mucopurulent discharge with mattering that causes the lids to stick together on awakening are common symptoms. Pain is usually absent.
- Visual acuity is typically unaffected.
- The infection usually starts unilaterally but often spreads to the fellow eye within a few days due to hand-to-eye contact.
Membranous Conjunctivitis (Same as Acute Conjunctivitis)
Chronic Conjunctivitis
- Symptoms include mild, chronic redness and irritation of the conjunctiva and lids.
- Visual acuity is usually unaffected.
- Discharge may be mucoid or watery.
Clinical Signs
Hyperacute Conjunctivitis
- The classic presentation is a severely injected, chemotic conjunctiva with copious purulent discharge. Marked lid edema, tenderness, and redness are common.
- PA nodes are often enlarged and tender to palpation.
- Corneal involvement may occur, resulting in SPK or frank corneal ulceration (e.g., Neisseria may invade an intact cornea). Peripheral ring infiltrates and ulcers may be seen in gonococcal keratitis, resulting in corneal perforation if left untreated.
- Conjunctival pseudomembranes may be evident.
- Neisseria meningitidis may gain access to the central nervous system through infection of the conjunctiva via hematogenous spread, resulting in infectious meningitis. Other concomitant infections may involve the genitourinary tract and/or the pharynx if Neisseria gonorrhoeae is responsible for the underlying infection. The genital symptoms usually precede the ocular symptoms by a week or two. Rarely, urethritis may be absent due to direct inoculation of the organism into the eye.
- Other potential ocular and systemic complications of gonococcal conjunctivitis include iritis, lid abscess, dacryoadenitis, and septicemia.
- Conjunctival pseudomembranes may be evident.
Acute Conjunctivitis
- The principle causes of acute bacterial conjunctivitis are two Gram-positive organisms, Staphylococcus aureus and Streptococcus pneumoniae, and two Gram-negative bacteria, N. gonorrhoeae and Haemophilus species (Figs. 6-5 and 6-6)
- The typical presentation is a mild to moderate diffuse or segmental, bulbar, and tarsal conjunctival injection with canthal involvement.
- There is usually minimal eyelid involvement and no PA lymphadenopathy, except in very severe cases.
- A papillary conjunctival tissue reaction is common.
- Pseudomembranes or small subconjunctival hemorrhages may be present (Streptococcus and Haemophilus).
- Mucopurulent discharge may be mild to moderate and may seal the eyelids upon awakening.
- The cornea is usually uninvolved; however, a mild, inferior punctate keratitis may be present.

Figure 6-5. Streptococcal bacterial conjunctivitis. Note the purulence in the cul-de-sac.

Figure 6-6. Haemophilus blepharoconjunctivitis in a young child. Note the bluish/purple lid coloration which is common in Haemophilus infection.
Membranous Conjunctivitis
- This disorder has the same clinical presentation as acute conjunctivitis, with the addition of pseudomembranes or membranes and markedly swollen lids.
- Pseudomembranes (fibrinous exudate on the conjunctival surface without deep attachments that can be removed without significant bleeding) in bacterial conjunctivitis are most commonly caused by Neisseria or Streptococcus pyogenes; true membranes (fibrin strands project into the conjunctiva between epithelial cells, causing bleeding when removed) are most often caused by Corynebacterium diphtheriae.
- Pain is a prominent feature of membranous conjunctivitis.
- Any severe bacterial conjunctivitis can cause a pseudomembrane.
- Membranous conjunctivitis may be associated with corneal ulceration and/or permanent loss of goblet cells, which could result in OSDs, palpebral scarring, and chronic dry eye. Palpebral scars may be present as a result of resolved membranes. Viral conjunctivitis is more commonly associated with membranous conjunctivitis.
