Purpose
To bring together information concerning the epidemiology and the economic and individual burdens of glaucoma.
Design
Interpretive essay.
Methods
Review and synthesis of selected literature published from 1991 through December 2010.
Results
An estimated 3% of the global population over 40 years of age currently has glaucoma, the majority of whom are undiagnosed. Vision loss from glaucoma has a significant impact on health-related quality of life even in the early stages of disease. The overall burden increases as glaucomatous damage and vision loss progress. The economic burden of glaucoma is significant and increases as the disease worsens.
Conclusions
Early identification and treatment of patients with glaucoma and those with ocular hypertension at high risk of developing vision loss are likely to reduce an individual’s loss of health-related quality of life as well as the personal and societal economic burdens.
Glaucoma is a group of chronic eye diseases that irreversibly damages the optic nerve and that can result in serious vision loss and blindness. After cataract, it is the second-leading cause of blindness worldwide and is one of the leading causes of preventable blindness.
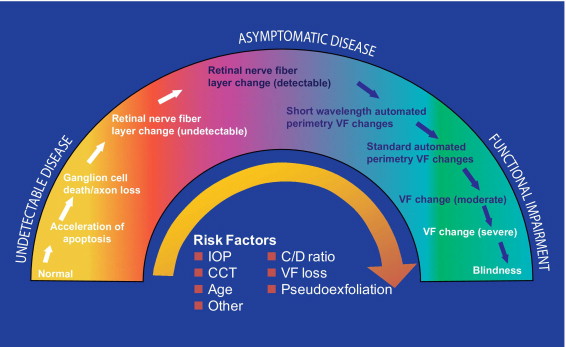
Patients with glaucoma present to eye health professionals with varying severity along a continuum ( Figure 1 ) . Across much of the continuum, glaucoma damage is relatively asymptomatic because of redundancy in the sensory system and the binocular nature of vision; one eye may compensate for early losses in the other. Major risk factors for developing glaucoma include an elevated intraocular pressure (IOP), greater cup-to-disc ratio, thinner central corneal measurement, older age, and family history of glaucoma. These and other risk factors also increase the chance of progressive severe disease.
This essay aims to integrate epidemiologic information with the economic and individual burdens of glaucoma to highlight the impact of glaucoma on individuals, health systems, and societies. We also hope that this information will increase public awareness of glaucoma, will expand professional knowledge of risk factors for visual disability, and will elevate the priority of eye health.
Methods
Publications in English from 1991 through December 2010 on the topics of the epidemiology, economic burden, and individual burden of glaucoma were reviewed. In addition to author identification of important articles, Medline searches (and Embase and IPD for epidemiology) were conducted to identify additional relevant articles using combinations of keywords with “glaucoma” including “prevalence,” “incidence,” “epidemiology,” “cost,” “resource,” and “quality of life.” Searches were intended to serve as the basis for summarizing and integrating important information on the topics of interest and not to meet criteria for a systematic review.
Epidemiology
The prevalence of glaucoma is increasing worldwide ( Figure 2 ) . Globally, an estimated 60.5 million people (2.65% of the global population over 40) suffered from glaucoma in 2010. Of these, an estimated 44.7 million had primary open-angle glaucoma (POAG) and 15.7 million primary angle-closure glaucoma (PACG). The prevalence of glaucoma is expected to reach 79.6 million in 2020, impacting all countries, although the largest increases are expected to be in China and India, which together will represent nearly 40% of cases worldwide. Globally, the number of people with POAG is estimated to reach 58.6 million by 2020, and 21 million will have PACG. More than 4.5 million currently were bilaterally blind from POAG in 2010, a number that is forecasted to rise to 5.9 million by 2020.
