and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
6.1 Facial Artery Musculomucosal (FAMM) Flap

Fig. 6.1
The airway is secured by nasal intubation. With the patient in supine position and the head extended, the face and head is prepared. The anterior incision lies 1 cm posterior to the oral commissure. The orifice of the parotid duct marks the posterior limit of the flap
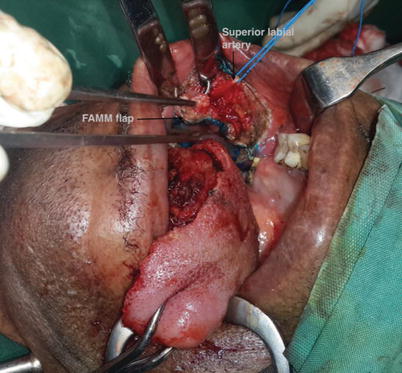
Fig. 6.2
When incising the anterior border of the flap, the superior labial artery is identified. It is ligated and by following its proximal course, the facial artery is identified
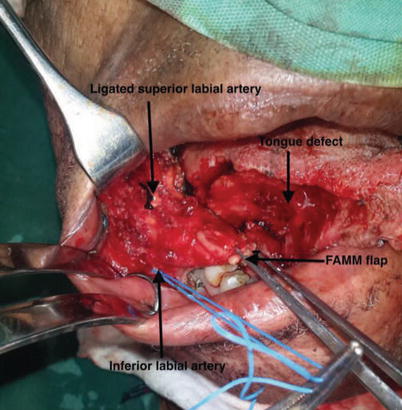
Fig. 6.3
The flap is elevated in the layer underneath the facial artery including the overlying buccinators muscle and a small portion of the orbicularis oris muscle close to the oral commissure. The inferior labial artery is identified and ligated
