5 Anesthesia and Patient Positioning
Torsten Birkholz, Martin Marsch
Introduction
Endonasal surgery poses several specific complications in terms of anesthetic management and operative positioning. Adequate analgesia and control of blood pressure and intraoperative bleeding are the main anesthesiological determinants of a successful surgical intervention. Additionally, the method of anesthesia should maintain optimized comfort for the patient and should be cost-effective.
The decision whether to perform local or general anesthesia depends on various factors and should be discussed with the patient on an individual basis.
Topical, infiltrative, or regional anesthesia approaches depend on the patient’s compliance and might involve substantial discomfort from swallowed blood. The surgical field is limited to the regionns reached by infi ltration, nerve block, or topical anesthesia. Accepting these limitations, topical, infiltrative, and regional anesthesia are the most cost-effective methods if they remain free of complications.
Systemic analgosedation performed by the surgeon alone might carry legal risks. Monitored anesthesia care by an anesthesiologist or, if legally permitted, by an anesthesia nurse is to be preferred.
General anesthesia sets no limitation on the surgical field and provides excellent bleeding control and surgical field exposure. Extensive endonasal surgery and teaching surgery should always be performed under general anesthesia. Considerations of patient comfort and surgical safety dictate a preference for general anesthesia as the major anesthetic technique in endonasal surgery.
Topical, Infiltrative, and Regional Anesthesia
Topical analgesia with lidocaine or other aminoamide local anesthetics can be used for limited operations such as hiatotomy, infundibulotomy, or partial anterior and posterior ethmoidectomy. After the application of nebulized local anesthetic, cotton wool carriers with local anesthetic solution can be placed in the middle and upper meatus. The concentration of lidocaine may be up to 4% to reach a sufficient analgetic effect. However, maximum dosages for all anesthetics should be observed. For lidocaine, dosages of 3–4 mg/kg body weight (300 mg) without epinephrine and 7 mg/kg bodyweight with epinephrine 1:200 000 are generally recommended.
Maximum dosages and potential side-effects are matters of particular consideration when using cocaine. Cocaine as a local anesthetic is potent and has positive psychotropic effects, increasing the patient’s surgical tolerance. Its side-effects are potentially dangerous and are related to its sympathomimetic effects. Patients with coronary heart disease, arterial hypertension, cardiac dysrhythmia, or congestive heart failure, those using tricyclic antidepressive drugs or MAO-inhibitors, and former cocaine abusers should be excluded. Topical maximum dosages are 1–2 mg/kg body weight. Use of cocaine demands a more intensive focus on cardiovascular monitoring. The authors recommend standard ECG and noninvasive blood pressure and pulse oximetric monitoring for the use of cocaine. From an anesthesiological point of view, all interventions not attended by an anesthesiologist should nevertheless be accompanied by standard cardiovascular monitoring according to ASA monitoring standards.
Infiltrative anesthesia is usually applied in septal correction surgery, infiltrating the entire septum with lidocaine 1% and epinephrine 1:200 000. The columella and the mucosa of the premaxilla should be infi ltrated to allow the dissection of the basal septum and the hemitransfixation stitch. The addition of epinephrine has two beneficial effects. First, it slows the absorption of the anesthetic agent by constriction of the vascular periphery, and second, it makes both the mucosa and the bone somewhat anemic, thus reducing intrasurgical hemorrhage. Rare complications have been reported, for instance, tissue necrosis or blindness originating from a collateral spasm of the ipsilateral central retinal artery resulting from unintentional injection into one of the greater feeding arteries (Fig. 5.1). Regional anesthesia is an adequate alternative in order to avoid mucosal edema and trauma by infi ltration. Other techniques, such as infiltration of the lateral wall of the inferior meatus and submucosal infiltration of the fossa canina, permit simple antral operations.
Regional anesthesia is characterized by the blockade of nerves, leading to regional analgesia in the nerve’s sensory supply area. Figure 5.2 shows the supply areas of the sensory nerves in the nasal cavity. The ethmoid and middle turbinate region can be satisfactorily anesthetized with 0.3–0.5 mL lidocaine 1% administered to each of the anterior and posterior ethmoidal nerves. The injection is performed into the medial canthus and directed carefully to the shallow grooves representing the entrances of the anterior and posterior ethmoidal nerves (Fig. 5.3a, b).
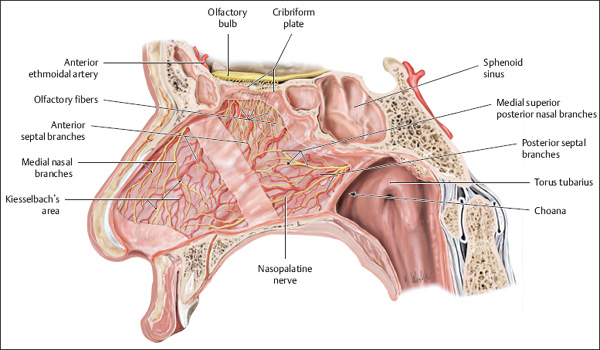

Fig. 5.2 The sensory nerve supply of the lateral nasal wall. (From Thieme Atlas of Anatomy: Head and Neuroanatomy. Stuttgart: Thieme; 2007. Illustrator: K. Wesker.)
During this procedure, close bone contact should be maintained strictly. An additional depot of about 0.5 mL lidocaine 1% is placed at the pterygopalatine foramen. A combination with topical anesthesia is prudent. Additional anesthesia for the maxillary cavity could be provided by the infi ltration of the lateral edge of the posterior choana, directing it toward the pterygopalatine fossa.
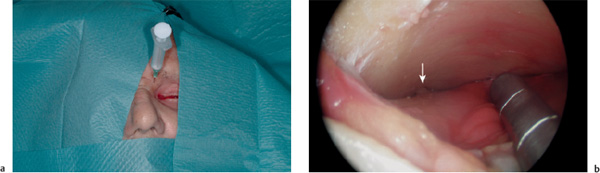
Fig. 5.3 a, b Block anesthesia of the ethmoidal nerves.
a. The syringe in position after probing the entrance of the anterior ethmoidal nerve with the tip of the cannula.
b. Exposure of the shallow funnel of the bone around the nerve’s entrance (arrow) during an external frontal sinusotomy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


