Fig. 1
Robotic neck dissection performed through a retroauricular incision
In addition to technical feasibility, outcomes of robotic neck dissection have been compared to those of conventional techniques in patients with papillary thyroid cancer [7]. In general, there are longer operative times, shorter hospital stays, equivalent complication rates, and equivalent lymph node yields when using robot approaches. Notably though, the robotic arm of the study had significantly younger patients with lower staged disease [7].
Robotic neck dissection for primary tumors other than thyroid has also been studied. Several authors have reported on the use of robotic neck dissection via the modified facelift approach for parotid tumors [6, 8], submandibular cancer [9], oral cavity cancers [10–12], and laryngopharyngeal cancer [12, 13]. The authors of these studies endorsed the technical feasibility of this procedure for low stage neck disease, and almost all patients in these studies had preoperative cN0 disease. Outcomes data was provided for robotic neck dissection and conventional neck dissection, demonstrating similar findings to the studies done comparing these approaches for neck dissection done for thyroid cancer [7, 12]. The authors found that operative times were longer in the robotic group but that hospital stay, lymph node yield, and complications were equivalent [10]. Taken together, the literature suggests that robotic transaxillary or modified facelift approaches for neck dissection are technically feasible, oncologically sound, and cosmetically superior procedures for thyroid disease and low N stage head and neck cancers.
Sellar and Parasellar Applications
One of the most logical applications of robotic surgery within the head and neck is in the sellar and parasellar region. Although it is remote from the nasal vestibule, there are multiple endoscopic approaches already described to build upon. Several authors have detailed robotic techniques used to approach the sella with varying degrees of success. The da Vinci robot from Intuitive Surgical, which has traditionally been used in the head and neck for transoral approaches, now commonly referred to as transoral robotic surgery (TORS), has been applied to surgical approaches in this region. Additionally, several authors have described novel robotic systems for use in sellar or parasellar surgery.
One group described using the da Vinci robot to access the skull base through nasal placement of the camera, and bilateral sublabial incisions with anterior and medial maxillary antrostomies (Fig. 2) [14]. The surgical corridors were then joined posterior to the nasal septum, providing good access to the sellar, parasellar, clival, and anterior skull base regions. The authors commented that the three-dimensional view and precision of the robot allowed for meticulous dural closure as well [14]. The obvious limitation with this technique is the invasive nature of the approach involving bilateral anterior maxillary antrostomies through a vestibular incision.
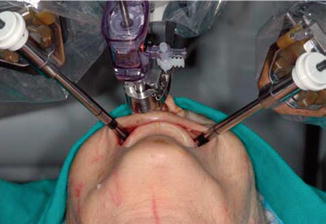
Fig. 2
Robotic Trocars placed through Caldwell-Luc maxillary antrostomies and camera placement through the right side of the nose
Another group described using the da Vinci robot to access the sella and parasellar regions through a combined oral and transcervical approach on cadavers [15]. The authors pointed out that the limitation of traditional TORS in skull base surgery is access of the mechanical instruments, even though reasonable visualization can be achieved using an angled camera. Therefore the authors placed the camera transorally and the arms of the da Vinci were placed transcervically through a blind introduction of trocars posterior to the submandibular glands. Using this technique the authors reported adequate surgical access to the sella, sphenoid, clivus, nasopharynx, and suprasellar anterior fossa [15]. Again, the limitation stems from the invasive nature of placement of the robotic arms..
Other researchers have reported the development of novel robots for assistance with sellar surgery. Nathan et al. reported the use of a robotic endoscope holder named the Automated Endoscope System for Optimal Positioning (AESOP). This robotic scope holder assists the surgeon and can be activated by voice commands to move or return to set positions. In a cadaveric study, the authors report improvement in visualization and tremor reduction, with the additional benefit of freeing the surgeon’s second hand for another instrument [16]. Another team modified a robotic endoscope holder used for ventriculostomies, the Evolution 1 from Universal Robotic Systems, for use in sellar surgery [17]. Similarly to the AESOP design, this robot is designed to free up more hands for traditional endoscopic surgery. The robotic-held endoscope is controlled from a remote joystick, and the authors reported successful two handed surgery with the scope in place [17].
Aside from the da Vinci system and the robotic endoscope holders, another group has developed a novel surgical robot, the A73, based on the RV-1a automated arms robot from Mitsubishi Electric. The robot has an arm with visualization capabilities and multiple functions, including drilling, suctioning, and flushing, and has been designed to perform automated resection of the anterior sphenoid wall. The robot integrates preoperative imaging into its surgical plan and removes the anterior sphenoid face without deep penetration in the sphenoid or into lateral structures. In a series of cadaveric heads, the robot successfully removed the anterior sphenoid wall without damage to surrounding structures in five specimens [18, 19]. Before widespread adoption of an automated surgical robot, though, large trials will need to demonstrate its reliability and safety.