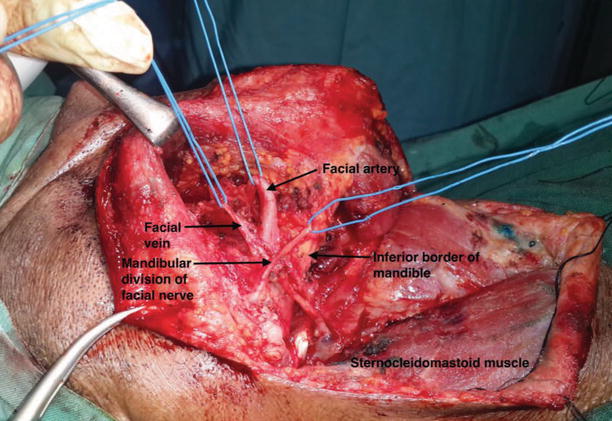
Fig. 6.4
Dissection is continued underneath the facial artery to the neck over the mandible. The flap is completely mobilized from the neck with the facial artery and vein in view
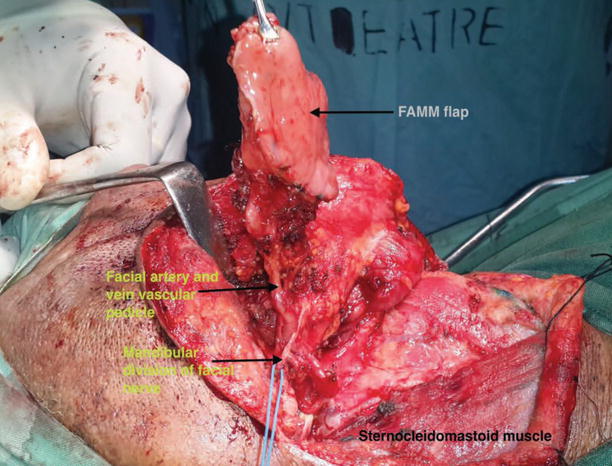
Fig. 6.5
The flap is mobilized to the neck with its vascular pedicle
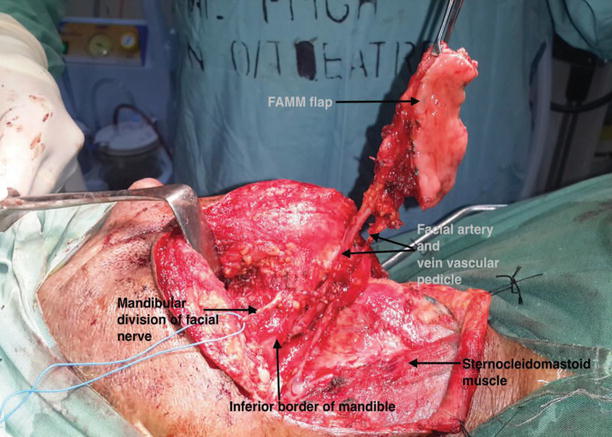
Fig. 6.6
The mandibular division of the facial nerve which runs over the facial artery and vein is dissected and preserved. The flap with its vascular pedicle is passed under the nerve to the neck
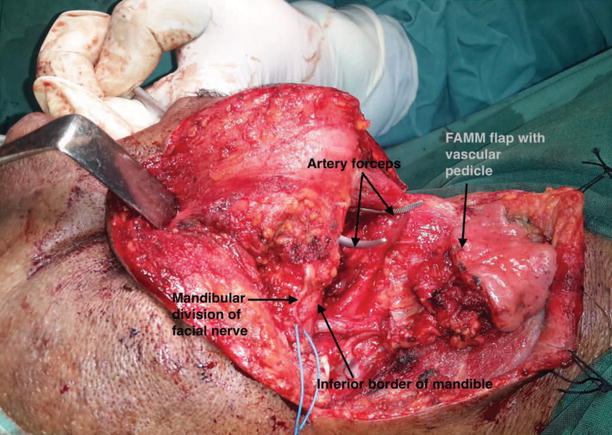
Fig. 6.7
With artery forceps, a tunnel is created communicating the floor of mouth and neck
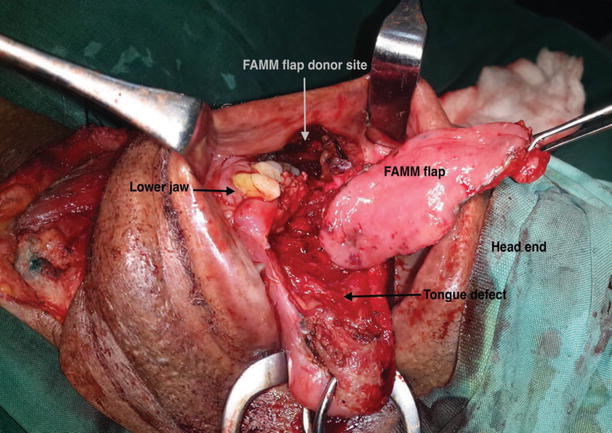
Fig. 6.8
The flap is mobilized to the oral cavity
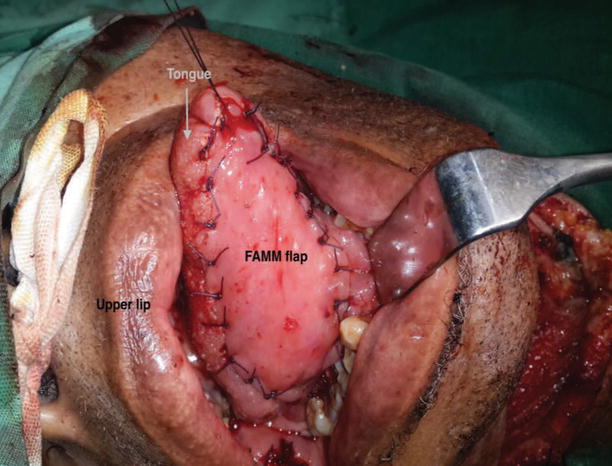
Fig. 6.9
The defect is closed with interrupted sutures

