Purpose
To report pathologic evaluation and diagnostic yield of an aspiration cutter-assisted biopsy of anterior segment tumors.
Design
Retrospective, consecutive, interventional case series.
Methods
Fifty-five eyes of 55 patients with iris and iridociliary tumors underwent an aspiration cutter-assisted biopsy at a single institution. Cytospin and cell-block preparations were performed on all biopsy samples. Bleached preparations and a panel of immunohistochemical stains were performed in selected cases. Cytologic diagnosis was correlated with clinical diagnosis and with histopathologic diagnosis, when available. Main outcome measures were (1) specimen cellularity, (2) diagnostic studies performed, (3) cytopathologic diagnosis, and (4) concordance with histopathologic diagnosis.
Results
Specimen cellularity was adequate for cytopathologic interpretation of cytospin preparations in 55 (98.2%) of 56 biopsies. Twenty-three (41%) of 56 biopsy samples had diagnostic material in cell-block preparations. The most common cytopathologic diagnoses were melanoma (n = 39/56; 69.6%), melanocytoma (n = 4/56; 7.1%), nevus (n = 4/56; 7.1%), lymphoma (n = 2/56; 3.6%), and epithelial implantation cyst (n = 2/56; 3.6%). One biopsy sample (1.8%) yielded nondiagnostic material. Wide incisional or excisional biopsy confirmation was available in 13 (23.2%) of 56 aspiration cutter-assisted biopsy cases. Cytopathologic diagnoses were consistent with histopathologic diagnosis in 12 (92.3%) of 13 cases.
Conclusions
Although specialized pathologic techniques were necessary to maximize material available for diagnosis, all biopsies yielded cellular material and 41% yielded diagnostic tissue in cell block preparation. Although lower than the yield of wide incisional or excisional biopsy, aspiration cutter-assisted biopsy of anterior segment tumors achieved a diagnostic yield of 98.2%.
Iris and iridociliary tumors are easily accessible to biopsy in cases where clinical diagnosis is equivocal. Although these lesions traditionally have been managed with wide incisional or excisional biopsy (iridectomy or iridocyclectomy) or enucleation, less invasive diagnostic techniques recently have been advocated, such as fine-needle aspiration biopsy (FNAB), vitrector-assisted biopsy, and Kelly punch-assisted biopsy. The diagnostic yield of these alternative biopsy methods can be limited by small tissue sample size.
In 2005, the Finger iridectomy technique for biopsy of anterior segment tumors was described. In summary, an aspiration cutter was inserted through a clear corneal incision while anterior chamber depth was maintained with viscoelastic. Both full- and partial-thickness biopsy samples were obtained with machine-controlled suction and cutting speeds. Both iris and ciliary body tumors were sampled. The viscoelastic was removed and the wounds typically were self-sealing. Using a small-gauge aspiration cutter allowed for a relatively small incision. Advantages of this approach include that using a clear corneal incision guaranteed that any tumor liberated from the wound not be retained beneath conjunctival tissue and that the use of viscoelastic both maintained anterior chamber depth and stabilized the iris and tissue sample (compared with saline infusion techniques). When compared with their experience with FNAB, the authors found that this technique resulted in partial thickness and iridotomy-like full-thickness biopsies, which allowed for larger specimens and retained iris function. This article describes our experience with pathologic evaluation of iris and iridociliary tumor biopsy samples obtained with this aspiration cutter technique.
Methods
A retrospective, consecutive, interventional, noncomparative, single-center case series study was performed. This involved a review of the medical records and pathologic slides of 55 patients (55 eyes) who underwent 56 aspiration cutter-assisted biopsies at The New York Eye and Ear Infirmary. One patient underwent 2 biopsies. The biopsied material was assessed for (1) cellularity, (2) diagnostic studies performed, (3) cytopathologic diagnosis, and (4) concordance with histopathologic diagnosis.
Pathologic Analysis
The typical specimen from aspiration cutter biopsy consisted of 2 to 3 syringes, each containing 0.2 to 0.3 mL of fluid (aqueous and viscoelastic) with small-suspended tissue fragments. The specimen was assessed grossly for cellularity. One to 2 cytospin preparations were prepared from each syringe. Any remaining specimen was processed for cell-block preparation.
Cytospin Technique
A cytospin technique for aspiration cutter-assisted biopsies has been described in detail. Briefly, approximately 0.5 mL of fluid sample with an equal amount of cytospin collection fluid (70% ethanol) were added to the cytospin sample delivery chamber (cytospin slides filter cars, sample chambers metal clips, and collection fluid all from Thermo-Shandon, Pittsburgh, Pennsylvania, USA). After spinning at 1800 rpm for 2 minutes, the slides were removed from the cytospin chamber and fixed in 95% alcohol fixative or cytologic fixative (70% alcohol/formalin). In this study, the cytospin technique was the preferred method of pathologic evaluation in biopsies that appeared paucicellular on gross inspection.
Fibrin Clot Cell-Block Technique
The fibrin clot cell-block technique was implemented to maximize diagnostic material in a cell block preparation. After cytospin preparation, the remaining specimen and syringe washings with balanced salt solution (to maximize yield) were poured into 50-mL test tubes and were centrifuged at 2500 rpm for 10 minutes. After the supernatant was discarded, 3 to 8 drops of human plasma and 3 to 8 drops of dissolved thromboplastin with calcium (Dade Innovin, cat. no. B4212–100; Siemens Healthcare Diagnostics, Inc, Indianapolis, Indiana, USA) were added to the cell sediment and mixed. The resultant formed clot was wrapped in lens paper, was placed in a processing-embedding cassette, was fixed in 10% neutral-buffered formalin, and was processed routinely for pathologic evaluation.
