Purpose
To compare concentrations of tear cytokines in 3 groups composed of Sjögren syndrome (SS) dry eye, non–Sjögren syndrome (non-SS) dry eye, and normal subjects. Correlations between ocular surface parameters and tear cytokines were also investigated.
Design
Prospective cross-sectional study.
Methods
SS dry eye patients (n = 24; 40 eyes) were diagnosed with primary SS according to the criteria set by the American-European Consensus Group. Non-SS dry eye patients (n = 25; 40 eyes) and normal subjects (n = 21; 35 eyes) were also enrolled. Tear concentrations of interleukin (IL)-17, IL-6, IL-10, IL-4, IL-2, interferon γ (IFN-γ), and tumor necrosis factor α (TNF-α) were measured by a multiplex immunobead assay. Ocular Surface Disease Index (OSDI), tear film breakup time (TBUT), Schirmer I test, and fluorescein staining scores were obtained from dry eye patients.
Results
All cytokine levels except for IL-2 were highest in the SS group, followed by non-SS dry eye group and control subjects. Concentrations of IL-17, TNF-α, and IL-6 were significantly different among the 3 groups (IL-17: SS > control P < .001, non-SS > control P = .042, SS > non-SS P < .001; TNF-α: SS > control P = .006, non-SS > control P = .034, SS > non-SS P = .029; IL-6: SS > control P = .002, non-SS > control P = .032, SS > non-SS P = .002). IL-17 was significantly correlated with TBUT (R = −0.22, P = .012) and Schirmer I test (R = −0.36, P = .027) scores in the SS group. IL-6 was significantly correlated only with TBUT (R = −0.38, P = .02) in the non-SS group.
Conclusions
Differences in tear cytokine levels and correlation patterns between SS dry eye and non-SS dry eye patients suggest the involvement of different inflammatory processes as causes of dry eye syndrome.
Dry eye syndrome is a common disease. It is associated with discomfort, visual disturbance, and visual loss. Despite the prevalence of this disorder, it has proven difficult to develop an effective treatment because of its resemblance with other ocular surface diseases and anatomic problems, as well as discrepancies between symptoms reported by patients and their doctors’ observations. The general treatment for dry eyes is application of artificial tears. Recently, inflammation has been shown to be an important factor in the pathogenesis of dry eye syndrome. Because inflammation is thought to be responsible for many symptoms, anti-inflammatory therapies including topical corticosteroids, tetracyclines, and topical cyclosporine A are prescribed.
Many studies in regard to inflammatory cytokines and chemokines have evaluated the pathogenesis of dry eyes, as well as possible treatments for the inflammation induced in dry eye syndrome. Recently, interleukin-17 (IL-17), which is produced by a T cell subset, known as T helper type 17 lymphocytes (Th-17), has been studied as a possible connection between inflammation and disruption of the corneal barrier after desiccating stress. Among dry eye subtypes, Sjögren syndrome (SS) dry eye patients are associated with systemic autoimmune disease. Accordingly, tear cytokine levels may vary between SS dry eye and other dry eye subtypes.
In this study, we compared the levels of IL-17 in tears of dry eye syndrome patients and normal subjects. Dry eye syndrome patients were divided into 2 groups: SS dry eye and non–Sjögren syndrome (non-SS) dry eye. In addition to IL-17, interferon γ (IFN-γ), tumor necrosis factor α (TNF-α), IL-10, IL-6, IL-4, and IL-2 were analyzed. Correlations between tear levels of cytokines and severity of clinical signs and symptoms were also analyzed.
Methods
We prospectively analyzed the levels of inflammatory cytokines in tears. Forty eyes of 24 SS dry eye patients and 40 eyes of 25 non-SS dry eye patients were enrolled in the study. Thirty-five eyes of 21 normal subjects were used as controls. This prospective cross-sectional study was approved by the Institutional Review Board (4-2009-0694) of Yonsei University College of Medicine, and informed consent was obtained from all subjects. All SS dry eye patients were diagnosed with primary SS according to the criteria set by the American-European Consensus Group for Sjögren syndrome. Most importantly, the serum antibodies of all SS patients were positive. Because of the unique female-to-male prevalence ratio observed in SS (F:M = 9:1), we included only female patients to prevent misinterpretation of data. To evaluate ocular surfaces and symptoms, we examined tear film breakup time (TBUT), Schirmer I test, corneal and conjunctival staining grade, and Ocular Surface Disease Index (OSDI) in all patients and normal subjects. The Oxford scheme (score 0-5) was used to grade corneal and conjunctival staining.
