A relationship between allergic rhinitis and acute and chronic rhinosinusitis has been postulated for many years. Epidemiologic evidence suggests that such a relationship is likely. In addition, evidence of a common pathophysiologic mechanism linking these diseases is compelling and continues to evolve. Although a clear and definitive causal relationship remains to be elucidated, an increasing number of studies support the plausibility of this link. The current paradigm of the “unified airway” and evidence to support this model further strengthen this link. This article reviews the literature relating allergic rhinitis and acute and chronic rhinosinusitis.
Although conventionally considered as distinct clinical entities, allergic rhinitis and rhinosinusitis are increasingly being regarded as interrelated and part of a spectrum of upper airway inflammatory disease. A recent article by Krouse and colleagues illustrated the concept of a “unified airway” with inflammatory processes affecting and coexisting in the upper and lower airways and underscored the importance of understanding this relationship to effectively diagnose and treat illnesses within this spectrum. Despite the lack of a clearly established causal link between allergic rhinitis and rhinosinusitis, an increasing body of evidence published in both the otolaryngology and allergy literature is strongly suggestive of a shared pathophysiologic relationship. Both conditions are characterized by an inflammatory response leading to an altered milieu within the nose and paranasal sinuses, thus rendering normal host defenses weakened and susceptible to further inflammatory insult. Although the inciting agents or factors leading to the inflammatory response, and the immunologic mechanisms driven by this response, may differ, it is logical to infer that an allergic-mediated inflammation within the nasal lining could lead to or contribute to the development of a sustained inflammatory state within the paranasal sinuses, especially if the allergic response occurs repeatedly and chronically.
Undoubtedly, the role of allergy in the pathogenesis of rhinosinusitis has been the subject of much scrutiny, debate, and controversy over the past several years. However, the compelling notion of a “unified airway” would lead one to argue that distinct clinical entities do not exist in a mutually exclusive vacuum, but rather that one entity could variably affect the development of or alter the course of another. This article will discuss both allergic rhinitis and rhinosinusitis as separate entities and will then go on to explore them as part of a spectrum of upper airway disease with a common pathophysiologic link.
Allergic rhinitis
Allergic rhinitis is a prevalent disease, estimated to affect approximately 20% of the adult population in the United States, and up to 40% of children . These statistics are even more astounding when one considers the impact that allergic rhinitis has on quality-of-life measures and societal costs. Allergic rhinitis accounts for approximately 16.7 million physician office visits annually, and its treatment with over-the-counter and physician prescriptions result in direct costs of approximately $4.5 billion/year in the United States. Furthermore, an estimated 3.8 million lost work and school days occur annually as a result of allergic rhinitis . Previous studies have demonstrated that patients with allergic rhinitis have a statistically diminished quality of life as compared with the normal population . An extensive list of allergy and allergic rhinitis statistics is available on the American Academy of Allergy, Asthma, and Immunology Web site, www.aaaai.org . Regardless of the different statistics cited in various reports, it is clear that allergic rhinitis has had a profound impact on our society.
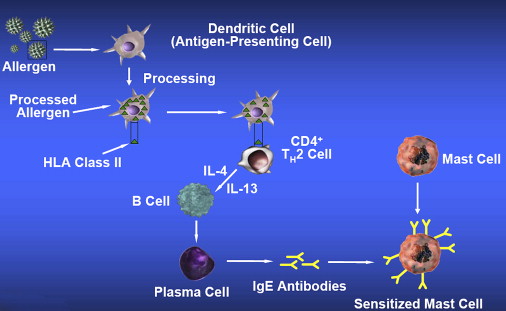
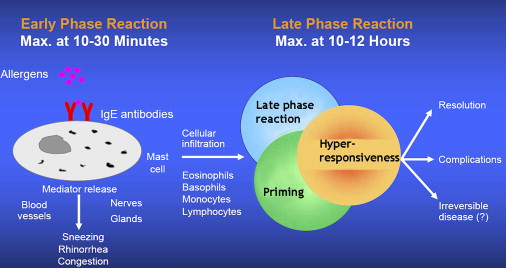
The hallmark of allergic rhinitis is an IgE-mediated, type 1 hypersensitivity reaction to an inciting inhaled antigen and, in some cases, an ingested food that causes a cross-reaction because of antigenic similarities between the inhalant and the food. The result of this reaction is a cascade of immunologic events leading to the clinical expression of the disease, which includes both nasal and non-nasal symptoms ( Box 1 ). The basic immunologic mechanisms underlying the “allergic reaction” within the nose and paranasal sinuses are well characterized. In general, allergic sensitization and response occur in a series of steps with the first step involving an Antigen Processing Cell (APC) or macrophage incorporating and processing the antigen that has entered the host. After processing the antigen, the APC contacts a CD4 + T H 2 T-helper cell via HLA Class II receptors on its cell surface. This interaction activates the T H 2 cell, resulting in the release of various cytokines, such as interleukin (IL)-4 and IL-13, which stimulate more T H 2 cells to respond to the antigen load and also cause B cells to differentiate into plasma cells that elaborate IgE antibodies specific to the antigen ( Fig. 1 ). These antibodies then attach to the surface of mast cells, rendering