Fig. 3.1
Drawings made by the patient of the images seen during the episodes. Here the drawing represents the start of the episode in the central part
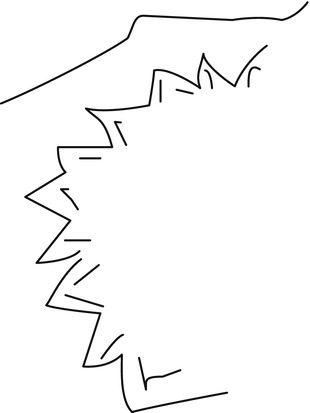
Fig. 3.2
The fortification spectra
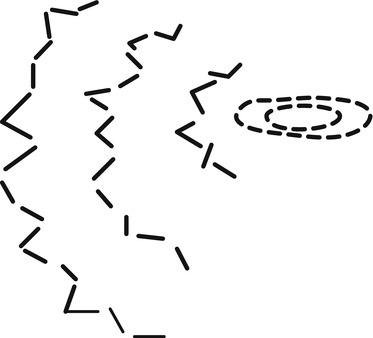
Fig. 3.3
Lights moving from the central to periphery of the visual field in intervals of around 5 min
3.2 Differential Diagnosis and How to Work Up This Type of Patient
This patient reports acute and recurrent episodes of transient neurological deficit. Given the age of the patient (i.e., >50 years), vascular etiology is the first to consider. The history of high blood pressure as a vascular risk factor is also in favor of this etiology.
The most common cause of sudden loss of vision in an older patient is amaurosis fugax, which is a sudden transient, partial, or total loss of vision of any cause; it comes from the Greek amaurosis, meaning dark and the Latin fugax, meaning fleeting. Although the term is related to vascular origin, it may be associated with a heterogeneous group of disorders. The origin can be vascular (embolic or hypoperfusion), ocular, neurological, or idiopathic. The clinician’s goal must be to determine the underlying cause of the patient’s transient visual disturbances.
In a historical series of 186 subjects reporting onset of a sudden visual deficit (not necessarily transient), the evaluation determined the underlying cause to be stroke or transient ischemic attack (24 %), ocular disease (17 %), transient monocular blindness (10 %), and migraine (14 %). The cause remained unknown in 22 %, with a miscellany of causes comprising the remaining 12 %.
In a more recent study of 337 prospectively studied patients with sudden, transient monocular loss of vision, 159 had a normal internal carotid artery (ICA) on the relevant side, 33 had a stenosis between 0 and 69 %, 100 had a stenosis of 70–99 %, and 45 had an ICA occlusion.
Some patterns of clinical presentation can suggest carotid disease, such as an altitudinal onset or disappearance of symptoms. A severe (70–99 %) stenosis has been associated with a duration of between 1 and 10 min, and with a speed of onset in seconds. ICA occlusion has been associated with attacks being provoked by bright light, an altitudinal onset, and the occurrence of more than ten attacks. The frequent repetition of these events in a short period of time could be suggestive of an impending brain infarct. Ischemic problems are usually associated with negative visual phenomena. On examination of the fundi the intravascular retinal emboli were visualized in some cases.
Age older than 50 years and the presence of vascular risk factors, such as hypertension, diabetes, or hypercholesterolemia, are also indicative of an ischemic origin of the problem.
Temporal arteritis, or giant cell arteritis, is another condition that can produce episodes of amaurosis fugax, especially in patients older than 60 years. This is a type of vasculitis whereby the vessels more often involved are the arteries of the scalp and head, especially the arteries over the temples. Giant cell arteritis can cause swelling and thickening of the small artery under the skin; the temporal artery becomes very sensitive and painful to palpation of the skull. The most common symptom is a headache around the temples or in another location, and general symptoms such as fatigue, loss of appetite, weight loss, or a flu-like feeling. Pain in the jaw with chewing is also common. The visual phenomenon is negative, and the duration of the clinical presentation is from weeks to a few months.
The list of “ocular” causes of amaurosis fugax is long. Blepharitis, dry eye syndrome, keratitis, glaucoma, optic disc drusen, vitreous detachment, retinal break, orbital or intraocular tumor, or vasospasm can produce these visual symptoms. The external signs of inflammation can help the diagnosis in blepharitis or keratitis. The symptoms are monocular and the duration of the visual disturbances can be very brief (i.e., seconds), such as in retinal breaks or vitreous traction. The patients describe negative and positive symptoms, which can worsen with eye movements or when the patient is blinking or rubbing the eyes.
Visual disturbances of neurological origin may appear, derived from lesions from the optic nerve to the occipital lobe. Optic neuritis, papilledema, or increase in intracranial pressure can also produce amaurosis fugax.
Occipital and temporoparietal arteriovenous malformations can cause a variety of visual disturbances and headaches. The most typical symptoms are homonymous visual disturbances, headache, seizures, and hemorrhage. A symptomatic migraine with typical aura may be the only clinical manifestation.
Epilepsy, especially occipital seizures, usually begins with visual hallucinations such as flickering or colored lights, rapid blinking, or other symptoms such as eye movements, pallinopsia, or eye pain. The visual symptoms are usually complex, with metamorphoses and stereotyping, sometimes with associated headache. The initiation usually is acute and the duration short (minutes). Seizures are sometimes triggered by visual stimuli, such as seeing flashing lights or a repeating pattern.
Migraine aura is the name given to the many types of neurological symptoms that may occur just before or during a migraine headache. Said to be experienced by 20–25 % of individuals, aura is a fully reversible neurological syndrome, which can develop over 5 min and last for up to 2 h. Usually the aura is associated with headache, but in some cases is the only clinical manifestation.
Occasionally patients in the stroke population older than 40 years have unexplained transient focal neurological events in association with normal neuroimaging. Some authors describe late-life migraine accompaniments that are not uncommon in older populations. In this group the visual symptoms are the most frequent, and fulfill the criteria of migraine aura in a significant number of cases.
In performing the differential diagnosis, the most important tool is the clinical history. The way the episodes started, progression, presence of positive and negative symptoms, duration, worsening with movement, or possible precipitating factors give an initial indication of the etiology. It is also necessary to perform a full neurological examination (including fundi), cranial palpation, and neurovascular examination.
If an ocular origin is suspected, the patient should be referred to the ophthalmologist for a thorough examination. Laboratory testing must be part of the initial diagnostic workup: complete blood count and chemistry, erythrocyte sedimentation rate (ESR), and polymerase chain reaction (mandatory if temporal arteritis is suspect). If carotid disease is suspected a duplex examination is mandatory, and in some cases another neuroimaging procedure (magnetic resonance imaging (MRI) angiography or computed tomographic angiography) is required to evaluate the carotids and/or the brain (brain MRI). A cardiologic examination is essential if an embolic origin is suspected. An electroencephalogram (EEG) is necessary if epilepsy is considered to be the origin of the problem.
3.3 Diagnostic Workup of the Case
In this case the most important feature in establishing the diagnosis was the clinical history. As the patient recounted a history of stereotypical spells that described very well the fortification spectra, the origin of this visual phenomenon necessarily had to be the occipital cortex (right in the majority of episodes, although the patient referred also to episodes in the right visual field). The duration of the spells was typical for migraine aura, and the frequency (1–10 per year) and long history (17 years) was also in favor of migraine etiology.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


