Purpose
To evaluate the long-term age-related anterior chamber changes by anterior segment optical coherence tomography (OCT) and the impact of such changes on the stability and behavior of angle-supported phakic intraocular lenses (IOLs).
Design
A retrospective consecutive observational cohort study.
Methods
A total of 23 eyes with high myopia implanted with an angle-supported phakic IOL between 1990 and 1996 at Vissum Corporación Oftalmológica de Alicante were included in the study. Patients were evaluated using OCT. Anterior chamber depth, anterior chamber width, crystalline lens rise, and the distance between phakic IOL and endothelium were measured.
Results
Fifteen years after implantation, anterior chamber depth was 2.9 ± 0.3 mm, crystalline lens rise 748.18 ± 393.13 μm, and phakic IOL–endothelium distance 2.1 ± 0.30 mm. The predictive model showed that 30 years after implantation, endothelial cell count was less than 600 cells/mm 2 in patients with a preoperative spherical equivalent of -25 diopters (D). Twenty years after implantation, the safety zone of 1.5 mm between endothelium and the lens will not be respected in patients with a preoperative spherical equivalent of -20 D.
Conclusions
The findings of this study could have an important influence on the decision about the indication to implant angle-supported phakic IOLs in young patients with a long postoperative life expectancy, as age-related changes in the anatomy of the anterior segment may create a long-term hazard for the implanted eye.
Over the last 2 decades, phakic intraocular lenses (IOLs) have proven to be a safe and reliable method for correcting high myopia, hyperopia, and astigmatism, as long as strict patient selection inclusion criteria for implantation are applied. Improvements in the safety of these procedures will be achieved when accurate measurements of the anterior chamber are obtained.
Several studies have been conducted on the use of anterior segment optical coherence tomography (OCT) for anterior segment measurements. The potential mechanical contact between the phakic IOL and the corneal endothelium has been suggested as the principal risk of endothelial cell loss.
Other studies described the effect of aging on the anterior chamber and the consequent modification in crystalline lens shape and volume. The lens thickness increases from 18-20 μm every year.
Baikoff suggested that the safety distance between the edge of the optic of an angle-supported phakic IOL and the endothelium has to be a minimum of 1.50 mm. If this distance is not respected, eye rubbing can give rise to endothelial alterations caused by the contact of the endothelium with the edge of the phakic IOL.
The increase in the lens thickness leads to a reduction in the anterior chamber depth of approximately 18.3 μm per year. This means that after 20 years, the anterior pole of the crystalline lens has moved forward by 400 μm.
In order to implant an anterior chamber lens, the patient selected should have a mean crystalline lens height of a maximum of 300 μm at the time of implantation. This would allow forward movement of the crystalline lens over 20 years maintaining the phakic IOL within the safety zone. Therefore, 700 μm can be considered as the safety margin required for phakic IOL vault (300 μm mean crystalline lens height + 400 μm crystalline lens rise; over a 20-year period of crystalline lens growth = 700 μm).
Taking this into consideration, the phakic IOL must be placed within a safety zone consisting of a distance of 1.5 mm from the endothelium at the front and at the back by the theoretical 400 μm protrusion of the anterior pole of the lens with respect to the base line joining the 2 recess angle points ( Figure 1 ).
Based on these considerations, we decided to investigate the change in the anterior chamber related to age in patients implanted with angle-supported phakic IOL (Baikoff ZB; Domilens, Lyon, France) This is the first study with a long follow-up on eyes implanted with this angle-supported phakic IOL model.
Patients and Methods
Patients implanted with Baikoff ZB (Domilens) at Vissum Corporacion Oftalmológica de Alicante between December 1990 and July 1996 were identified from surgical records (n = 123; 208 eyes). Of these, 23 eyes (14 patients) had over 15 years of follow-up without any further surgical procedure or ocular inflammation. The patients had a preoperative spherical equivalent refraction ≥−10.00 diopters (D) of myopia. The selection criteria for angle-supported phakic IOL implantation were the following: anterior chamber depth ≥3 mm from the corneal endothelium to the anterior capsule of the lens as measured by A-scan ultrasonography; endothelial cell density ≥2000 cells/mm 2 in patients aged ≥25 years and 2500 cells/mm 2 for younger patients with a stable refraction for a minimum of 2 years of preoperative follow-up. Exclusion criteria included patients aged ≤20 years, anterior chamber congenital abnormalities, history of uveitis, anterior or posterior synechiae, and eyes with other surgery prior to the implantation and during the follow-up.
The ethical board committee of Vissum Corporación Oftalmológica de Alicante approved the retrospective revision and analysis, for scientific purposes, of the ophthalmologic data obtained from the patients included in the present investigation. Each patient gave informed consent for this research. The study was conducted in accordance with local and regional regulations, good clinical practices, and the tenets of the Declaration of Helsinki.