Chronic Conjunctivitis
- Staphylococcus
- The lids may show signs of crusting and formation of collerettes with associated madarosis and trichiasis. In addition, the skin of the lids may show an eczematous-type reaction. The bulbar conjunctiva may be mildly to moderately injected with or without the presence of phlyctenules. The palpebral conjunctiva usually demonstrates a papillary reaction. The cornea may be involved with inferior punctate keratitis, marginal infiltrates, or micropannus as a result of the presence of bacterial exotoxins. (See Bacterial Blepharitis.)
- Moraxella
- Moraxella may cause mild to moderate papillary conjunctivitis without corneal involvement. It may also result in angular blepharoconjunctivitis (Staphylococcus has also been implicated as a common cause in this presentation). On occasion, Moraxella may cause a chronic follicular conjunctivitis with corneal involvement, including punctate keratitis, subepithelial infiltrates, and preauricular lymphadenopathy. This latter presentation could be confused with adenovirus or chlamydial infections.
Demographics
Hyperacute Conjunctivitis
Hyperacute conjunctivitis can occur in men or women. It is usually associated with venereal disease (i.e., Gonococcal infections). Hyperacute conjunctivitis may be implicated in ophthalmia neonatorum.
Acute Conjunctivitis
Acute conjunctivitis is usually self-limiting in 1 to 3 weeks. It is a less common cause of “pink eye” in the United States, although its presence is not unusual. Streptococcus is the predominate etiology in the northern United States, while Haemophilus aegyptius (Koch-Weeks bacillus) is the leading cause in the southern United States.
Haemophilus influenzae must be considered in any conjunctivitis in young patients, as the ability to make appropriate antibodies for H. influenzae does not exist in children aged 5 and under. However, the H. influenzae type B vaccine has greatly reduced the incidence of this disease.
Membranous Conjunctivitis
Membranous conjunctivitis is rarely caused by C. diphtheriae because of immunizations in the United States.
Chronic Conjunctivitis
Chronic conjunctivitis may occur in men, women, or children and may be the sequelae of an acute infection that received inadequate or inappropriate treatment.
Significant History
Hyperacute Conjunctivitis
History of urethritis or other urogenital involvement may be present. A history of a new sexual partner or of promiscuity is significant. The patient may also have other venereal diseases—there is an especially high frequency of coinfection with chlamydia.
Acute Conjunctivitis
The patient may have a history of an upper respiratory infection or contact with someone with conjunctivitis or an upper respiratory infection. Children at daycare facilities may be more likely to come in contact with pathogens.
Corynebacterium diphtheriae conjunctivitis may be associated with a history of respiratory involvement including airway obstruction with a pharyngeal membrane; exotoxins from C. diphtheriae may result in paralysis of accommodation and extraocular muscles as well as cardiac toxicity and liver necrosis.
S. pyogenes may be associated with chronic low-grade dacryocystitis, which develops into an acute conjunctivitis.
Chronic Conjunctivitis
Chronic conjunctivitis is often associated with blepharitis or past episodes of acute bacterial infection.
Ancillary Tests
In general, the diagnosis of a nonsevere conjunctivitis is made clinically. However, cases of severe bacterial infections mandate further investigation.
Hyperacute Conjunctivitis
- Cytology
PMN response with intracellular bacteria.
- Gram stain
Gram-negative intracellular, diplococci, with many PMNs—Neisseria.
Gram-negative bacilli or coccobacilli—H. influenzae.
- Cultures
Purulent discharge should be streaked on blood and chocolate agar and incubated at 37° in 10% CO2 or on a Thayer-Martin plate. Antibiotic sensitivities should also be performed.
Note: Imaging may be indicated in cases of orbital abscess or advanced cellulitis.
Acute Conjunctivitis
- Cytology
PMN response.
- Gram stain
Presence of bacteria. The clinician should note the morphology of the organism (e.g., rod, club, or cocci) as well as other characteristic features of the organism (e.g., clusters, chains).
- Cultures
Cultures are necessary in persistent infections that do not respond to empiric treatment and should include plating on blood and chocolate agar as well as thioglycolate broth. Antibiotic sensitivities should also be requested.