All dry eye patients had experienced symptoms of dry eyes for more than 6 months and used only artificial tears that did not contain preservatives (topical anti-inflammatory drugs such as 0.05% cyclosporine A or steroids were not used). For inclusion in the dry eye group, patients had to either have undergone corneal and conjunctival staining or have an OSDI over 20, in addition to a TBUT of <5 seconds or a Schirmer I test score of <10 mm. Exclusion criteria included a history of previous ocular surgery, contact lens use, and any ocular surface inflammation or infection not directly related to dry eyes. Patients who demonstrated 2 or more morphologic changes in meibomian glands, including vascular dilation, acinar atrophy, or orifice metaplasia, on the posterior lid margin were also excluded. Normal subjects comprised subjects that were not pregnant, were not on medication (systemic or topical), and did not have a history of contact lens use, as well as exhibited no ocular symptoms or signs such as corneal erosion or corneal staining.
As IL-17 level has been shown to be associated with autoimmune reaction of SS, we measured IL-17 level in 3 study groups. We also measured IFN-γ and IL-2 levels, which are known to be related with T helper 1 (Th1) activation and response. IL-6 and TNF-α, which were shown to be increased in previous studies about cytokine levels of dry eye patients, were also measured. Recently, some studies showed that not only Th1 cytokines but also Th2 cytokines were correlated with SS. Therefore, we assessed and compared IL-4 and IL-10 cytokine levels in tears among study groups.
All examinations were performed on each eye separately and were performed at sufficient time intervals (more than 10 minutes) to minimize the impact of having the same researcher conduct the experiments.
Tear Sample Collection and Analysis
To collect tear samples, 30 μL of phosphate-buffered saline was instilled into the inferior fornix (without topical anesthetics). A total of 20 μL of tear fluid and buffer were collected with a micropipette at the medial and lateral canthus. To minimize ocular surface irritation, we collected the mixture of tear fluid and buffer solution as soon as possible. The fluid was placed into a 1.5-mL Eppendorf tube and stored at −70 C until further examination.
Cytokine concentrations were measured using a multiplex immunobead assay (BDTM Cytometric Bead Array Human Soluble Protein Flex Set; BD Biosciences, San Jose, California, USA) and flow cytometry (BDTM FACS LSR II; BD Biosciences).
Statistical Analysis
Statistical analyses were performed using SPSS for Windows version 15.0 (SPSS Inc. Chicago, Illinois, USA). Cytokine concentrations among the 3 study groups were compared by analysis of variance with Tukey post hoc testing. Correlations between cytokine concentration and clinical parameters (OSDI, TBUT, Schirmer I test, staining grade) were analyzed by Pearson correlation coefficient.
Results
The demographics and clinical features of the SS dry eye group, non-SS dry eye group, and control group are shown in Table 1 . There were no significant differences in mean age among the 3 groups. Between the 2 dry eye groups, there were also no significant differences in mean OSDI, staining grade scale, TBUT, and Schirmer I test.
| Characteristics | Sjören Syndrome Dry Eye | Non–Sjören Syndrome Dry Eye | Control | P Value a (SS vs Non-SS) |
|---|---|---|---|---|
| Number of eyes (OD/OS) | 40 (18/22) | 40 (18/22) | 35 (18/17) | |
| Mean age ± SD (Range) | 55.9 ± 9.96 (37-74) | 55.4 ± 12.44 (32-79) | 52.8 ± 13.19 (37-76) | .984 |
| OSDI (0-100) ± SD | 41.56 ± 23.22 | 33.05 ± 13.67 | 10.48 ± 10.98 | .135 |
| Grade (0-5) ± SD | 1.86 ± 1.4 | 0.8 ± 1.2 | 0 | .198 |
| TBUT(s) ± SD | 3.88 ± 1.98 | 4.56 ± 2.54 | 8.91 ± 3.89 | .52 |
| Schirmer I (mm) ± SD | 4.98 ± 3.12 | 7.12 ± 4.53 | 11.88 ± 6.48 | .291 |
a The mean value was compared by analysis of variance and multiple comparison. We presented P values calculated by Tukey post hoc test between SS dry eye group and non-SS dry eye group.