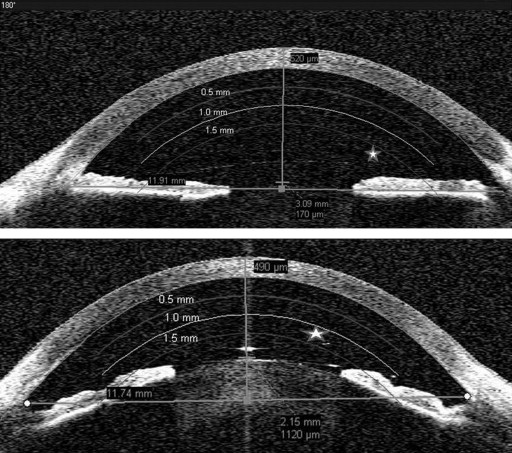
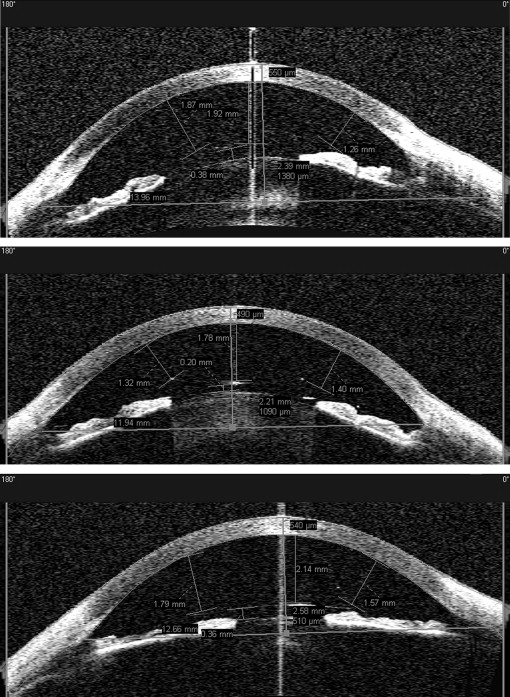
Patients were evaluated using a high-resolution anterior segment Visante OCT (Carl Zeiss Meditec Inc. Dublin, California, USA). This instrument provided images of the anterior chamber using 1300 nm wavelength infrared light. The technique works by splitting the light source into a reference and a measurement beam. The measurement beam from the ocular structures interacts with the reference light reflected from the reference mirror causing interference. Once the eye is aligned, the anterior segment can be scanned several times. Manifest refraction was tested before the OCT scans to compensate for spherical ametropia during scanning. To acquire images of the unaccommodated eye, the focus of an internal fixation target was adjusted with reference to the subject’s refraction. All examinations were performed in a room with dim illumination. Each image was displayed on a computer screen. The measurements were evaluated using the refractive tools provided by the manufacturer: distance between the anterior surface of the center of the phakic IOL and the corneal endothelium, distance between the posterior surface of the center of the phakic IOL and the anterior surface of the crystalline lens, and distances between the edges (nasal and temporal side) of the phakic IOL and the corneal endothelium. Three anterior segment parameters, including horizontal anterior chamber width (measured from the recesses of the iridocorneal angle on each side of the eye’s optical axis), anterior chamber depth (measured from the central anterior corneal epithelium to the anterior crystalline lens capsule), and crystalline lens rise (measured by the anteroposterior distance between the anterior face of the lens and the recess-to-recess line ), were taken. Examples of different crystalline lens rises are shown in Figure 2 .
These measurements were performed according to the methods described by Huang and associates and by a qualified expert in the use of anterior segment OCT technology used for this investigation. We did not evaluate the change in anterior chamber depth during accommodation because it would have meant adding another variable influenced by age. According to other authors, the movement of the lens towards the endothelium is 100 μm at 40 years and nil at 65 years. These data did not affect our population, where only 2 patients were younger than 45. Furthermore, in a previous report accommodative changes in the anterior chamber depth were studied in a population with high myopia and the decrease in the anterior chamber depth with accommodation was on average 1.5 times lower than that of emmetropic eyes. In our population the spherical equivalent range was −11 to −21 D.
For each patient, we considered the age at the first visit and the age at implantation. Cataract type and morphology were evaluated using the Lens Opacities Classification System III (LOCS III). Ocular hypertension was defined as intraocular pressure elevation >21 mm Hg. Endothelial cell loss was calculated as: ECDi = ECD0 (1 − % of loss/100) × n. ECDi is the current cell density estimated at any moment, ECD0 is the cell density at the first visit, and n is follow-up in years. Main outcome measures were evaluations of the anterior segment OCT measurements after at least 15 years of implantation of an angle-supported phakic IOL (Baikoff ZB; Domilens).
Data Analysis and Statistics
For the statistical treatment of the data, the program used was SPSS 17.0 for Windows (SPSS, Chicago, Illinois, USA). Kolmogorov-Smirnov test was applied for all data samples in order to check normality. Wilcoxon test for paired data was applied to assess the significance of differences between preoperative and postoperative data. The level of statistical significance was always the same ( P < .05). Correlation coefficients (Pearson or Spearman, depending on whether normality could be assumed) were used to assess the correlation between variables. Two predictive models were developed using multiple linear regression analysis to predict changes in endothelial cell count and in the anterior chamber depth. The regression analysis was carried out using different methods (backward, forward, and stepwise) with the purpose of contrasting the reliability of the model obtained, not depending on the method used. Selected variables by the 3 mentioned methods were always the same. Finally, we applied the method “enter.”
