Guidelines-based management of the patient with asthma allows maximal levels of function with few adverse effects. A flexible approach to therapy that emphasizes an ongoing partnership between the patient and physician allows optimal communication, facilitating treatment adherence and maximal levels of control. Through assessment of the patient’s initial severity of disease and an evaluation of the patient’s ongoing level of control, appropriate medical therapy can be initiated and level of therapy can be modified based on the patient’s response. Patient education, environmental control strategies, and proper use of medications are vital in achieving maximal benefit in asthma management. Excellent asthma control is possible and should be a goal of both physicians and patients.
Once considered primarily a disease of bronchoconstriction, the pathophysiology of asthma is now characterized by inflammation of the airway with resultant restriction in airflow secondary to this inflammation. It is this understanding of the central role of inflammation in asthma that has allowed more efficacious treatments for patients.
In 1991, the National Heart, Lung, and Blood Institute (NHLBI) described asthma as a pulmonary disease with specific characteristics: (1) reversible airway obstruction, (2) airway inflammation, and (3) increased airway responsiveness to various stimuli . This approach to asthma has been reiterated recently in the 2007 NHLBI guidelines for the diagnosis and treatment of asthma, known as EPR 3 . This document reinforces the concept that inflammation is central to the pathophysiology and symptom progression among individuals with asthma, and that effective treatment and control depend on the successful management of inflammation ( Fig. 1 ).

In the 2007 NHLBI guidelines, asthma is evaluated both by the degree of severity expressed in the patient’s symptoms, as well as by the current degree of asthma control. While severity may be more reflective of the underlying baseline of the patient’s asthma, control is more dynamic, and describes the degree to which the patient’s current symptoms are active and impact daytime function, sleep, and quality of life. These guidelines define three components of assessment and monitoring that are relevant in the evaluation of the patient with asthma:
- •
Severity: the intrinsic intensity of the disease process. Severity is most easily and directly measured in a patient who is not currently receiving long-term control treatment.
- •
Control: the degree to which the manifestations of asthma (symptoms, functional impairments, and risks of untoward events [eg, hospitalizations, exacerbations]) are minimized and the goals of therapy are met.
- •
Responsiveness: the ease with which control is achieved by therapy .
The current paper will focus on the assessment and management of the patient with asthma, and will use the 2007 NHLBI guidelines as a framework for discussion. It will first examine in greater detail the concept of asthma control, and review some of the data relative to parameters of control. It will then review options for treatment of the patient with asthma, presenting a step-care approach to management that is central to the current guidelines.
Asthma control
Observations of patients with asthma suggest that they frequently evaluate if their asthma is controlled based only on their symptoms. Subtle changes are often overlooked or may not be viewed as important. Physicians will generally rely on patients’ perceptions and individual reports of symptoms in evaluating their degree of control in the absence of objective measures. This overreliance on symptoms can overestimate asthma control and lead to ineffective asthma treatment .
An evaluation of asthma control focuses on the efficacy and success of the patient’s current treatment rather than on the patient’s underlying disease state . Asthma control is a dynamic indicator of asthma status and allows both the physician and the patient to evaluate the patient’s current medical status. When asthma guidelines are used to maximize asthma control, research has demonstrated that patients of various asthma severities can both improve their symptoms and enhance their quality of life .
In evaluating the level of asthma control, both subjective and objective indices are used by physicians and patients. In addition, both physiological and psychometric measures can be used to assess patient function, and are important in modifying medical management. Assessing asthma control allows physicians to select the most appropriate treatment based on a graded approach to asthma management.
Evaluating asthma control
As noted earlier, asthma control is generally evaluated by the patient’s self-reported observations of the prominence of their current symptoms, including shortness of breath, cough, wheeze, and nocturnal awakenings. Physicians also evaluate the frequency of the use of rescue inhalers. Studies suggest that relying on patient symptoms alone to assess asthma control may be insufficient to detect early changes in functional status . Patients who consider themselves to be under control, frequently continue to experience sleep disruption, fatigue, and decreased activity.
