Aniridia and Cataracts
Rupal H. Trivedi
M. Edward Wilson
Cataract can be seen in eyes with familial or traumatic aniridia. This chapter discusses mainly the management of familial aniridia; however, some of the principles are useful for traumatic causes of iris loss as well. Cataracts develop in 50% to 85% of patients with familial aniridia, usually during the first two decades of life (Fig. 36.1).1 Netland et al.2 evaluated the prevalence of ocular and systemic abnormalities associated with aniridia in members of Aniridia Foundation International in a survey. Cataract was documented in 71% of respondents. Frequently, small anterior and posterior lens opacities are noted at birth, but these do not usually cause significant visual difficulty. Aniridia was present at birth in all subjects but not diagnosed until a median age of 1.5 months (range, 0-528 months).2 Cortical, subcapsular, and lamellar opacities often develop by the teenage years and may require lens extraction. In those families whose members maintain good vision throughout life, there appears to be a lower incidence of visually significant lens opacities.1 Yoshikawa et al.3 reported a membranous cataract in association with aniridia.
Other clinical features of familial aniridia include the following:
Decreased vision: Even in the absence of cataract, vision is usually in the 20/100 to 20/200 range in patients with aniridia secondary to macular hypoplasia and optic nerve hypoplasia. Although iris hypoplasia is the most common ophthalmic manifestation of the aniridic eye, it is usually not the major determinator of visual function. Poor visual acuity appears to be correlated with absence of the macular reflex, optic nerve hypoplasia, and the development of cataracts, glaucoma, and corneal opacification.
Photophobia: Photophobia may occur secondary to excessive light stimulation because of poor pupillary constriction. A characteristic facial expression in many children consists of narrowing of the palpebral fissures and furrowing of the brow.
Ectopia lentis: Partial dislocation of the lens, usually due to “weak” zonular fibers (due to a molecular defect of the zonule), is more common in aniridic patients. Ectopia lentis has been reported in 0% to 56% of patients with aniridia.1,4
Glaucoma: Glaucoma in infants with aniridia is rare, although it is relatively common later in childhood. Glaucoma was reported in 46% of respondents.2 The median age at diagnosis of glaucoma was 8.5 years (range, 0-58 years).1 Routine gonioscopic examination is important to detect anatomical changes in angle structure that may progress to angle closure. A small stump of iris can gradually produce angle closure by mechanically covering the trabecular meshwork. Patients with more residual iris (often up to where the collarette would be) seem to be at lower risk of glaucoma from this mechanism.
Corneal involvement: Changes in the corneal epithelium occur in all patients with aniridia over time. A superficial, slightly elevated, faint gray pannus with fine radially oriented blood vessels that stain positive with fluorescein is characteristic. Defects appear in the corneal periphery and progress to the center with age. Corneal erosions and frank ulceration occur in some cases. These lesions may progress to end-stage corneal scarring involving all layers. Dry eye was reported to be present in 53% and keratopathy in 45% of respondents.2
Brandt et al.5 reported a markedly increased central corneal thickness in eyes with aniridia. The authors noted an average central corneal thickness at least 100 µm greater than literature-derived normal values.5 This may lead to incorrect estimates of intraocular pressure (IOP) by applanation techniques and highlights the importance of monitoring patients with aniridia for the development of glaucoma by gonioscopy and optic nerve examination. Limbal stem cell transplantation may be considered to help prevent or treat corneal blindness in aniridia.
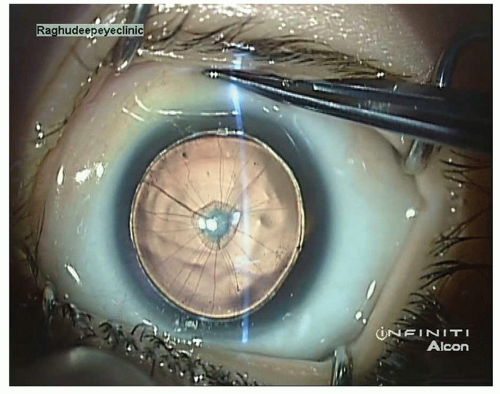 Figure 36.1. Aniridia with anterior polar cataract in a 2-month-old child. (Courtesy Dr. Abhay R. Vasavada and Dr. Sajani Shah, Ahmedabad, India.) |
Optic nerve hypoplasia, strabismus, and nystagmus: Macular hypoplasia is usually accompanied by noticeable optic nerve hypoplasia. Foveal hypoplasia was documented to be present in 41% of respondents and absent in 14%, while 45% were not sure.2
Nystagmus and strabismus are common as well. Nystagmus was reported to be present in 83% of respondents, while strabismus in 31%.2
Hyphema: Theobald et al.6 have published a case report of a 2-month-old infant with known hemophilia A and aniridia who presented with spontaneous hyphema and severe IOP elevation. IOP remained uncontrolled with medical intervention. Anterior chamber washout was performed; at that time, an extensive pupillary plexus was noted over the anterior lens of both eyes, consistent with persistent iris structures associated with aniridia.
Type 2 aniridia with preserved ocular function: One of us (M.E.W.) has reported two cases of so-called “type 2 aniridia with preserved ocular function.”7
Duane retraction syndrome: Association of bilateral Duane syndrome with bilateral aniridia has been recently reported.8
Computed tomography (CT) scan: Mehta et al.9 noted an abnormal lens shape on CT in a patient with aniridia and cataract. The lens shape appeared reversed; that is, the anterior lens surface was more convex and the posterior lens surface less convex.9 A B-mode ultrasound scan showed that the lens capsule shape was normal. In addition, it showed that the cataract was the same shape as the CT image. The CT had imaged the cataract of the patient as opposed to the lens capsule, hence giving the abnormal appearance. The authors cautioned clinicians about misinterpretation when assessing patients with aniridia and cataract by CT scan.9
MANAGEMENT OF ANIRIDIA AND CATARACTS
Detailed preoperative assessment of ocular structures including careful evaluation of the zonular apparatus is essential. In the preoperative assessment of the aniridic patient with a cataract, it is important to attempt to ascertain whether the progressing visual loss arises from increasing lens opacification and not from other factors, such as worsening glaucoma or corneal opacification.10 The guarded prognosis for visual outcome needs to be explained to the patients/parents/legal guardian.
One aspect of an aniridic eye that can be an advantage when performing cataract surgery is that the absence of iris tissue gives better visualization while performing cataract and intraocular lens (IOL) surgery. There are literature reports of thinning of the anterior capsule in association with congenital aniridia.11 However, caution is required, as all aniridic eyes with a thin anterior capsule were in younger patients in the reported series compared with the control group. It is not clear whether younger age or aniridia led to the thinner capsules. Uka et al.12




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
