Purpose
To compare wound characteristics and integrity of the 2.2-mm and 2.65-mm clear corneal incisions.
Design
Prospective, randomized clinical trial.
Methods
Patients undergoing phacoemulsification with lens implant were randomized to receive a 2.2-mm or 2.65-mm temporal clear corneal incision. The incisions were evaluated at 2, 24, and 96 hours for gape and wound architecture using anterior segment optical coherence tomography and for integrity using the Seidel test. Squareness of an incision was calculated (ratio of the incision length to the width).
Results
There were 30 patients in each group. Both incision sizes were watertight, although a mild internal main wound gape was detected on anterior segment optical coherence tomography in 35 eyes (58.3%) at 2 hours. The smaller wound was more square (0.81; standard deviation [SD], 0.11) than the larger wound (0.62; SD, 0.08; P < .001, t test). The mean squareness of eyes without wound gape at 2 hours (0.66; SD, 0.11) was lower than those with a wound gape (0.75; SD, 0.14; P = .008). A squareness factor of 0.72 or more had a positive predictive value for presence of wound gape at 2 hours of 79.3% and a negative predictive value of 61.3%. One side port incision with squareness of 1.39 had a mild leak at 2 and 24 hours, but no gape was seen on anterior segment optical coherence tomography.
Conclusions
Both the 2.2-mm and 2.65-mm clear corneal incisions clinically were competent, but the side port incision may leak. A truly square wound has a greater likelihood of being associated with internal wound gape at 2 hours after surgery, especially if the squareness factor is 0.72 or more.
Phacoemulsification using a clear corneal incision is the preferred technique of cataract removal today. However, there has been growing concern that the incidence of postcataract endophthalmitis is on the rise, and this has been observed to coincide with the increasing trend of using sutureless temporal clear corneal incisions (CCI) as compared with the scleral tunnel incisions used in the past. In the European Society of Cataract and Refractive Surgery multinational prospective study on postcataract endophthalmitis, the incidence of infection was 0.38%.
Recent studies using laboratory models have demonstrated that CCIs may behave as valves during intraocular pressure (IOP) fluctuations, for example during episodes of hypotony in the early postoperative period, or after eye blinking or rubbing, thereby possibly permitting fluid from the ocular surface to enter the eye through a wound gape. Pathogens thus may gain entry into the anterior chamber after surgery. In fact, wound leak on the first postoperative day has been associated most strongly with postoperative endophthalmitis. Furthermore, toxic anterior segment syndrome on the first postoperative day has been described in a series of 8 patients as a result of antibiotic and steroid ointment migrating into the anterior chamber from the ocular surface. This supports the hypothesis that the extraocular fluid can enter the wound within the first 24 hours after surgery. Severe postoperative hypotony likely is the result of loss of wound apposition and leakage, especially in the first 24 hours. One of the proposed benefits of a paradigm shift from coaxial to microcoaxial phacoemulsification is the reduced risk of postoperative endophthalmitis, which has yet to be supported by published data.
Anterior segment optical coherence tomography (AS OCT) has been found to be useful in evaluating incision architecture, and recent studies suggest that CCIs seem to be safe. In this study, we used the AS OCT to study the architecture of CCIs, and in particular wanted to compare the difference in wound integrity, if any, between the 2.2-mm and 2.65-mm incisions.
Methods
This was a prospective, randomized study conducted at the Singapore National Eye Centre. Consecutive patients who had no ocular pathologic features other than cataracts and were planning to undergo phacoemulsification with intraocular lens (IOL) implantation were recruited to participate in this study. All preoperative assessments were performed by 1 observer (A.S.Y.C.) and included documentation of the density of the nucleus (using the Lens Opacities Classification System III grading scale whereby grades 1 to 2 were categorized as soft, grades 3 to 4 were categorized as hard, and grades 5 to 6 were categorized as extremely hard). The intraocular pressures (IOPs) were measured using Goldman applanation tonometry, and the mean of 3 readings was taken. The axial length was measured using the IOL Master (Carl Zeiss Meditec, Inc., Jena, Germany), unless it was unable to give good measurements, in which case the immersion technique was used (Ocuscan; Alcon Laboratories, Inc, Fort Worth, Texas, USA).