Results
The study evaluated 23 eyes of 14 patients with a mean age at the last visit of 49.6 ± 7 (SD) years (range 40-64 years) with a minimum follow-up of 15 years and a median follow-up for implantation of 19.8 ± 5.2 years. The mean preoperative spherical equivalent refraction was -16.02 ± 3.40 D (range: −11 to −21 D) and at 15 years postoperatively, it was −1.75 ± 3.01 D (range: −11.75 to −1.75 D) (Wilcoxon test; P < .001). The mean best-corrected visual acuity (BCVA) at the preoperative visit was 0.4 ± 0.20 logMAR (Snellen 20/50) and at the end of follow-up 0.18 ± 0.1 logMAR (Snellen 20/30) (Wilcoxon test; P < .01). Fifteen years after implantation, anterior chamber depth was 2.87 ± 0.3 mm, crystalline lens rise 748.18 ± 393.13 μm, phakic IOL–endothelium nasal edge 1.62 ± 0.25 mm, phakic IOL–endothelium temporal edge 1.8 ± 0.28 mm, phakic IOL–endothelium in the center 2.1 ± 0.30 mm, and phakic IOL–crystalline lens 0.5 ± 0.15 mm. A significant correlation was found between crystalline lens rise and age at the end of the follow-up (r = 0.473; P < .026). Anterior chamber depth showed a negative correlation with age (r = −0.257; P < .236). The distance between phakic IOL and endothelium also had a negative correlation with age (r = −0.146, P < .507). Mean endothelial cell density preoperatively and at the end of the follow-up was 2856 ± 517 cells/mm 2 and 2005 ± 570 cells/mm 2 , respectively (Wilcoxon; P < .01). The median coefficient of endothelial cell loss was 27.6% (range: 1.5 to 75%). A positive correlation was found between number of years of angle-supported phakic IOL implantation and endothelial cell loss (r = 0.671; P = .001). The overall initial and final variables are shown in Table 1 .
| Characteristic | Preoperative Data Mean ± SD | Outcome Data Mean ± SD | P Value a |
|---|---|---|---|
| Spherical equivalent (D) | −16.02 ± 3.40 | −1.75 ± 3.01 | <.001 |
| BCVA (logMAR) | 0.4 ± 0.20 | 0.18 ± 0.1 | <.010 |
| Endothelial cell count (cells/mm 2 ) | 2856 ± 517 | 2005 ± 570 | <.010 |
| Anterior chamber depth b (mm) | 3.28 ± 0.2 | 2.87 ± 0.3 | <.0001 |
a Comparison was made between 2 related samples with the Wilcoxon test.
b The comparison between these measurements suffered a bias of different instrument ultrasound A-scan (preoperative data) vs Visante optical coherence tomography (postoperative data).
Predictive Models
A linear regression model was developed for the postoperative value of the endothelial cell count. The endothelial cell count (ECC) showed strong and significant correlations with 2 variables: preoperative spherical equivalent (SE) (r = 0.692, P = .001) and number of years of implantation (r = 0.671, P < .001). These 2 variables were included in the following linear regression model for the calculation of the endothelial cell count at the end of the follow-up:
The spherical equivalent is in diopters and time of implantation (TI) in years. This equation predicts a loss of 67 cells per diopter of spherical equivalent. The more negative the spherical equivalent, the higher the endothelial cell loss. The model also predicts a loss of 49 cells per year since implantation of the lens.
Predictability was R 2 = 0.624 (R 2 adjusted = 0.582), P < .001. No influential points or outliers were detected: mean Cook’s distance = 0.074 ± 0.162. The unstandardized residuals were normally distributed ( P = .200), confirming homoscedasticity of the model. Ninety percent of unstandardized residuals were lower than 1.020 with a 95% confidence interval ranging from −0.043 to 0.043. The Durbin-Watson was 1.650, showing the independence of the residuals. Multicollinearity tests were also examined, providing variance inflation factors (lower than 1.349). Low values for the condition indexes were confirmed, with a maximum value of 10.802.The values predicted by the model are presented in Table 2 .
| Pre SE (D) | TI (y) | |||||
|---|---|---|---|---|---|---|
| 15 | 20 | 25 | 30 | 35 | 40 | |
| −10 | 2580 | 2334 | 2088 | 1842 | 1596 | 1350 |
| −15 | 2243 | 1997 | 1751 | 1505 | 1259 | 1013 |
| −20 | 1907 | 1661 | 1415 | 1169 | 923 | 677 |
| −25 | 1570 | 1324 | 1078 | 832 | 586 | 340 |
| −30 | 1233 | 987 | 741 | 495 | 249 | 3 |
| −35 | 895 | 649 | 403 | 157 | – | – |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


