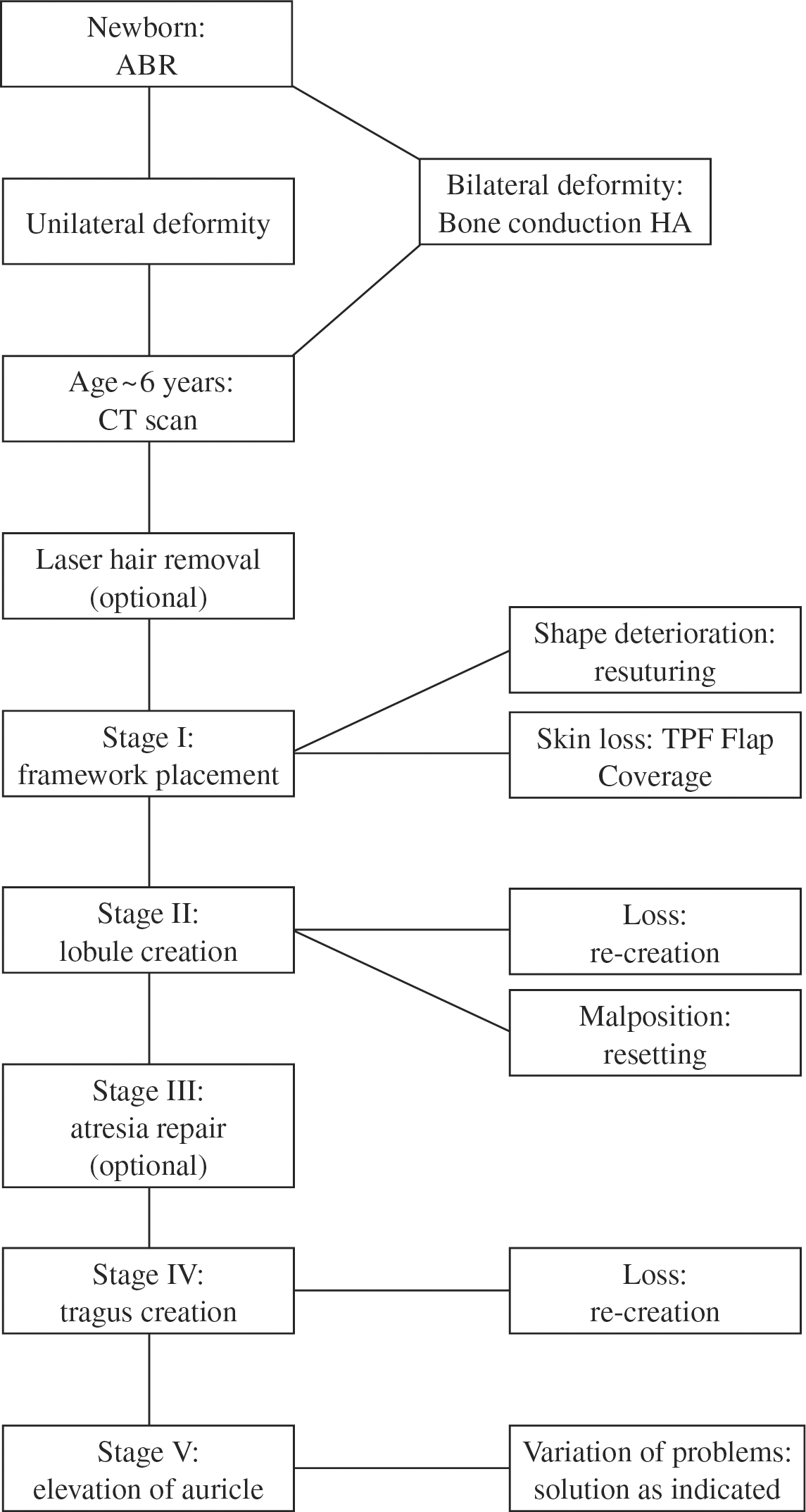
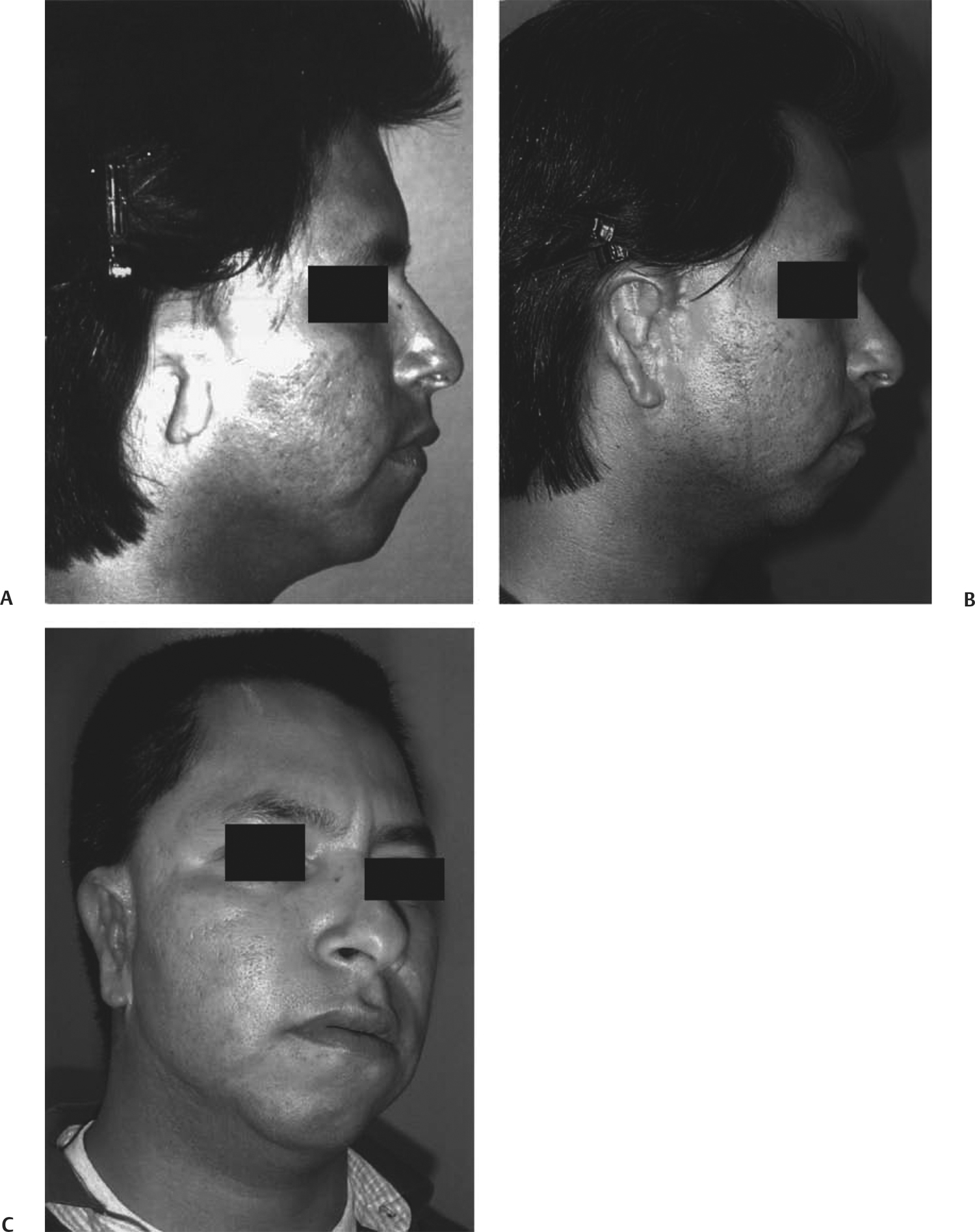
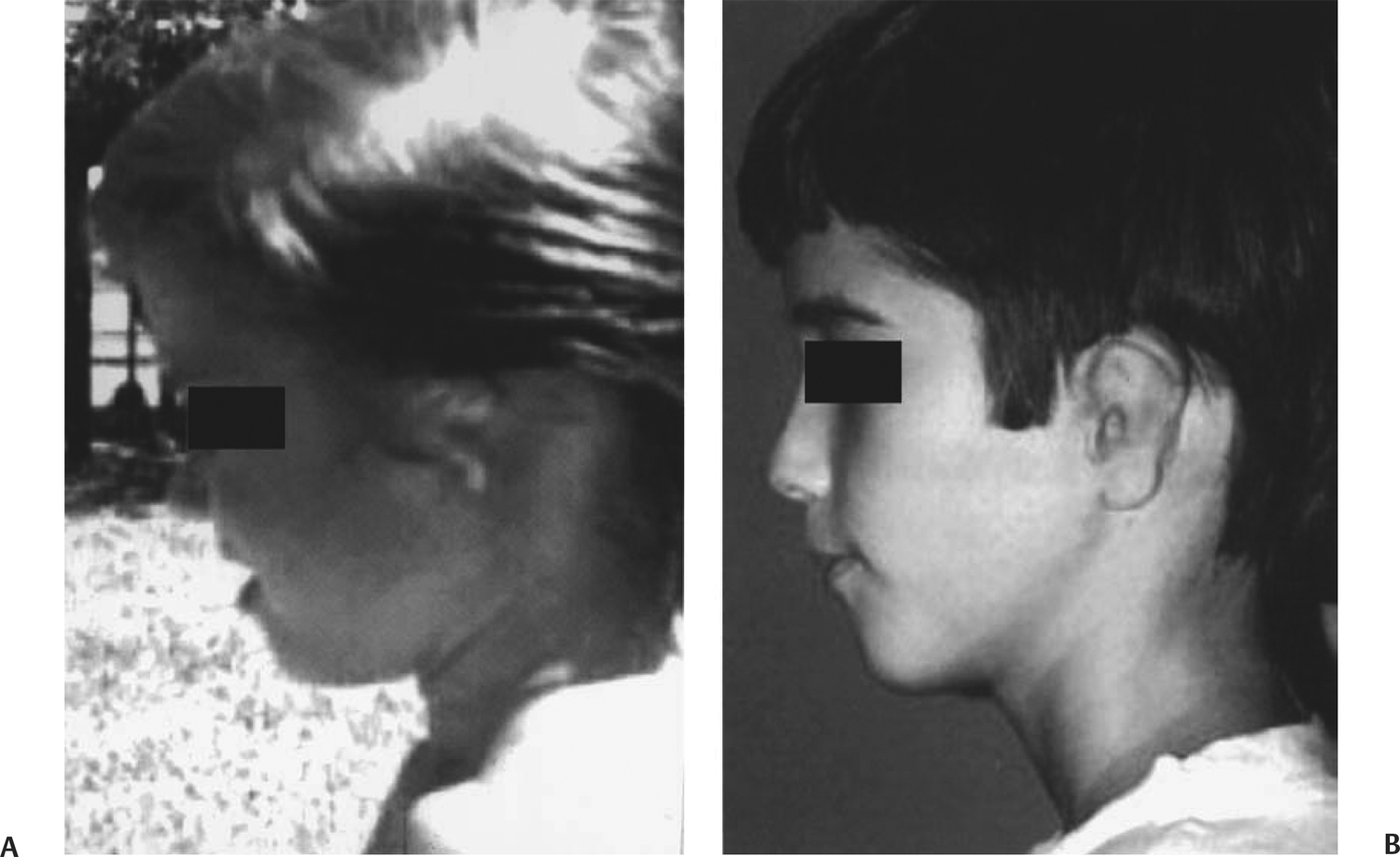
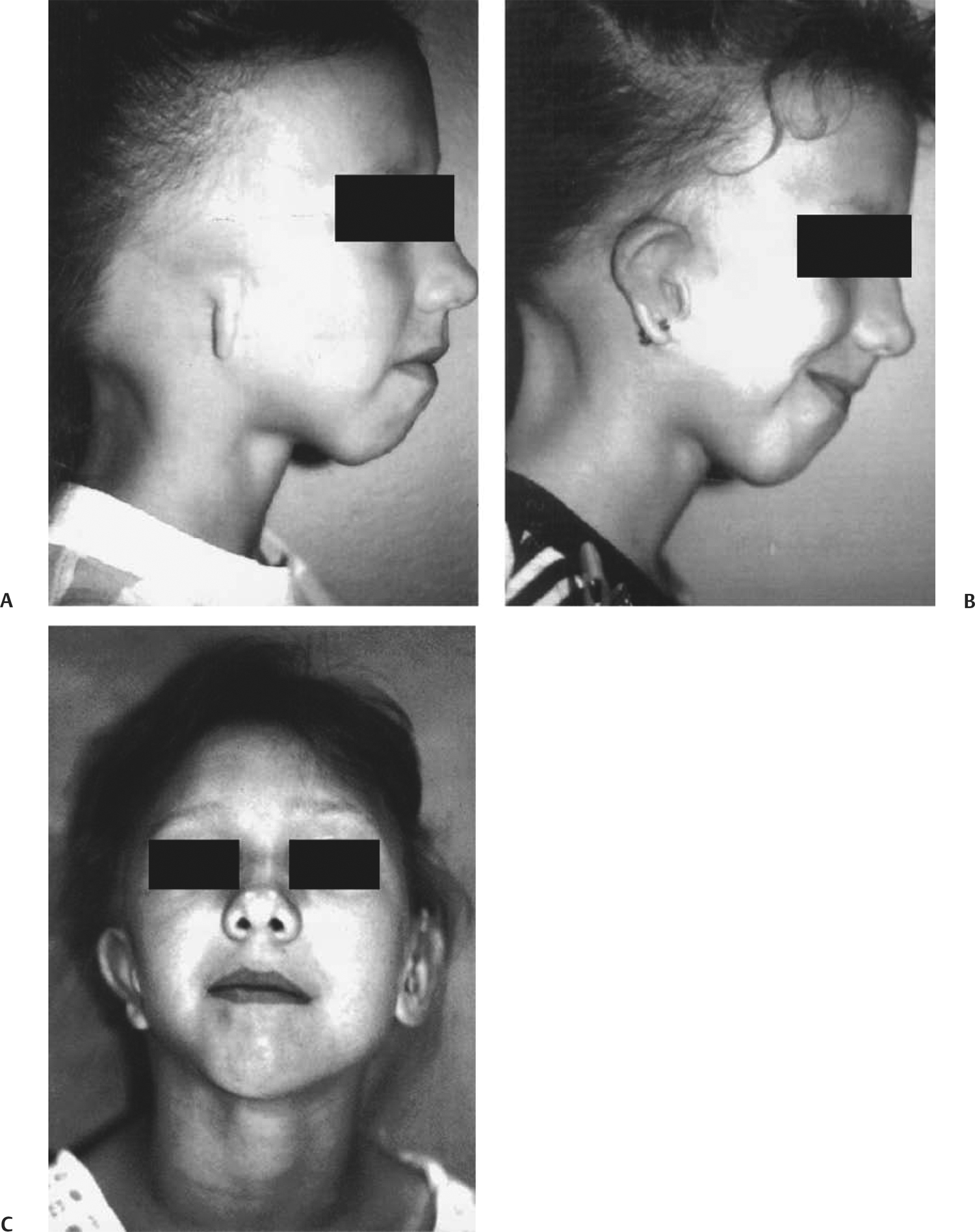
36 Auricular Reconstruction, Revision, and Salvage Since the advent of autologous cartilage for use in the repair of congenital microtias, numerous authors have published their results and recommendations for managing this deformity. Brent’s publication detailing 1200 cases serves as the gold standard for all surgeons.1–3 The need for this repair continues, as the incidence of this condition is not lessening and remains at 1 in 6000 births. Aguilar published the Integrated Auricular Reconstruction Protocol (IARP), which encourages plastic surgeons to consider the repair of the aural atresia (that usually accompanies this condition) as an integral part of the staged reconstruction.3 In this protocol, the individual stages correspond to fixed procedures, and our descriptions of these stages remain constant. Stage III is the correction of the aural atresia; this stage may not be done in all patients. In this protocol, stage IV is tragal reconstruction, and stage V represents auricular elevation. This chapter will focus on eight cases that represent individuals presenting with congenital mocrotiz/atresia in a variety of age groups with standard and unusual considerations. The discussion