Antral Lavage
Elina M. Toskala
INTRODUCTION
Interest in maxillary sinus pathology began in the 17th century, and trephination of the antrum for suppuration was the most common operation on the maxillary sinus in that period. One of the first descriptions of an intranasal antrostomy was by Gooch in the 1770s. Routine puncture of the inferior meatus became more common in the 1880s after publications describing the use of the needle, trocar, and stylette to puncture the wall of the inferior meatus. In 1890, Lichwitz invented the cannula accompanied with the perforating needle. Later operations left the opening through the canine fossa into the antrum open for repeated lavages. Caldwell (1893), Scanes Spicer (1894), and Luc (1897) used the canine fossa incision but closed it following removal of infected mucosa and the creation of an intranasal antrostomy.
Acute maxillary sinusitis (AMS) is a common health care problem that is said to affect 2% of people with upper respiratory tract infections (URIs). AMS should be suspected in patients who have had a history of recent viral URI and symptoms of purulent nasal discharge, nasal blockage, and often facial pain, which have continued over a week after the initial symptoms began. The diagnostic methods vary, and there is not one single method that can be used to definitively diagnose bacterial AMS, except aspiration of the maxillary sinus. The diagnosis in most cases is based on symptoms and clinical examination alone. Radiographic plane film imaging of the sinuses or a limited CT scan has been used, but they are not sensitive or specific enough and are really not needed to diagnose uncomplicated bacterial AMS. Imaging does not differentiate bacterial from viral infections. Ultrasound is also used in some countries, although rarely in the United States.
AMS is by definition inflammation of the mucosa of the paranasal sinus with retention of fluid (purulent exudate) in the sinuses. This fluid is contaminated by bacteria in most cases. Edema of the mucosa of the osteomeatal complex causes blockage of the maxillary sinus and in some cases the frontal sinus, resulting in a feeling of increased pressure and pain in the face.
Puncture of the sinus and aspiration of fluid for bacterial culture are considered to be the gold standard in the diagnosis of maxillary sinusitis. Cultures obtained by rigid nasal endoscopy have also been proven to be a reliable method for detecting the major pathogens in AMS and are easier to obtain.
In most cases, the first line of therapy is antibiotics and nasal decongestants without bacterial cultures. When symptoms persist, antral lavage has been used to relieve the feeling of pressure in the sinuses and improves the patency of the maxillary ostium. It is thought that washing out the bacterial should improve resolution of the infection. Patients often feel immediate relief of their pressure symptoms when the purulent exudate is drained from the sinus, and the ostium is opened by the pressure from saline used for lavage. Antral lavage also provides material for culturing the bacteria causing the persistent symptoms and directs the antibiotic treatment based on sensitivity of the bacteria to antibiotics instead of empiric antibiotic treatments that are often used at the onset of AMS (Fig. 10.1).
Although antral lavage has fallen out of fashion, it is an effective, rapid, and inexpensive procedure with a long-standing history of success. Indeed, to date, there have been no controlled studies comparing antral lavage to balloon dilatation of the ostium of the maxillary sinus. Although balloon dilatation of the ostium is currently en vogue, there is still a lack of evidence of improved efficacy with the more expensive balloon dilatation approach.
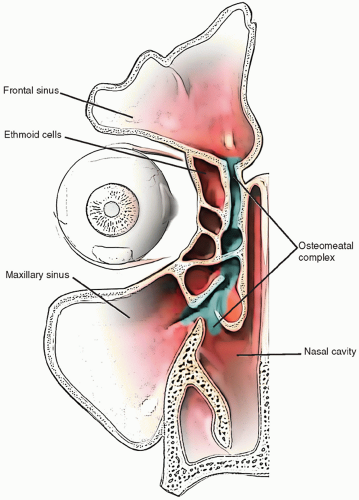 FIGURE 10.1 Schematic of maxillary sinus, ostium, osteomeatal unit, and the nasal cavity. |
HISTORY
The typical patient referred for antral lavage presents with a recent history of an URI. Although the viral symptoms may have resolved, the patient presents with localized pain and pressure in the area of one maxillary sinus. The patient has usually been started on antibiotics by his or her primary care physician but continues to have worsening discomfort localized to the area of the involved maxillary sinus. The discomfort interferes with the patient’s sleep and is not relieved by anti-inflammatory agents or a topical nasal decongestant. The patients feel that the area over the sinus is swollen and report a low-grade fever. Usually, no frontal or vertex headache is reported. Symptoms of pain in the teeth should be elicited.
PHYSICAL EXAMINATION
Examination of the face may be normal, although in some cases, edema and ecchymosis may be present. Extraocular movements should be intact. Anterior rhinoscopy demonstrates discharge in the nasal cavity with edema and erythema of the mucosa. There may be tenderness on palpation of the affected maxillary sinus, and the patient reports a feeling of pressure in the cheek area when the head is bent forward. Examination of the pharynx and larynx demonstrates some degree of purulent exudate. Nasal endoscopy usually demonstrates marked edema in the middle meatus with purulent exudate on the affected side. There is reduced transillumination over the affected maxillary sinus. The contralateral maxillary sinus and both frontal sinuses usually transilluminate normally. The maxillary dentition should be examined and the teeth individually tapped with a tongue blade. If pain is elicited, one must be suspicious of a periapical abscess giving symptoms of pain in the face similar to maxillary sinusitis.
INDICATIONS
Acute bacterial maxillary sinusitis causing symptoms of pressure and pain in midface.
A feeling of numbness of the teeth or symptoms that do not resolve with symptomatic medical treatment.
The upper respiratory infection has persisted over 7 days, and the patient is agreeable to the procedure.
Imaging of the maxillary sinus can be done by plane radiography to identify the degree of pneumatization, in the presence of maxillary sinus opacification or air-fluid level. However, this study does not provide reliable information regarding associated ethmoid disease. Young children should have an antral lavage only under general anesthesia. This could be done, for example, when a patient undergoes adenoidectomy or tympanostomy and has had AMS that has not resolved with antibiotics and decongestants, and the radiograph demonstrates that child has sinuses that has been aerated and sufficiently developed to perform the procedure.
Patients who are on mechanical ventilation may develop sinusitis, and antral lavage can be performed at the bedside under local anesthesia to improve sinus clearance of purulent secretions that may otherwise slow the patients’ overall recovery.
CONTRAINDICATIONS
The main contraindications for sinus lavage are anatomical, young age, and patient refusal. Maxillary sinus lavage under local anesthesia is best avoided in patients who are anxious because they are subject to some discomfort and a cracking sound as the trocar enters the sinus.
Previous sinus surgery to the inferior aspect of the medial wall of the maxillary sinus due to Caldwell-Luc, inferior antrostomy, or medial maxillectomy could cause the trocar to enter through the posterior wall of the maxillary sinus. Physicians should always ask about prior sinus surgery before proceeding with the lavage. Thick bone on imaging or an underdeveloped maxillary sinus is a contraindication to maxillary sinus lavage.
A prior orbital blowout fracture.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