them “sensitized.” This phase of the immunologic response resulting in mast cell sensitization is also known as the priming phase. Subsequent allergen provocation from further allergen exposure results in mast cell degranulation and the release of pre-formed mediators, such as histamine, kinins, and proteases. This “early-phase response” occurs about 10 to 30 minutes after allergen exposure. The increased number of degranulating mast cells in the nasal epithelium produces significant vascular leakage and interstitial edema resulting in irritation of sensory nerves, nasal pruritis, rhinorrhea, nasal congestion, and sneezing. The “late phase” of this allergic response occurs approximately 4 to 8 hours after antigen exposure as a result of chemotaxis and migration of neutrophils, basophils, eosinophils, T-lymphocytes, and macrophages across the mucosal endothelium into the nasal submucosa ( Fig. 2 ). Further cytokine and chemokine release from these cells results in increased nasal inflammation and end organ damage. With repetitive allergen exposure, a priming effect occurs, where progressively smaller amounts of allergen are required to elicit an early-phase response.
Nasal
Sneezing
Rhinorrhea
Pruritis
Congestion
Smell impairment
Postnasal drip
Eustachian tube dysfunction
Non-nasal
Lacrimation
Conjunctivitis
Itching eyes
Fatigue
Sleep disturbances
Depression
Headache
Palatal pruritis
Ear fullness/otalgia
Midface pressure
Cognitive impairment
Allergic rhinitis has been conventionally divided into seasonal allergic rhinitis (SAR) and perennial allergic rhinitis (PAR). SAR, also known as “hay fever,” is the more common form, occurring during different seasons depending on the inciting inhalant antigen. Typical seasonal allergens include tree pollens in the spring, grass pollens in the summer, and weed pollens in the fall. Nasal and ocular symptoms are prominent during these exposures. PAR is the more chronic form of allergic rhinitis where symptoms occur to some degree year-round. Molds, cockroaches, mites, and animal dander are the typical inciting agents.
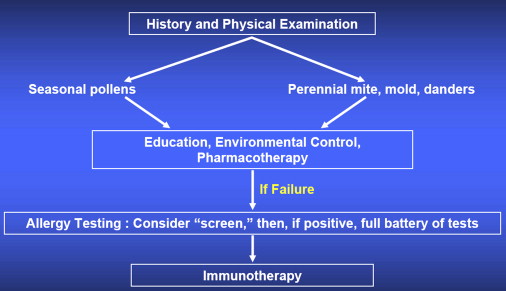
Irrespective of the plethora of classification systems used to describe allergic rhinitis, the evaluation and treatment algorithms for this disease are relatively straightforward. A thorough history will in most cases be able to distinguish allergic rhinitis and its subtypes from other common types of rhinitis (ie, infectious, occupational, chemical/irritative, anatomic, vasomotor, nonallergic with eosinophilia, medication-induced, hormonal, atrophic, and gustatory rhinitides). Several physical exam findings further corroborate the diagnosis of allergic rhinitis ( Box 2 ). Once a presumptive diagnosis of allergic rhinitis is made, then management entails educating and counseling a patient and his or her family about the disease and its treatment ( Fig. 3 ). Avoidance of triggering allergens and environmental modification are the initial measures taken to prevent or mitigate the symptoms of allergic rhinitis. Environmental measures often entail the modification of factors that are known to be or are potentially the source of the allergic response in areas such as the home, school, and workplace. Pharmacotherapy, with oral or topical antihistamines, oral or topical steroids, leukotriene inhibitor agents, mast cell stabilizers, anticholinergics, and limited use of oral or topical decongestants, plays a significant role in the management of allergic rhinitis. The unifying theme among these agents is the modulation of the immune response to the inciting agent. In some cases, the pharmacologic agent targets specific sites in the immunologic pathway (mast cell destabilizers, antihistamines) and in others, the agent has a generalized mode of action in mitigating the immune response (steroids). The efficacy and safety of these various agents have been extensively studied, and is beyond the scope of this article. The use of laboratory and skin testing enables a definitive diagnosis to be established and is required before the onset of immunotherapy, which is employed and warranted when the above measures are insufficient to attain symptom control. Documentation of specific allergen sensitivities by in vivo skin testing or in vitro serum testing allows for targeted immunotherapy. Immunotherapy involves the injection of increasing amounts of allergen every 5 to 7 days until a “maintenance dose” is achieved that relieves symptoms or is maximally tolerated. This dose is then given once every 2 to 4 weeks based on the length of symptom control. Immunotherapy is typically continued for 3 to 5 years and results in long-term symptom control in up to 75% of patients. There has been considerable interest regarding sublingual immunotherapy or SLIT, which has been widely used in Europe. This therapy entails the sublingual deposition of the allergen (in most cases many times the dose of injected allergen in conventional immunotherapy) and has been noted to achieve symptom relief after 2 years of institution. This therapy is starting to gain widespread acceptance in the United States based on many studies touting its efficacy and safety.