Membranous Conjunctivitis
- Cytology
PMN response.
- Gram stain
Gram-positive cocci arranged in chains or pairs (S. pyogenes).
Gram-positive pleomorphic rods that appear drumstick shaped (C. diphtheriae).
Gram-negative diplococci (Neisseria).
- Cultures
Beta-hemolysis on blood agar (S. pyogenes).
Loeffler’s blood serum (C. diphtheriae).
Chronic Conjunctivitis
- Cytology
PMN response.
- Gram stain
Gram-positive cocci in clusters (Staphylococcus).
Gram-negative diplobacilli usually arranged in pairs (Moraxella).
- Cultures
Staphylococcus: Blood agar with coagulase testing (S. aureus—positive; S. epidermidis—negative) and mannitol fermentation to differentiate S. aureus from S. epidermidis; sensitivities should be performed because of propensity toward resistance.
Moraxella: Enriched media such as Loeffler’s medium.
Hyperacute Conjunctivitis
- All cases of Neisseria infection must be reported to the Center for Disease Control (CDC)
- Systemic treatment is mandatory in this condition; topical treatment is only adjunctive.
- Hospitalization is not uncommon, especially if keratitis exists.
- The patient and sexual partners must be promptly referred for venereal aspects of N. gonorrheae and coinfection with other sexually transmitted diseases (STDs) such as HIV, syphilis, and/or chlamydia to avoid significant morbidity. Care should be taken to protect patient confidentiality.
1. Topical therapy (inadequate as the only form of treatment).
Warm saline rinses q.i.d. until the discharge has resolved.
Erythromycin, tobramycin, or bacitracin ung q.i.d.
Fluoroquinolones (FQs) (ciprofloxacin, levofloxacin, ofloxacin, moxifloxacin, or gatifloxacin) q2h × 4 to 7 days.
2. Systemic therapy
No keratitis present
ceftriaxone 250 mg to 1g IM or IV as a single dose in adults
Keratitis present
ceftriaxone 1 g IV q12–24h × 3 days or until symptoms subside and there is an appropriate clinical response.
Treatment for a concomitant chlamydial infection includes erythromycin, tetracycline, or sulfacetamide ointment two to three times per day plus:
azithromycin 1 g p.o. (single dose) preferred treatment, or
doxycycline 100 mg b.i.d. p.o. × 1 to 2 weeks
Acute Conjunctivitis
Nonsevere cases of acute conjunctivitis generally subside in 1 to 2 weeks; however, topical antibiotics may accelerate resolution of the infection and reduce the risk of transmission. Empirical treatment without cultures tends to be the rule in therapy.
Besivance (besifloxacini> 0.6%) 1 gtt. t.i.d. for 7 days. or
Zymar (gatifloxacin) 1 gtt. q2h while awake × 2 days and then 1 gtt. q.i.d. days 3 to 7, or
Vigamox (moxifloxacin) 1 gtt. t.i.d. × 4 to 7 days, or
Polytrim (trimethoprim/polymyxin B) 1 gtt. q.i.d. × 7 to 10 days, or
Azasite (azithromycin) 1 gtt. b.i.d. for 2 days and then 1 gtt. q.i.d. for 5 days, or
Consider other antibiotics with similar action,
Ocuflox (ofloxacin) 1 gtt. q.i.d. × 7 to 10 days, or
Ciloxan (ciprofloxcin) 1gtt. q.i.d. × 7 to 10 days or
Tobrex (tobramycin) 1 gtt. q.i.d. × 7 to 10 days (S. pneumo resistance may be a problem), or
Ilotycin (erythromycin ophthalmic) ung b.i.d. × 7 to 10 days. (S. aureus strains have become increasingly resistant to its action.)
Membranous Conjunctivitis
After instillation of a topical anesthetic, remove the membranes with a forceps. Removal can be difficult and results in bleeding.