that follows specifies issues concerning surgical timing, materials, drains and dressings, hairline, atresia repair, and problem areas associated with this type of reconstruction, as well as complications associated with revision surgery. This 29-year-old Hispanic male patient finally sought treatment after many years of ridicule and embarrassment (Fig. 36.1). Stage I reconstruction with rib cartilage graft was accomplished on October 7, 1998. The cartilaginous framework was larger and thicker than standard, measuring 6.5 cm long, 3.5 cm wide, and 20.0 mm high. The procedure was tolerated well without tissue necrosis, and a second procedure to transfer the lobule was accomplished on February 9, 1999. A computed tomography (CT) scan of the temporal bones determined that he was not a candidate for atresia repair due to a congenital absence of the ossicular chain. Therefore, a stage IV reconstruction, or creation of the tragus, was performed on May 5, 1999. Following this procedure, the patient developed an infection, causing resorption of the cartilage graft. This was subsequently revised on December 4, 2000. The elevation, stage V, was completed on October 10, 2000. This patient had been followed since birth for a bilateral complete aural atresia with a grade III microtia of the left ear and a grade II microtia of the right (Fig. 36.2). He was fitted with a bone-conducted hearing aid, and reconstruction was begun at age 5. Preoperative CT scans showed the patient to be a good candidate for atresia repair on the right, more completely formed ear and a marginal candidate on the left. Stage I reconstruction was done on the left ear on December 16, 1994, with framework measuring 5.0 cm long, 2.8 cm wide, and 15.0 mm high. Stage II was accomplished on the left in conjunction with atresia repair on the right ear by the otologist. A later hearing test confirmed a 20 dB speech reception threshold with a 96% speech discrimination score. The remaining two stages were completed by December 27, 1996. Photographs taken during subsequent follow-up visits showed no resorption of cartilage graft and hearing in the normal/near-normal range without benefit of a hearing aid. This patient is a 6-year-old white female with an almost complete anotia of the right ear with a severe hemifacial microsomia (Fig. 36.3). Preoperative CT scans determined that she was not a candidate for atresia repair due to malposition of the facial nerve and malformation of the ossicular chain. External reconstruction was begun on July 8, 1992, and the appropriate stages were completed on July 12, 1993. Note the addition of pierced earrings following the final procedure. This patient also had mandibular distraction. Fig. 