Anterior Cranial Fossa Applications
The approaches previously described for the sella and parasellar regions have also been used to operate in the anterior cranial fossa on cadaveric specimens. Hanna et al described the sublabial incisions with anterior and medial maxillectomies for robotic arm placement and intranasal camera placement, and described this for use in the anterior cranial fossa as well [14]. They noted with this approach that they had excellent exposure of the cribriform plate, fovea ethmoidalis, medial orbit, and planum sphenoidale in all four cadaveric specimens experimented on. In addition they noted that the greatest advantage they perceived with this technique was magnified, tremor free closure, and suturing of dural defects [14]. Another group described a combined unilateral transmaxillary and endonasal approach to the skull base [20]. The authors reported that the endonasal portion of the surgery could be constricted and sometimes benefitted from release of the medial crural nasal cartilages from the caudal septum for increased room to maneuver. The investigators noted adequate dissection of the anterior skull base back to the region of the pituitary, allowing pituitary dissection, although they suffered from more frequent robotic instrument collisions anteriorly. The transmaxillary window was created with an osteoplastic flap that could be replaced at the end of the case [20]. The authors of these studies worked with the da Vinci robot and both noted that there was a lack of tools designed for boney work, necessitating an assistant to perform this part of the resection [14, 20].
Infratemporal Fossa and Paraphayrngeal Space Applications
Dissection of the intratemporal fossa and parapharyngeal space has also been described with robotic surgery or robotic-assisted techniques. One group described entirely transoral approaches to the parapharyngeal space and the infratemporal fossa using the da Vinci robot [8]. They were able to perform this technique on two cadaveric and one live canine specimen, with adequate access to the internal and external carotid, jugular vein, cranial nerves IX, X, XI, and XII. The authors then followed up their preclinical discussion with a report of robotic dissection and removal of a benign cystic parapharyngeal mass in a living patient. The dissection was described without complication and the wound was closed intraorally [20].
One paper described successful resection of three tumors of the parapharyngeal space via a completely transoral (TORS) approach (Fig. 3) [21]. They were successful in removal of a pleomorphic adenoma, parapharyngeal lipoma and an adenoid cystic carcinoma from paraphayngeal locations via this technique. The authors noted that the main limitations in this approach were inadequate oral access, involvement of the carotid artery, or cervical spine instability [21].

Fig. 3
Transoral resection of parapharyngeal space tumor
Another group described a combined transoral and suprahyoid transcervical approach to the infratemporal fossa using the da Vinci robot [23]. While this approach also utilized a transoral camera and robotic arm placement, it was combined with a suprahyoid pharyngotomy into the vallecula for placement of the second robotic arm. The authors noted excellent visualization of the infratemporal fossa and the limits of dissection were listed as the lower cranial nerves and jugular foramen posteriorly, the pterygoid space anteriorly, the temporomandibular joint and mandibule ramus laterally, and foramen ovale medially [23].
A different approach described using a transmaxillary placement of the da Vinci robot for cadaveric dissection [20]. The authors required an assistant to perform boney removal of the anterior osteoplastic flap, as well as the removal of the boney medial and posterior walls of the maxillary sinus. They then reported on dissection of the infratemporal fossa using the robot, noting excellent visualization for anatomic dissection [20].
It seems that dissection of the infratemporal fossa and parapharyngeal space can be achieved from a completely transoral route, although more invasive camera and arm placement have been described. Future research will need to focus on limitations of these approaches and outcomes when using this approach.
Clivus, Nasopharynx and Craniocervical Junction Applications
Robotic surgical approaches to the nasopharynx, clivus, and craniocervical junction have been described using the da Vinci surgical robot. For nasopharyngectomy a preclinical study on cadavers compared a strictly transoral (TORS) approach to a combined transnasal and transoral approach [24]. In the traditional TORS procedure all of the robotic arms were placed transorally, while in the combined procedure investigators placed the camera transnasally and the robotic working arms transorally. The authors noted improved visualization of the surgical field with the combined approach, although they also noted that the procedure could be accomplished from either route. Additionally the authors noted that the cadaveric study was performed in an edentulous patient, and they felt the presence of teeth would limit transoral robotic arm placement. The authors then described a transcervical placement of the robotic working arms posterior to the submandibular gland with transnasal camera placement based on the cervical TORS (C-TORS) technique (Fig. 4) [22, 24].
 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