After informed consent, the patients were randomized (using a list of computer-generated random numbers at the time of arranging the surgical date) to receive either a 2.2-mm or 2.65-mm CCI. The phacoemulsification with IOL implantation was performed by 1 of 3 consultant surgeons (S.-P.C., S.-E.T., L.L.). The patients were reviewed postoperatively at 2, 24 and 96 hours by a single masked investigator (A.S.Y.C.). The following assessments were made during these visits: imaging of the center of main and side port incisions using AS OCT (Visante, Model 1000; Carl Zeiss Meditec, Inc.) by a single trained technician, slit-lamp examination of the wounds looking in particular for wound gape and wound integrity using the Seidel test, and IOP. There was in addition a final follow-up at 1 month to ensure that the eye had recovered completely from surgery, during which the IOP also was checked. Patients who experienced intraoperative complications or were unable to adhere to study protocol were excluded from the study.
Surgical Procedure
After an aseptic technique, under topical anesthesia, a temporal CCI was made using a 2.2-mm metal trapezoidal keratome (ClearCut slit knife, single bevel; Alcon Laboratories, Inc) or a 2.65-mm metal trapezoidal keratome (LaserEdge 2.65-mm angled bevel up; Bausch & Lomb, Inc., Rochester, New York, USA). The keratome size was chosen according to the assigned incision size. Dispersive viscoelastic was injected to fill the anterior chamber followed by circular continuous capsulorrhexis using the Utrata forceps (Rhein Medical Inc., St. Petersburg, Florida, USA). A side port incision was created using a 1.0-mm trapezoidal metal keratome (ClearCut side-port dual bevel angled knife, Alcon Laboratories, Inc). After cortical-cleaving hydrodissection, the nucleus was emulsified using either a stop-and-chop or quick chop technique, depending on the nuclear density. Phacoemulsification through a 2.65-mm incision was performed using the Stellaris system (Bausch & Lomb), and in eyes with a 2.2-mm incision, phacoemulsification was performed using either the Infiniti (Alcon Laboratories, Inc) or Stellaris systems, according to the surgeon’s usual preference. The chopper used was a Nagahara karate chopper (ASICO, LLC., Westmont, Illinois, USA). Cortical material was aspirated, and a single piece hydrophobic acrylic lens (SA60AT; Alcon Laboratories, Inc.) was injected into the capsular bag using a C cartridge and a unihand spring injector. For the 2.2-mm incisions, the bevel of the cartridge was docked at the incision without fully entering the eye (counter-traction technique), whereas for the 2.65-mm incisions, the tip of the cartridge was introduced into the anterior chamber. The viscoelastic material was removed using automated irrigation and aspiration, and the 2 incisions were hydrated. The incisions were checked for leakage before application of antibiotics and steroids (cefazolin, gentamicin, and dexamethasone). Immediately after surgery, tobramycin and betamethasone eye drops were started and instilled every 3 hours for 1 week, then reduced to 4 times daily for 3 weeks.
Anterior Segment Optical Coherence Tomography Evaluation
All the AS OCT images of the main and side port incisions were examined for the presence of wound gape. Both external and internal gapes were recorded, and the extent of nonapposition was recorded as being complete, three quarters, half, one quarter, or less as compared with total incision length. Descemet membrane detachment, when present, also was recorded. The thickness of the main incision was measured at 2, 24, and 96 hours and was expressed as a percentage of the preoperative temporal corneal thickness. The corneal thickness was measured at the midpoint of the incision. The preoperative temporal corneal thickness was calculated by multiplying the nasal corneal thickness measured at 96 hours by a corrective factor. This coefficient is obtained from normative data of the average temporal (655 μm) and nasal (689 μm) peripheral corneal thickness. The equation used is: estimated temporal corneal wound thickness = nasal corneal thickness × 655/689.