- C. diphtheriae
C. diphtheriae antitoxin 10,000 to 100,000 units parenterally
Erythromycin, penicillin, or
Clindamycin, or
Topical penicillin (must be compounded by pharmacy)
- S. Pyogenes
Topical: bacitracin or erythromycin ung b.i.d.-q.i.d.
Systemic: penicillin G or V is generally recommended. However, cephalexin or erythromycin 250 mg q6h p.o. × 7 days may be effective.
Note: Topical steroids are often helpful in reducing inflammation and preserving the conjunctiva architecture when added to other treatments.
Chronic Conjunctivitis
- Topical
Lid hygiene with a commercial lid scrub preparation (diluted baby shampoo may be substituted but may be more irritating to the eye). Warm compresses may also facilitate management.
Topical bacitracin, Polysporin, or erythromycin ointment applied to the lids and lashes hs × 3 to 4 weeks and then tapered to a maintenance dose.
Topical antibiotic/steroid gtts may be helpful for bulbar conjunctival and corneal involvement:
Maxitrol drops (neomycin/polymyxin B/dexamethasone) 1 gtt. t.i.d. × 7 to 10 days, or
TobraDex (tobramycin/dexamethasone) 1 gtt. t.i.d. × 7 to 10 days, or
Zylet (loteprednol etabonate 0.5%/ tobramycin) 1 gtt. t.i.d. × 7 to 10 days
Patients who do not respond to therapy may be carriers and require culturing of the nasopharynx, ear canal, and skin, as well as systemic treatment.
- Systemic:
Tetracycline (do not use tetracycline in pregnant women or children under age 8 and be aware of photosensitizing effects of drug) or erythromycin 250 mg q.i.d. p.o. × 2 to 4 months or
Doxycycline or minocycline 50 to 100 mg b.i.d. p.o. × 1 month and then tapered and used for several additional months or
If penicillinase resistant antibiotic is necessary, consider cloxacillin:
Greater than 20 kg—250 mg q6h p.o. × 10 days or
Less than 20 kg—50 mg/kg/d in equally divided doses q6h p.o. × 10 days
Phlyctenulosis
Marcus G. Piccolo and Victor Malinovsky
ICD-9: 370.31
 THE DISEASE
THE DISEASE
Pathophysiology
Phlyctenulosis is an immune reaction of the conjunctiva, limbus, or cornea, most commonly initiated by bacterial proteins that are recognized as antigenic (antigens). The immune reaction is classified as a Type IV delayed hypersensitivity response resulting in a raised nodule and localized perivascular inflammation. The nodule may necrose and ulcerate, further amplifying the resultant inflammatory response.
Etiology
Phlyctenulosis is the result of systemic or local infection by a pathogen that acts as an antigen in the eye. Although the antigen is usually bacterial protein, other pathogens have also been responsible for initiating a phlyctenular response, including virus, fungus, chlamydia, and nematodes.
The organisms most likely to cause a phlyctenular response are tubercle bacillus and Staphylococcus spp. Classically, systemic tuberculosis (TB) was implicated as the primary cause. More recently, hypersensitivity to Staphylococcus spp., associated with bacterial blepharitis, has been a more common presentation. Other less common pathogens include Coccidioides immitis, Candida albicans, Chlamydia spp., H. aegyptius, herpes simplex virus (HSV), and various nematodes.
The Patient
Clinical Symptoms
Patients presenting with phlyctenulosis often experience discomfort or pain (especially if the phlyctenule is limbal or corneal), photophobia, tearing, and irritation.
Clinical Signs
Phlyctenulosis typically causes a red irritated eye. The phlyctenule itself is a small (1 to 3 mm) elevated nodule. The nodule is usually yellow, gray, or pinkish-white in color and can be found on the bulbar conjunctiva, at the limbus (the most common location), or on the cornea (Fig. 6-7). The lesion is frequently inflamed and surrounded by dilated vessels. On rare occasion, a phlyctenule can be found on the tarsal conjunctiva.