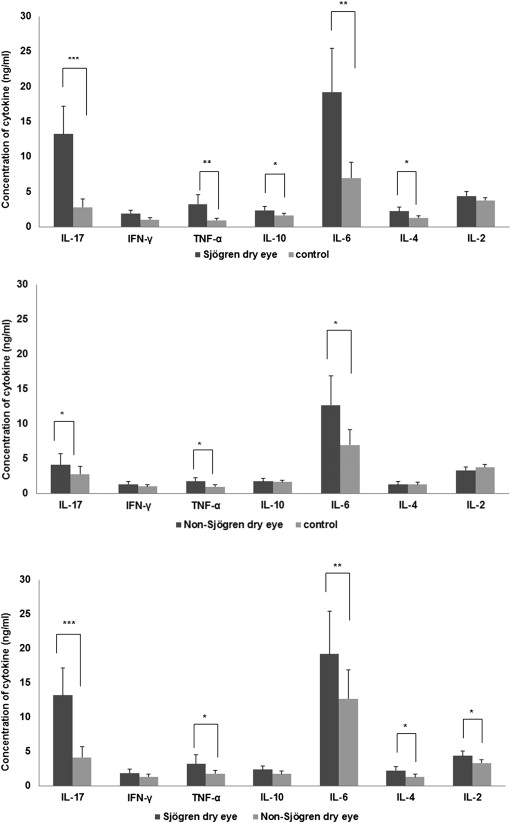
The mean values of cytokine levels in tears are shown in Table 2 . Figure 1 shows the differences in cytokine concentrations among the 3 groups. All of the mean concentrations of tear cytokines in the SS dry eye group were higher than those of the other 2 groups. The mean concentrations of IL-17, TNF-α, IL-10, IL-6, and IL-4 in the SS dry eye group were significantly greater than those in the control group ( Figure 1 , Top, IL-17: P < .001, TNF-α: P = .006, IL-10: P = .049, IL-6: P = .002, IL-4: P = .019). There were also significant differences in IL-17, TNF-α, and IL-6 between the non-SS dry eye group and the control group ( Figure 1 , Middle, IL-17: P = .042, TNF-α: P = .034, IL-6: P = .032). Between the 2 dry eye groups, the mean concentrations of IL-17, TNF-α, IL-6, IL-4, and IL-2 were significantly different ( Figure 1 , Bottom, P value was presented in Table 2 ).
| Cytokine (ng/mL) | Sjören Syndrome Dry Eye | Non–Sjören Syndrome Dry Eye | Control | P Value a (SS vs Non-SS) |
|---|---|---|---|---|
| IL-17 | 13.22 ± 12.7 | 3.99 ± 5.18 | 2.78 ± 3.51 | <.001 |
| IFN-γ | 1.89 ± 1.65 | 1.24 ± 1.30 | 1.00 ± 0.83 | .09 |
| TNF-α | 3.24 ± 4.26 | 1.67 ± 1.46 | 0.95 ± 0.91 | . 029 |
| IL-10 | 2.36 ± 1.67 | 1.70 ± 1.23 | 1.63 ± 0.91 | .074 |
| IL-6 | 19.22 ± 20.11 | 12.12 ± 13.54 | 6.97 ± 6.73 | . 002 |
| IL-4 | 2.23 ± 1.81 | 1.21 ± 1.30 | 1.30 ± 0.98 | .015 |
| IL-2 | 4.38 ± 2.14 | 3.24 ± 1.58 | 3.76 ± 1.30 | .025 |
a The mean value was compared by analysis of variance with Tukey post hoc test. We presented P values only between SS dry eye and non-SS dry eye in this table (by Tukey post hoc test). Significant differences are designated in bold.
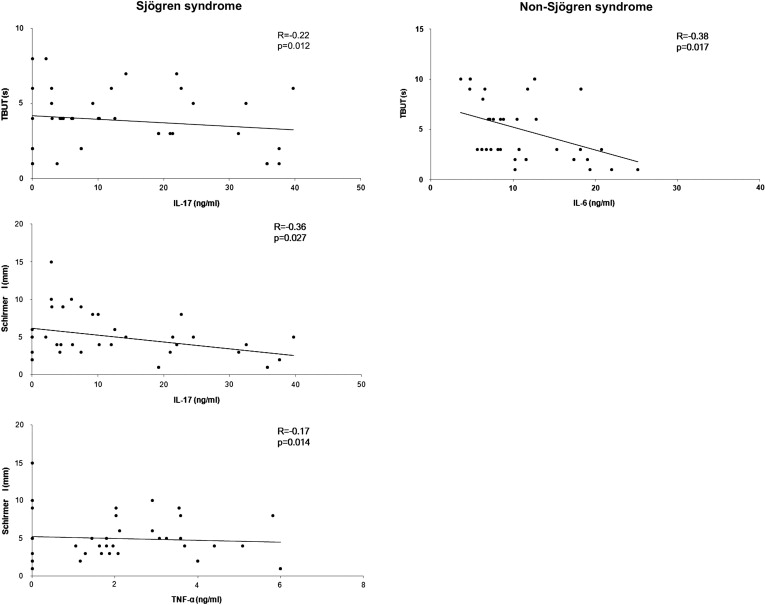
We next investigated correlations between tear cytokines and parameters of ocular surfaces including OSDI, corneal and conjunctival grade, TBUT, and Schirmer I test for the 2 dry eye groups. In the SS dry eye group, only IL-17 and TNF-α levels were significantly correlated with ocular surface parameters. Whereas IL-17 level was shown to be significantly correlated with TBUT and Schirmer I test, TNF-α was only significantly correlated with Schirmer I test ( Figure 2 , IL-17 with TBUT: R = −0.22, P = .012; IL-17 with Schirmer I: R = −0.36, P = .027; TNF-α with Schirmer I: R = −0.17, P = .014). In the non-SS dry eye group, only TBUT and IL-6 level were significantly correlated with ocular surface parameters ( Figure 2 , R = −0.38, P = .017). The other cytokines were not significantly correlated with ocular surface parameters.