Histopathologic and Immunohistochemical Evaluation
All cytospin and cell block preparations were stained with routine hematoxylin and eosin stain. Bleached preparations were performed on cell blocks when cytoplasmic pigment precluded evaluation of nuclear detail. Immunohistochemical stains were obtained on cytospin, cell block preparations, or both in selected cases and included melanocytic markers (S-100, MART-1, HMB45), cytokeratins (CAM 5.2, CK20, CK7, LMWCK, HMWCK), thyroid transcription factor (TTF-1), macrophage marker CD68, and leukocyte markers (CD45, CD20, CD3). In this series, biopsy specimens were examined by 2 or 3 ophthalmic pathologists (T.M., S.A.M.) and a consensus diagnosis was rendered.
Results
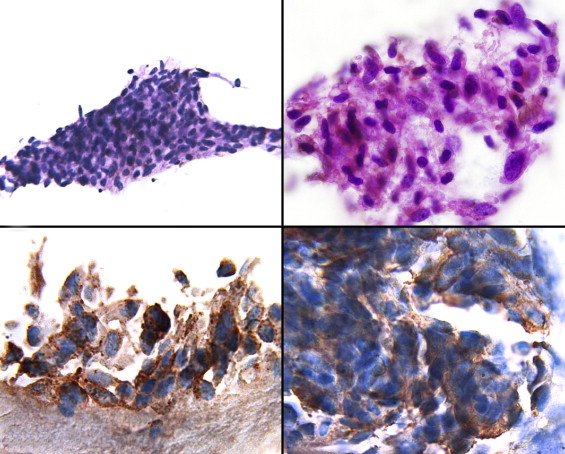
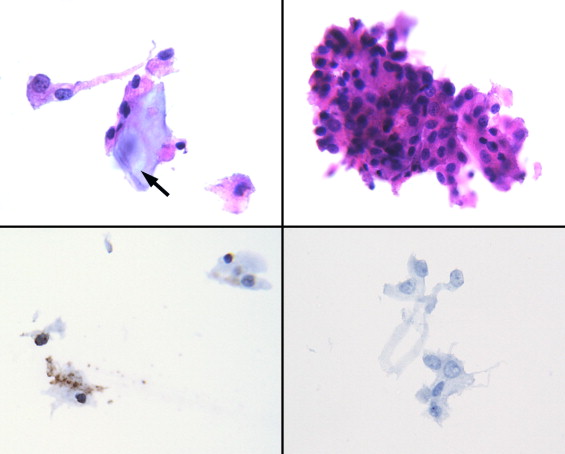
The pathologic characteristics of 56 aspiration cutter-assisted biopsies are summarized in the Table . Specimen cellularity was adequate for cytopathologic interpretation of cytospin preparations in 55 (98%) of 56 biopsies. Twenty-three (41%) of 56 biopsies biopsy samples had diagnostic material in cell-block preparations. Small tissue fragments, allowing limited histopathologic evaluation, were present in 35 (62.5%) of 56 biopsies. The most common cytopathologic diagnosis was malignant melanoma, accounting for 39 (69.6%) of 56 cases ( Figure 1 ). Benign melanocytic lesions (spindle cell nevus and melanocytoma) were the second most common category, each accounting for 4 (7.1%) of 56 cases ( Figure 2 ). There was 1 case each (1.8 %) of adenocarcinoma of nonpigmented ciliary body epithelium ( Figure 3 ), metastatic carcinoma ( Figure 4 ), and invasive conjunctival squamous cell carcinoma. There was 1 case of remarkable iris stroma consistent with posttraumatic iris lesion (diagnosed in 1 patient with a history of several intraocular surgical procedures and renal cell carcinoma who underwent iris biopsy to rule out metastasis).
| Cytopathologic Diagnosis | No. (%) | Histopathologic Diagnosis | No. (%) |
|---|---|---|---|
| Melanoma | 39 (69.6%) | Melanoma | 4 (7.1%) |
| Necrotizing granulomas | 1 (1.8%) | ||
| Melanocytoma | 4 (7.1%) | Melanocytoma | 1 (1.8%) |
| Nevus | 4 (7.1%) | N/A | 0 (0%) |
| Large B-cell lymphoma | 1 (1.8%) | Diffuse large B-cell lymphoma (lymph node biopsy) | 1 (1.8%) |
| B-cell lymphoma, NOS | 1 (1.8%) | N/A | |
| NPCE tumor, likely low-grade adenocarcinoma | 1 (1.8%) | Low-grade adenocarcinoma of NPCE | 1 (1.8%) |
| Invasive conjunctival SCCA | 1 (1.8%) | Invasive conjunctival SCCA | 1 (1.8%) |
| Malignant epithelial cells, consistent with endometrial carcinoma | 1 (1.8%) | Endometrial carcinoma (endometrial biopsy) | 1 (1.8%) |
| Epithelial implantation cyst | 2 (3.6%) | Epithelial implantation cyst | 2 (3.6%) |
| Chronic inflammation | 1 (1.8%) | Sarcoid granuloma | 1 (1.8%) |
| Unremarkable iris stroma, consistent with posttraumatic deformity | 1 (1.8%) | N/A | 0 (0%) |
| Total | 56 (100%) | Total | 13 (23.2%) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