An accurate assessment of asthma control must also involve objective measures of lung function, such as spirometry and/or peak expiratory flow (PEF). Spirometry assesses inspiratory and expiratory phases of lung function, and demonstrates pulmonary flow through the small, distal bronchioles. Thorough diagnostic spirometry involves the administration of bronchodilators to assess the reversibility of pulmonary obstruction, since reversible obstruction to flow is characteristic of asthma. PEF can provide a simple measure of early flow and can be a method for the patient to follow lung status and detect changes at home. PEF is not as sensitive to small airway obstruction as spirometry, although it can be a useful index of changes in acute lung function.
Psychometric measures of asthma control
The availability of reliable, validated instruments to assess asthma control allows physicians to accurately evaluate patient symptoms and function. One such test that has been frequently employed in clinical practice is the Asthma Control Test (ACT). The ACT is a five-item instrument that can be used to identify patients with varying degrees of asthma control. It is easily administered in the office and can be used after downloading it from the ACT Web site ( http://www.asthmaactionamerica.org/i_have_asthma/control_test.html ). On the ACT, patients respond to five questions in which they rate their degree of asthma control over the preceding 4 weeks on five questions:
- 1.
How much of the time did your asthma keep you from getting as much done at work or home?
- 2.
How often have you had shortness of breath?
- 3.
How often did your asthma symptoms wake you up at night, or earlier than usual in the morning?
- 4.
How often have you used your rescue inhaler?
- 5.
How would you rate your asthma control?
Guidelines-based asthma control: GINA 2006
The recognition of asthma control as a dynamic index of the patient’s current asthma status was recently discussed in the 2006 GINA (Global Initiative for Asthma) guidelines. These international consensus recommendations discuss broadly the epidemiology, pathophysiology, assessment, and management of asthma. In the 2006 GINA guidelines, management strategies for asthma are primarily based on an ongoing assessment of control rather than on disease severity . These guidelines argue that control is a sensitive indicator of the patient’s asthma status.
In the 2006 GINA guidelines, components that contribute to an assessment of control include (1) daytime symptoms; (2) limitation of activities; (3) nocturnal symptoms and nocturnal awakenings; (4) the use of rescue medications; and (5) objective assessment of lung function. The goal of control in GINA is for the patient to have no daytime or nocturnal symptoms and to have no limitation in daytime activities or social function. Short-acting bronchodilators should not be used more often than twice weekly or refilled more than twice yearly, and asthma exacerbations should occur less than yearly.
Guidelines-based severity assessments: NHLBI EPR 3
The 2007 NHLBI guidelines describe asthma severity as reflecting the intrinsic intensity of the patient’s disease. The initial assessment of patients with asthma begins with the selection of a severity classification ( Fig. 2 ), as the intensity of therapy will depend on this initial assessment of asthma severity. This evaluation will generally include the patient’s assessment of symptoms and functional status over the 2 to 4 weeks before the diagnostic visit, and will use objective measurement of lung function using spirometry.

Classification of asthma severity in the 2007 NHLBI guidelines involve both the chronicity of the patient’s disease and the intensity of the patient’s components of severity. These components include (1) frequency of patient symptoms; (2) frequency of nighttime awakenings; (3) interference with normal activity; (4) frequency of short-acting beta-2 agonist use for symptom control; and (5) lung function as assessed by FEV 1 and forced vital capacity (FVC). Two broad classification categories based on the time course of the patient’s disease involve (1) intermittent asthma (symptoms occurring 2 days weekly or less/nighttime awakenings occurring 2 nights per month or less; and (2) persistent asthma (symptoms occurring more than 2 days weekly/nighttime awakenings occurring more than twice monthly). Persistent asthma is also graded by the severity and frequency of patient symptoms and by impairment in lung function, and can be classified as (1) mild, (2) moderate, or (3) severe.