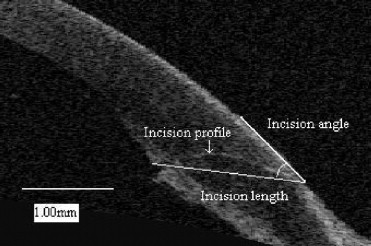
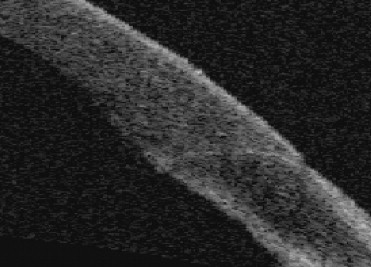
The main wound’s profile also was graded as flat or curved. The angle of the main incision (defined as the angle between the incision and the tangent to the corneal epithelial surface) and the chord lengths of the main and side port incisions were measured at 96 hours using the instrument’s caliper ( Figure 1 ). The incision length of the main wound (measured from the wound entry to its exit point) was adjusted for stromal swelling by using the estimated preoperative temporal corneal thickness. The squareness factor was determined by expressing the incision length as a fraction of the incision width so that a ratio of 1 indicates that the wound is square. A ratio of less than 1 indicates that the wound is rectangular in configuration and is shorter than it is wide. The main wound was defined as having a square configuration if its incision length was within 90% of the width of the keratome used. Statistical analysis was performed using SPSS software version 13.0 (SPSS, Inc., Chicago, Illinois, USA), and statistical significance was set at P < .05.
Results
We recruited 65 patients, of which 5 withdrew from the study for various reasons: intraoperative zonulysis occurred in 1 patient and 4 patients were unwell after surgery, hence, the 2-hour postoperative AS OCT could not be performed. The mean age of the remaining 60 patients (60 eyes) was 66.2 years (standard deviation [SD], 7.3; range, 45.5 to 81.2) and there were 22 males. There was no difference in the proportion of cases with the 2 wound sizes among the 3 surgeons who performed the surgeries. For the 2.2-mm incision, there was no difference in the frequency of the use of the Infiniti or Stellaris systems among the 3 surgeons. There were no significant postoperative complications, including endophthalmitis, in any of the eyes.
Wound Characteristics
Side port incision
All these incisions had a flat profile and their mean incision angle was 40.11 (SD, 5.56 degrees; range, 27.70 to 54.70 degrees). The mean length of the side port incision was 1.43 mm (SD, 0.16 mm; range, 1.08 to 1.91 mm).
Main incision
Descemet membrane detachment was seen in 19 eyes (31.7%) at 2 hours after surgery, of which 8 (26.7%) were in the 2.2-mm incision group and 11 (36.7%) were in the 2.65-mm group. This difference was not statistically significant, and this is not surprising, because the phacoemulsification tips are sized appropriately, and hence wound size should be not be a factor in the occurrence of Descemet detachment. By 96 hours, 9 (47.4%) of the 19 eyes demonstrated spontaneous reattachment: 2 were from the 2.2-mm group and the other 7 were from 2.65 mm group. There was no correlation between the presence of Descemet detachment and mean IOP at all time points.