Figure 6-7. Phlyctenulosis secondary to bacterial blepharitis in a 12-year-old Hispanic female. Note the elevated lesions at the limbus.
Limbal phlyctenules typically have a more triangular shape with the apex toward the cornea. It is common for the nodule to ulcerate, in which case it will stain with fluorescein. In most cases, the nodule will appear, necrose, and then subside within 14 days. However, it is possible for the phlyctenule to persist and to recur.
Phlyctenules on the conjunctiva typically do not scar; however, limbal and especially corneal phlyctenules often result in scarring. A peripheral corneal phlyctenule may advance onto the cornea. In so doing, a leash of vessels will typically trail behind the nodule, creating a superficial fibrous vascular bundle with an underlying infiltrate. This fibrovascular response has the potential to cause significant visual impairment and may ultimately require a corneal graft. Past episodes of limbal phlyctenules may be visible by identifying triangle shaped scars at the limbus with pannus formation.
Demographics
Phlyctenulosis most commonly affects children and young adults, with a slight predilection for females. Populations that have a higher prevalence of TB may be more at risk. This systemic factor is greater in many third world countries where TB is endemic, as well as some locations within the United States that are inhabited by large third world populations. Although TB has historically been a prominent cause of phlyctenulosis, most authorities agree that the major cause of phlyctenulosis in the United States is secondary to staphylococcal blepharitis.
Significant History
A history of chronic lid infection/inflammation is significant for the presence of bacterial blepharitis and should be investigated as an etiology for phlyctenulosis.
A history of chronic cough or close contact with others who may have TB is important.
Ancillary Tests
Laboratory studies should focus on known etiologies, including a PPD skin test for TB, QuantiFERON-TB Gold (QFT-G) and tests to rule out other less common causes.
In recalcitrant cases, cultures (and sensitivities) of the lids and lashes may prove beneficial.
The Treatment
Treatment may require duel modalities. First, underlying infective diseases must be controlled. In the case of TB, or other less common etiologies, appropriate systemic therapy should be initiated. Bacterial blepharitis, if present, should be addressed with lid hygiene and appropriate topical antibiotics. Both bacterial blepharitis and chlamydial infections are discussed elsewhere in this text.
The specific treatment for phlyctenulosis is topical steroid therapy. A course of topical steroids will quickly cause the nodule and symptoms to abate, usually within 5 to 7 days.
Prednisolone acetate, 1% suspension q.i.d. × 5 to 10 days, is in most cases, sufficient to relieve symptoms and signs. Concomitant use of topical antibiotics is appropriate while steroid drops are used. A combination drug such as TobraDex (tobramycin/dexamethasone) or Zylet (tobramycin/loteprednol etabonate 0.5%) could also be used q.i.d. × 5 to 10 days.
Recurrences are not uncommon and should be treated aggressively, especially when corneal involvement is present.
Bacterial Keratitis
BACTERIAL INFECTIOUS CORNEAL INFILTRATES AND BACTERIAL CORNEAL ULCERS
Nicky R. Holdeman
ICD-9: 370.01, ICD-9: 370.03
 THE DISEASE
THE DISEASE
Pathophysiology
Bacterial keratitis is a potentially sight-threatening infection of the cornea and a major public health burden. A wide range of pathogens have been implicated; however, the lid margins provide a common source of bacteria that may, under the right conditions, invade the cornea. The severity of the condition and the complications incurred depend on the infectious agent, the production of toxins and enzymes by the organism, and the inflammatory response of the host. Vision compromise may occur by corneal scarring, by the development of glaucoma and cataracts, or by loss of the eye following corneal perforation.