Ocular
Conjunctivitis
Allergic shiners—venous stasis from persistent nasal congestion leading to lower eyelid edema
Dennie’s lines—creases in lower eyelid occurring from Mueller’s muscle spasm
Allergic lashes—long, silky, full eyelashes
Nasal
Turbinate congestion/bogginess and hypertrophy
Other
Posterior pharyngeal cobblestoning
Adenoid hypertrophy
Lateral pharyngeal bands
Crowded teeth/high-arched palate
Vocal cord edema
This basic overview of allergic rhinitis serves to illustrate the important point that immune responses to various allergens lead to predictable and distinct histopathologic changes in the nasal and paranasal sinus epithelium (as both are contiguous) that can impair and overwhelm host defenses and create a milieu where further inflammatory insult would occur more readily and on a more sustained level.
Rhinosinusitis
Perhaps no other topic in the field of otolaryngology has engendered as much heated debate and conflicting opinions as that of rhinosinusitis. Its definition, classification, and management have spawned countless task forces, consensus statements, clinical studies and review articles, basic science research studies, and roundtable discussions. Ultimately, rhinosinusitis is an inflammation of the nose and paranasal sinuses, attributed to many potential factors. The term “rhinosinusitis,” as opposed to “sinusitis,” is a more accurate reflection of the anatomic and pathophysiologic relationship that occurs as a result of these instigating factors. The statistics pertaining to rhinosinusitis are no less staggering than that of allergic rhinitis, with estimates of more than 30 million Americans affected by this disease yearly . In terms of its significance as a major public health concern, it ranks similar in prevalence to hypertension and diabetes . Direct and indirect costs attributable to this diagnosis are also estimated in the billions of dollars, and the personal and societal burden from decreased productivity and diminished quality of life further attest to the negative impact of this disease.
The typical pathophysiologic schema leading to the development of rhinosinusitis starts with some inciting agent (viral, bacterial, fungal, allergen) or predisposing factor (anatomic, immunologic) leading to generalized mucosal edema and inflammation. The specific immunologic mechanisms set into motion by these agents or factors may be different, but ultimately, the basic histopathologic responses are similar. In some cases, the effect of the infectious or allergic agent may be limited to generalized mucosal edema and inflammation, and with conservative or pharmacologic measures, the inflammation dampens or subsides. In rhinosinusitis, the events subsequent to mucosal inflammation and edema are more elaborate and likely occur due to the interplay of many factors occurring in concert, rather than in the case of allergic rhinitis where the inciting agent and immune response are directly related to each other both spatially and temporally. In the development of rhinosinusitis, mucosal inflammation leads to ciliary dysfunction and mucus stasis, as well as edema of the sinus ostia. The stasis of secretions within the sinuses serves as a nidus for bacterial colonization and growth. These events coupled with the impairment of host defenses as a result of the inflammatory mediators released in response to the inciting agent, create a cycle of sustained inflammation that can chronically damage the nasal and paranasal sinus linings ( Fig. 4 ). This vicious cycle will go unabated unless antibiotics, anti-inflammatory agents, and various conservative measures are used to restore the normal sinus cycle.