Also closely associated with severity in the 2007 NHLBI guidelines is the concept of risk of adverse events, including asthma exacerbations and death. Exacerbations involve declines in lung function, and can occur in patients with both intermittent and persistent asthma. Patients at increased risk include those with severe persistent airflow obstruction, those with two or more emergency room visits for asthma annually, and current smokers.
Once the degree of asthma has been evaluated and the level of asthma severity assigned, guidelines-based therapy can be prescribed on a step-care basis and the patient followed to assess response to therapy. This step-care approach to treatment will be discussed in the next section.
Guidelines-based control: NHLBI EPR 3
The 2007 NHLBI guidelines note that ongoing monitoring of the degree of asthma control is essential in allowing patients to achieve the goals of asthma therapy. They also note that when asthma is not controlled it is associated with increased asthma burden, decreased patient quality of life, and increased use of health care resources . The NHLBI guidelines describe three levels of asthma control:
- •
well controlled
- •
not well controlled
- •
poorly controlled
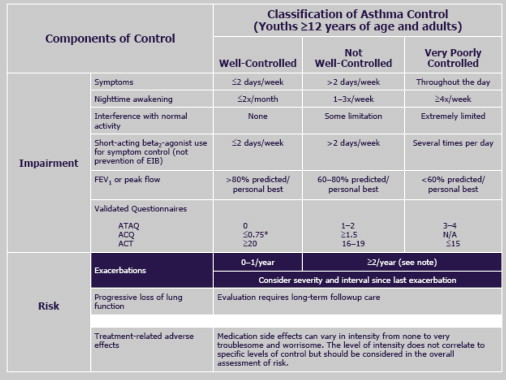
The NHLBI guidelines set certain behavioral criteria that define levels of asthma control. For a patient’s asthma to be considered well controlled, the patient must not have daytime symptoms more than twice weekly, must not awaken from sleep with asthma symptoms more than twice monthly, and must not use short-acting beta-2 agonist rescue medications more than twice weekly. In addition, asthma symptoms must not interfere with normal activities and FEV 1 must be at least 80% of predicted. Not-well-controlled asthma differs in several categories. Daytime symptoms occur more than twice weekly and nighttime awakenings from asthma occur one to three times a week. In addition, short-acting beta-2 agonist use increases to more than twice weekly and the patient begins to experience limitations in daily activities because of their asthma. Finally, FEV 1 levels are generally noted between 60% and 80% of predicted.
Poorly controlled asthma involves a significant worsening of asthma symptoms and functional impairment. Asthma symptoms persist throughout the day on a daily basis and the patient awakens with asthma more than four times weekly. The patient uses the rescue inhaler several times daily and daytime function is extremely limited. FEV 1 falls below 60% of predicted. The patient has significant impairment in both daytime and nighttime function. In cases of poorly controlled asthma, aggressive intervention is necessary to bring asthma back under control.
Earlier guidelines for the treatment of asthma primarily used assessment of disease severity in selecting appropriate medical intervention and intensity of pharmacotherapy. The major issue with this approach to therapy is that the use of severity assessments in planning treatment is not responsive to the current degree of asthma burden or impairment once the patient is on medical therapy. The 2007 NHLBI guidelines therefore argue that while the initial approach to therapy and intensity of treatment should be based on an appropriate assessment and classification of severity, once treatment is established the emphasis switches to asthma control in determining whether adjustments in therapy are necessary .
Asthma control: conclusions
Recent US and international guidelines on the treatment of asthma stress that asthma control is the most important dynamic indicator of the current status of the patient’s level of disease, and the most useful index in judging the need for adjustments in the patient’s treatment plan. While severity is important in initial treatment planning, it is not useful as an index of fluctuations in the intensity of the patient’s asthma. Assessment of asthma control should involve both subjective information involving patient symptoms and level of function, as well as an objective measure of lung function such as spirometry. Validated psychometric instruments are also available to evaluate asthma control in the office setting and at home. An asthma control measure such as the ACT used in conjunction with spirometry provides the physician with a comprehensive assessment and permits better management of the patient with asthma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