Wound Gape
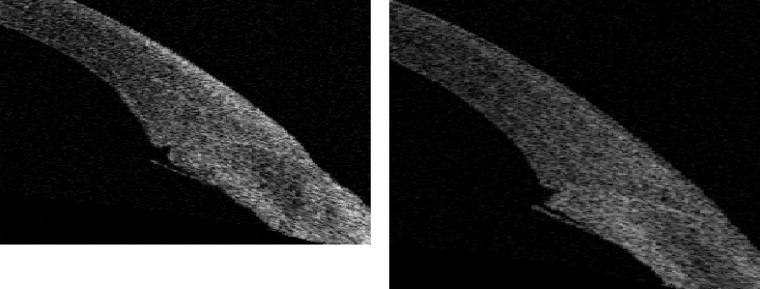
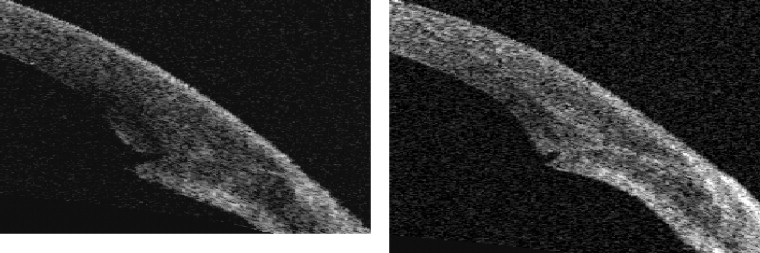
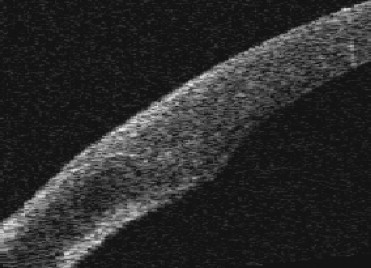
None of the side port incisions gaped. No eyes had gapes of the main incision that involved the entire length of the wound. Gapes were seen only in the internal aspect of the wound, and none were more than 25% of the wound length ( Figures 2 through 5 ). This internal wound gape was seen in 35 eyes (58.3%) at 2 hours after surgery. At 96 hours, 8 (22.9%) had closed. The mean squareness of eyes without internal wound gape at 2 hours (0.66; SD, 0.11) was significantly lower than that of eyes with a wound gape (0.75; SD, 0.14; P = .008, t test; Table 1 ). The area under the receiver operating characteristic curve was 0.70 (95% confidence interval, 0.57 to 0.84; P = .009). A squareness factor of 0.72 or more had a positive predictive value for presence of wound gape at 2 hours of 79.3% and a negative predictive value of 61.3%. There was no correlation between presence of this internal wound gape and the wound size, presence of Descemet membrane detachment, wound swelling at 2 hours, or nucleus density. The IOL insertion technique was not analyzed as a separate variable because this was entirely dependent on the wound size.
| Wound Gape at 2 Hours (35 Eyes) | No Wound Gape at 2 Hours (25 Eyes) | P Value | |
|---|---|---|---|
| Number (%) of eyes with 2.2-mm wound | 19 (54.3) | 11 (44.0) | .43 a |
| Mean percentage of wound swelling at 2 hours | 37.4 | 39.8 | .67 b |
| Standard deviation | 9.8 | 25.1 | |
| Number (%) of eyes with Descemet detachment | 22 (62.9) | 19 (76.0) | .28 a |
| Number (%) of eyes with hard nucleus | 18 (51.4) | 11 (44.0) | .57 a |
| Mean squareness | 0.75 | 0.66 | .008 b |
| Standard deviation | 0.14 | 0.11 | |
| Mean preoperative IOP | 15.10 | 15.00 | .89 b |
| Standard deviation | 2.8 | 3.2 | |
| Mean IOP at 2 hours | 20.9 | 19.5 | .37 b |
| Standard deviation | 7.1 | 4.6 | |
| Mean change in IOP at 2 hours | 5.8 | 4.5 | .47 b |
| Standard deviation | 8.0 | 4.8 |
Wound Leak
At all time points, none of the main wounds had a leak. One side port incision leaked at 2 hours and 24 hours, but was sealed by 96 hours. This occurred in a 72-year-old man whose left eye had crocodile shagreen. The incision was observed to leak when he squeezed his eye, involving less than half the width of the incision. His preoperative IOP was 10 mm Hg. His 2.65-mm wound was sealed during by hydration. No gape was seen on the AS OCT of both the main wound and side port incisions at 2 hours and 24 hours. The IOP at 2 hours was 18 mm Hg (an increase of 8 mm Hg); at 24 hours, it was 18 mm Hg (an increase of 8 mm Hg), and at 96 hours, it was 12 mm Hg (an increase of 2 mm Hg). The angle of the side port incision was 34.9 degrees, and its length was 1.39 mm.