Etiology
Bacterial infections of the cornea may be produced by a number of microorganisms. While regional variations within the United States may exist, the most common pathogens cultured from cases of bacterial keratitis include S. aureus (Fig. 6-8), S. epidermidis, Streptococcus viridans, S. pneumoniae, Pseudomonas aeruginosa (Fig. 6-9), and species of Moraxella, P. acnes, Klebsiella, Proteus, Serratia, Hemophilus, and Neisseria. A clinically significant number of cases are polymicrobial in nature.
Figure 6-8. Staphylococcus aureus keratitis.
Figure 6-9. Pseudomonas aeruginosa keratitis with surrounding infiltrate and hypopyon.
Up to 70% of contact lens–related microbial keratitis is due to P. aeruginosa; however, there is also a possibility of a mycotic process in these patients.
Methicillin-resistant S. aureus (MRSA) and methicillin-resistant S. epidermis (MRSE) is a growing concern but is not the No. 1 cause of keratitis. However, MRSA and MRSE has emerged as the most common infection occurring following anterior segment surgery, including cataract surgery, LASIK, and surface ablation procedures. Studies suggest that LASIK has a lower risk of postoperative infection than do PRK procedures and that fewer infections result from use of a femtosecond laser compared with microkeratome flaps.
Note: Microbial invasion of the cornea typically involves adherence of the bacteria to injured or compromised corneal tissue. Several species of bacteria, however, have been noted to penetrate intact corneal epithelia, including N. gonnorrhoeae, Neisseria meningitides, C. diphtheriae, H. influenzae, Listeria monocytogenes, and Shigella.
The Patient
Clinical Symptoms
- Conjunctival injection
- Pain or foreign body sensation
- Decreased visual acuity
- Photophobia
- Discharge
Clinical Signs
An infectious keratitis is often accompanied by
- Lid and conjunctival edema and hyperemia
- Purulent or mucopurulent discharge
- Anterior chamber inflammation (with or without hypopyon)
- Papillary conjunctival response
A bacterial corneal ulcer is present when an infectious infiltrate is associated with necrosis and loss of epithelial or stromal tissue.
- The ulcerated defect may have well demarcated borders with an ill-defined dense, gray stromal infiltrate and underlying endothelial plaque
- WBC infiltration and edema may extend well beyond the epithelial defect
Contact lens associated corneal infiltrates, including asymptomatic ones, should be considered infectious until proven otherwise. However, in general, an infectious infiltrate typically has the following features:
- Overlying epithelial defect that stains with sodium fluorescein
- Anterior to midstromal location that is light blocking
- Diffuse appearance with poorly defined borders
- No clear zone between the infiltrate and the limbus in peripheral lesions
- Greater than 2 mm in diameter
- Pain
- Anterior chamber reaction
The patient should be quickly assessed as to whether the keratitis is potentially sight threatening, including a history or clinical features suggesting a fungal, amoebic, mycobacterial, or drug-resistant organism. Bacterial ulcers may progress to corneal perforation within 24 hours if not properly identified and treated. Any of the following characteristics is highly suggestive of a serious, sight threatening infection:
- AC response of 1+ or more (>10 cells/1 mm beam)
- Infiltrate is greater than 2mm in size or extends into deep stroma
- Infiltrate is less than 3mm from the visual axis
- The condition is worse (signs and symptoms have not improved) after 24 hours of empiric therapy.
Note: In addition to the characteristics listed above, several features have been identified in which a microbial keratitis often leads to a poorer prognosis or results in a higher incidence of penetrating keratoplasty. These risk factors may serve as indicators for primary treatment failures and identify patients who may require intensive, tertiary care.
- The patient is 60 years of age or older
- Central location or limbal involvement of the ulcer
- Past ocular surgery, including LASIK
- Poor visual acuity at presentation
- Large ulcer (>5 mm), stromal thinning, and/or hypopyon
- Previous treatment with a topical steroid
- Delay in treatment or delay in referral (>7 days) to a corneal specialist
The patient should also be examined and monitored for secondary manifestations of inflammation, including
- Synechiae formation
- Elevated IOP
- Cataracts
- Progressive corneal thinning/perforation
- Scarring
Demographics
Approximately 30,000 cases of bacterial keratitis occur annually in the United States.