36.1 Case 1. A 29-year-old male. (A) Preoperative photograph. (B) The postoperative photograph shows an early result following stage V. (C) Note the change in hairstyle following full reconstruction. Fig. 36.2 Case 2. (A) Preoperative photograph of left grade III microtia/atresia. (B) Postoperative photograph taken 4 years after reconstruction. The patient was not a candidate for atresia repair on the left. This 6-year-old Asian male had a unilateral microtia with atresia of the right ear (Fig. 36.4). Reconstruction was begun on September 8, 1993, with the standard rib cartilage graft. Preoperative CT scans showed the patient to have a fused malleus/incus head and an incus that was two thirds of the normal size. Atresia repair was performed on February 9, 1994, and hearing was improved to normal range. All procedures were accomplished on June 16, 1994. This Hispanic male patient presented at age 13, when the family was advised that surgical reconstruction was possible (Fig. 36.5). A stage I procedure was performed on August 8, 1988, with a framework measuring 5.1 cm long, 3.2 cm wide, and 13.0 mm high. Transfer of the lobule was performed December 13, 1988. Preoperative CT scans showed satisfactory structures for the atresia repair, done on July 19, 1989. Postoperative speech reception threshold was improved to 15 dB with a speech discrimination score of 92%. All procedures were completed by December 13, 1991. Photographs taken 10 years following reconstruction showed no resorption of cartilage framework. This patient continues to have normal hearing, is married, and has a 6-year-old son with normal ears. This is a 6-year-old white female with a left microtia/atresia (Fig. 36.6). Staged reconstruction was begun on June 16, 1998, with a cartilaginous framework. All procedures were completed by June 2, 1999. This 32-year-old Hispanic female presented due to peer pressure and a desire to wear her hair in current fashion (Fig. 36.7). She also stated that she always had extreme difficulty with sound location and hearing when in crowds or on the telephone, which her job required. Stage I was performed on May 22, 1998, with framework measuring 5.2 cm long, 3.5 cm wide, and 14.0 mm high. The lobule was transferred on July 24, 1998, and later revised on September 17, 1998, due to migration of the pedicle flap off the lower end of the thicker framework necessary in adult rib. The preoperative CT scans showed the patient to be a good candidate for atresia repair. All procedures were accomplished when the patient requested ear piercing on March 22, 2001. Fig. 36.3 Case 3. (A)
Case Studies
Case 1
Case 2
Case 3
Case 4
Case 5
Case 6
Case 7
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