Intraocular Pressure
The mean preoperative IOP was 15.1 mm Hg (range, 10 to 21 mm Hg). The mean postoperative IOP was 20.3 mm Hg (range, 9 to 40 mm Hg), 16.1 mm Hg (range, 8 to 30 mm Hg), 13.7 mm Hg (range, 8 to 20 mm Hg), and 14.3 mm Hg (range, 7 to 21 mm Hg) at 2 hours, 24 hours, 96 hours, and 30 days, respectively. No eye had severe hypotony. The preoperative IOP was found to be correlated with the postoperative pressure change at all time points after surgery, such that eyes with a higher preoperative IOP had a larger reduction in IOP (Pearson correlation at 2 hours, 24 hours, 96 hours, and 30 days: −0.42, P = .001; −0.47, P < .001; −0.61, P < .001; −0.6, P < .001, respectively). The IOP was significantly higher at 2 hours when compared with the preoperative IOP in all eyes and at 24 hours in the eyes with a 2.65-mm wound ( P = .015, paired samples t test) or a hard cataract ( P = .003, paired samples t test; Tables 2 and 3 ). At 96 hours, the IOPs were significantly lower than the preoperative IOP readings for the 2.2-mm group ( P = .006, paired samples t test) or those with a soft nucleus ( P < .001, paired samples t test; Tables 2 and 3 ). By 1 month, the IOPs had returned to baseline values in both groups. The IOP change or IOP at all time points was not correlated with the axial length or wound squareness.
| IOP (mm Hg) | 2.2-mm Wound (30 Eyes) | 2.65-mm Wound (30 Eyes) |
|---|---|---|
| Mean preoperative IOP | 14.6 | 15.5 |
| Standard deviation | 3.2 | 2.8 |
| P value | Not applicable | Not applicable |
| Mean IOP at 2 hours | 21.3 | 19.3 |
| Standard deviation | 6.7 | 5.5 |
| P value | < .001 | .003 |
| Mean IOP at 24 hours | 14.7 | 17.6 |
| Standard deviation | 4.1 | 3.7 |
| P value | .94 | .015 |
| Mean IOP at 96 hours | 12.6 | 14.7 |
| Standard deviation | 2.6 | 2.6 |
| P value | .006 | .15 |
| Mean IOP at 30 days | 13.7 | 14.9 |
| Standard deviation | 2.9 | 3.3 |
| P value | .19 | .42 |
| IOP (mm Hg) | Soft Nucleus (31 Eyes) | Hard Nucleus (29 Eyes) |
|---|---|---|
| Mean preoperative IOP | 15.8 | 14.3 |
| Standard deviation | 3.0 | 2.8 |
| P value | Not applicable | Not applicable |
| Mean IOP at 2 hours | 19.2 | 21.5 |
| Standard deviation | 5.6 | 6.6 |
| P value | .005 | < .001 |
| Mean IOP at 24 hours | 15.6 | 16.7 |
| Standard deviation | 4.2 | 4.0 |
| P value | .86 | .003 |
| Mean IOP at 96 hours | 13.4 | 14.0 |
| Standard deviation | 3.0 | 2.6 |
| P value | < .001 | .63 |
| Mean IOP at 30 days | 14.5 | 14.1 |
| Standard deviation | 3.0 | 3.3 |
| P value | .06 | .79 |
Comparison between 2.2-mm and 2.65-mm Incisions
There were 30 eyes each in the 2.2-mm and 2.65-mm wound groups. Thirty-nine of the incisions had a flat profile and the rest had a curved profile. There was no difference in the proportion of flat and curved profiles or the mean incision angles between the 2 incision sizes. However, the mean incision length of the 2.2-mm wound (1.77 mm; SD, 0.25 mm) was slightly longer than that of the 2.65-mm wound (1.64 mm; SD, 0.22 mm; P = .029, t test), resulting in a greater squareness factor for the 2.2-mm wound (0.81; SD, 0.11; and 0.62; SD, 0.08, respectively; P < .001, t test). The mean IOP was significantly different between the 2 groups at 24 hours and 96 hours, with the 2.65-mm wound having a slightly higher IOP than the 2.2-mm wound at both times ( P = .006 and .003, respectively). The 2.2-mm wound was significantly more swollen at 24 hours than the 2.65-mm wound ( P = .015, t test). There was no correlation between the age; sex; baseline IOP; change from baseline IOP; axial length; wound gape; preoperative temporal corneal thickness; wound swelling at 2, 24, and 96 hours; wound profile; or angle with the incision size. These results are presented in Table 4 .