Corneal opacification and perforation from bacterial keratitis result in approximately 330 corneal transplants a year in the United States.
Bacterial keratitis may affect anyone at any age; however, the risk of infection increases with loss of the cornea’s barrier function and/or chemical defenses of the tear film. For example, the overnight use of contact lenses greatly increases the risk of corneal ulceration. Virtually, every CL wearer has occasional ocular surface defects caused by mechanical abrasion or hypoxia of underlying epithelial cells.
The incidence of infection is also higher in patients with other risk factors such as
- Neuroparalytic keratopathy
- Keratitis sicca
- Blepharitis
- Defective immune system (local or systemic immune deficiency)
- Alcohol or injectable drug abuse
- Vitamin deficiency
- Epithelial compromise, including trauma
- Diseases that compromise ocular wound healing (i.e.,) diabetes mellitus, rheumatoid arthritis, atopic dermatitis, ocular cicatricial pemphigoid
Significant History (Also See Risk Factors Above)
- Soft contact lens use (especially extended wear)
- Past ocular surgery (suture abscess, bleb infection)
- Systemic immunosuppression (acquired or iatrogenic)
- Malnutrition
- Bell’s palsy
- Topical steroid use (local immunosuppression)
- Epithelial defects (trauma, erosions, or corneal dystrophies such as ABMD)
- Recent exposure to a medical or hospital environment (inpatient, nurse, employee, etc.), athletes who participate in contact sports or frequent gyms, patients in nursing homes, contact with a correctional facility (prisoner or visitor), individuals with recurrent skin or soft tissue infection, or patients with a history of dialysis. These patients all have an increased risk of being hospital acquired or community acquired MRSA carriers.
- Use of long term antibiotics
- Multiple use of unit-dose preservative-free artificial tears
Ancillary Tests
When infection occurs, it is wise to presume the involvement of resistant organisms. The growing frequency of drug resistance among corneal isolates has reinforced the need for combined therapy guided by the results of laboratory cultures. Consequently, microbiologic studies (stains and cultures) of the cornea, and possibly the lids and the conjunctiva, are essential any time a sight threatening infectious keratitis is suspected (see above). One should also consider culturing (1) a patient with a significant decrease in vision, (2) a post surgical eye, (3) a monocular patient, (4) a diabetic or immunocompromised patient, or (5) a patient who works in a health care setting.
A clinically significant number of eyes with bacterial keratitis do not respond to empirically selected therapy and poor antibiotic sensitivity correlates with a larger corneal scar after resolution of a corneal ulcer. Culturing and sensitivity testing at the time of presentation will help to confirm the diagnosis and facilitate appropriate modification of treatment.
Stains (Routine)
- Gram stain—demonstrates bacteria and yeasts
- Giemsa stain—demonstrates fungal and viral elements
Note: Stains analyzed by a general microbiology lab will often have less diagnostic value than when interpreted by an experienced ophthalmic microbiology technician. Slides fixed by immersing in methanol can be used for special stains if required later.
Microbiologic Media (Routine)
- Blood agar—supports most aerobic bacteria and fungal organisms; will not support Haemophilus; poorly grows Neisseria
- Chocolate agar—supports most bacteria, including Haemophilus and Neisseria; does not provide information on alpha or beta-hemolysis
- Sabouraud’s agar (without cyclohexamide)—supports fungal pathogens while inhibiting bacterial growth
- Thioglycolate broth—used to isolate anaerobic bacteria and to saturate swabs prior to plating blood and chocolate agar
In contact lens associated ulcers, the patients’ lenses, solutions, and case should also be cultured, especially if the corneal cultures reveal no growth and the patient is not improving.
Note: One can expect a positive corneal culture to be obtained in approximately 50% to 60% of cases. Percentages may be increased by using nonpreserved topical anesthetics and proper culture techniques in patients with an adequate inoculum.