Fig. 6.10
The flap 6 weeks after operation
6.2 Palatal Flap

Fig. 6.11
The patient is intubated with endotrachal tube in the midline and patient is placed in head extended position. The flap marked is out with interrupted diathermy point
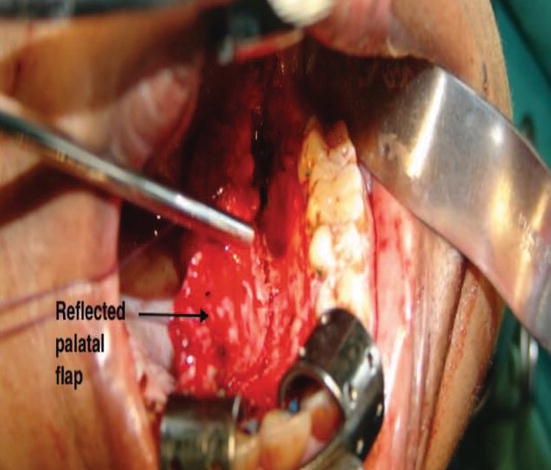
Fig. 6.12
The palatal mucoperiosteal flap is elevated from the bony hard palate in the anteroposterior direction by blunt and sharp dissection from nonpedicle to the vascular pedicle side
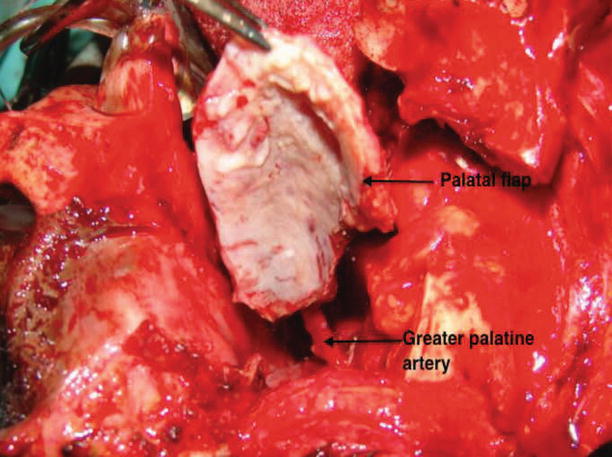
Fig. 6.13
The posteromedial part of the greater palatine canal is drilled under microscope. This freed up the greater palatine vascular pedicle and flap becomes rotatable
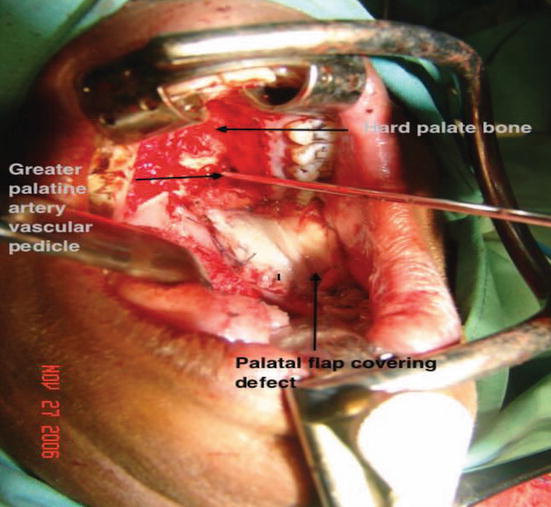
Fig. 6.14
The flap is rotated to resurface the mucosal defect which was located in the retromolar trigone, posterior part of the inferior alveolus and adjoining part of the floor of mouth
6.3 Submental Artery Flap

Fig. 6.15
With the patient in supine position and head extended, the face and head are prepared. The upper limit of the flap is marked along the mandibular arch in the submental region from the ipsilateral angle to a contralateral point across the midline. The inferior limit of the flap is outlined by an index finger-thumb pinch test to assess primary closure

Fig. 6.16
The flap is elevated from the contralateral side of the pedicle in the subplatysmal plane. When dissecting the upper margin of the flap, the marginal mandibular branch of the facial nerve which lies just deep to the platysma and overlying the facial artery is identified and preserved. The dissection is continued till the midline is reached
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