| IOP (mm Hg) | 2.2-mm Wound (30 Eyes) | 2.65-mm Wound (30 Eyes) | P Value |
|---|---|---|---|
| Mean age (yrs) | 65.6 | 66.9 | .49 a |
| Standard deviation | 7.8 | 6.9 | |
| Males, no. (%) | 9 (30.0) | 13 (43.3) | .28 b |
| Mean baseline IOP | 15 | 16 | .26 a |
| Standard deviation | 3 | 3 | |
| Flat profile, no. (%) | 19 (63.3) | 20 (66.7) | .79 b |
| Mean IOP at 2 hours | 21.3 | 19.3 | .24 a |
| Standard deviation | 6.7 | 5.5 | |
| Mean change in IOP at 2 hours | 6.6 | 3.8 | .11 a |
| Standard deviation | 7.2 | 6.2 | |
| Mean IOP at 24 hours | 14.7 | 17.6 | .006 a |
| Standard deviation | 4.1 | 3.7 | |
| Mean change in IOP at 24 hours | 0.07 | 2.1 | .09 a |
| Standard deviation | 4.7 | 4.4 | |
| Mean IOP at 96 hours | 12.63 | 14.7 | .003 a |
| Standard deviation | 2.6 | 2.6 | |
| Mean change in IOP at 96 hours | −2.0 | −0.8 | .15 a |
| Standard deviation | 3.7 | 2.8 | |
| Mean IOP at 30 days | 13.7 | 14.9 | .17 a |
| Standard deviation | 2.9 | 3.3 | |
| Mean change in IOP at 30 days | −0.9 | −0.6 | .78 a |
| Standard deviation | 3.7 | 4.1 | |
| Wound gape at 24 hours, no. (%) | 16 (53.3) | 14 (46.7) | .61 b |
| Wound gape at 96 hours, no. (%) | 17 (56.7) | 13 (43.3) | .30 b |
| Mean axial length | 23.38 | 23.74 | .22 a |
| Standard deviation | 1.14 | 1.10 | |
| Mean temporal corneal thickness | 0.70 | 0.72 | .36 a |
| Standard deviation | 0.05 | 0.05 | |
| Mean percentage of wound swelling at 2 hours | 42.39 | 34.57 | .15 a |
| Standard deviation | 23.68 | 7.56 | |
| Mean percentage of wound swelling at 24 hours | 37.3 | 31.7 | .015 a |
| Standard deviation | 8.3 | 8.2 | |
| Mean percentage of wound swelling at 96 hours | 33.44 | 31.99 | .59 a |
| Standard deviation | 9.48 | 9.92 | |
| Mean incision angle | 36.01 | 36.28 | .86 a |
| Standard deviation | 5.13 | 6.08 | |
| Mean wound length | 1.77 | 1.64 | .029 a |
| Standard deviation | 0.25 | 0.22 | |
| Number of eyes (%) with square wound | 5 (16.7) | 0 (.0.0) | .052 b |
| Mean squareness of wound | 0.81 | 0.62 | < .001 a |
| Standard deviation | 0.11 | 0.08 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