The Amies transport medium (without charcoal) may be a useful alternative to direct inoculation onto blood agar; however, this author recommends direct plating onto appropriate media whenever possible.
Corneal biopsy and/or polymerase chain reaction (PCR) analysis may be indicated when conventional cultures have not identified an organism and the infection has not responded to broad-spectrum antibiotics. While availability varies, PCR has shown to detect microbial DNA and to identify pathogenic organisms in a high proportion of culture negative cases.
Real-time PCR assay, such as Cycleave PCR, has been shown to simultaneously detect bacterial and fungal pathogens in patients with corneal ulcers. These tests are rapid (about 2 hours versus 48 hours for culture results) and may identify an infectious organism in culture negative cases. Future testing may involve an in-office diagnostic kit for pathogen-specific detection.
While not readily accessible to the majority of practitioners, confocal microscopy is a rapid, noninvasive tool and may be helpful in excluding fungal or Acanthamoeba-like structures in cases with negative bacteriologic results.
In addition, the parameters measured by anterior segment OCT can be useful in quantifying the response to treatment of infectious corneal ulcers.
The Treatment
Bacterial cytopathic effects and the host inflammatory response both contribute to corneal damage associated with bacterial keratitis. Thus, the basic principles in the treatment of bacterial keratitis is to rapidly eradicate the affected tissue of infectious organisms, to limit the structural damage caused by the infectious/inflammatory process, and to taper therapy appropriately in order not to impede healing.
The cornea is best treated by the frequent application of bactericidal concentrations of topical antibiotics in conjunction with ancillary therapy. Patients should be followed on a daily basis until clinical improvement has been demonstrated.
Treatment of infectious infiltrates and infectious ulcers typically involves
- Cycloplegics (5% homatropine, 1% atropine, or 0.25% scopolamine) b.i.d.–t.i.d. depending on the level of inflammation
- Topical antibiotics—Initial antibiotic selection should be based on the organisms demonstrated by the Gram and Giemsa stains, severity of the infection, risk factors, likely pathogens, and clinical impression. In cases of serious keratitis, it is best to treat with multiple broad spectrum antibiotics until the organism and sensitivity patterns are identified by culture. Depending on size, location, and severity, treatment may involve fortified and/or commercially prepared antibiotics:
1. Fortified antibiotics—For sight threatening infections, many external disease specialists have advocated the use of tobramycin (9.1 or 14 mg/mL) q15–60min, alternating with cefazolin (50 mg/mL) q15–60min around the clock and then tapering with clinical response. This combination is a common and well evaluated regimen and is preceded by a loading dose of one drop every 5 to 15 minutes during the first hour. However, there have been reports of some resistance to the aminoglycosides and to cefazolin. Retrospective studies have suggested the use of fortified vancomycin (25 to 50 mg/mL) alternating with ceftazidime (50 mg/mL). This latter combination typically covers MRSA and difficult Gram-negative bacteria, but the use of vancomycin and ceftazidime is limited due to the expense of these drugs and severe stinging on instillation. Consequently, the aminoglycosides and cefazolin are still considered by some as the mainstay of fortified antibiotic therapy in sight threatening infections (Table 6-3). Unfortunately, fortified antibiotics are not readily available in all areas, are slower acting, have variable corneal penetration, require refrigeration, and are more cytotoxic to the cornea when compared to the topical FQs.
2. Commercial antibiotics—Ciprofloxacin (Ciloxan), ofloxacin (Ocuflox) and levofloxacin (Iquix) have FDA approval for monotherapy treatment of bacterial keratitis. However, it is evident that there has been increasing development of bacterial resistance to FQs since their introduction.
TABLE 6-3 Formulation of Fortified Antibiotics
Note: Fortified antibiotics should be refrigerated and shaken before each use. In general, they are good for 4 to 7 days after reconstitution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