The prevalence of glaucoma, which increases with age and varies by ethnicity, is increasing primarily as the population ages. POAG is most prevalent among people of African descent, who have almost 3 times the prevalence compared with white subjects (odds ratio, 2.82; 95% confidence interval [CI], 2.14–3.72). After controlling for age and gender, the prevalence of POAG among Latino/Hispanic subjects is comparable to that among black subjects and 3-fold to 4-fold higher than that observed among white subjects. In contrast, PACG is more prevalent in Asian populations, with Asians representing 87% of those with PACG.
Research in the United States demonstrates the positive relationship between age and prevalence in black, Latino/Hispanic, and white populations. For example, the prevalence of POAG among black women in the Baltimore Eye Survey increased from 2.24% among those aged 50 to 54 years to 5.89% among those aged 70 to 74 years and to 9.82% among those >80 years. Among Latinos/Hispanics in the United States, the prevalence of POAG was 16 times higher among those ≥80 years compared with those aged 40 through 49 years and 13 times higher than those aged 50 through 59.
Because glaucoma frequently is relatively asymptomatic, especially in the early stages, and because there is a low public awareness of glaucoma and its risk factors even in developed societies, the majority of individuals with glaucoma remain undiagnosed ( Figure 3 ) . Many people are not proactive about eye health and remain unaware that they have glaucoma until they experience extensive and usually bilateral visual field loss. Often serendipitous, diagnosis and thus treatment are often delayed. Even among those with diagnosed glaucoma, many do not receive treatment. An analysis of US Medicare claims data from 1992 to 2002 found that an average of 27.4% of beneficiaries with diagnosed POAG did not receive related medical or surgical therapy in a given year.
In summary, glaucoma is a major worldwide epidemiologic challenge; an estimated 3% of the global population over 40 years of age currently have glaucoma, the majority of whom are undiagnosed. The number of cases will rise as the population ages.
Epidemiology
The prevalence of glaucoma is increasing worldwide ( Figure 2 ) . Globally, an estimated 60.5 million people (2.65% of the global population over 40) suffered from glaucoma in 2010. Of these, an estimated 44.7 million had primary open-angle glaucoma (POAG) and 15.7 million primary angle-closure glaucoma (PACG). The prevalence of glaucoma is expected to reach 79.6 million in 2020, impacting all countries, although the largest increases are expected to be in China and India, which together will represent nearly 40% of cases worldwide. Globally, the number of people with POAG is estimated to reach 58.6 million by 2020, and 21 million will have PACG. More than 4.5 million currently were bilaterally blind from POAG in 2010, a number that is forecasted to rise to 5.9 million by 2020.
The prevalence of glaucoma, which increases with age and varies by ethnicity, is increasing primarily as the population ages. POAG is most prevalent among people of African descent, who have almost 3 times the prevalence compared with white subjects (odds ratio, 2.82; 95% confidence interval [CI], 2.14–3.72). After controlling for age and gender, the prevalence of POAG among Latino/Hispanic subjects is comparable to that among black subjects and 3-fold to 4-fold higher than that observed among white subjects. In contrast, PACG is more prevalent in Asian populations, with Asians representing 87% of those with PACG.
Research in the United States demonstrates the positive relationship between age and prevalence in black, Latino/Hispanic, and white populations. For example, the prevalence of POAG among black women in the Baltimore Eye Survey increased from 2.24% among those aged 50 to 54 years to 5.89% among those aged 70 to 74 years and to 9.82% among those >80 years. Among Latinos/Hispanics in the United States, the prevalence of POAG was 16 times higher among those ≥80 years compared with those aged 40 through 49 years and 13 times higher than those aged 50 through 59.
Because glaucoma frequently is relatively asymptomatic, especially in the early stages, and because there is a low public awareness of glaucoma and its risk factors even in developed societies, the majority of individuals with glaucoma remain undiagnosed ( Figure 3 ) . Many people are not proactive about eye health and remain unaware that they have glaucoma until they experience extensive and usually bilateral visual field loss. Often serendipitous, diagnosis and thus treatment are often delayed. Even among those with diagnosed glaucoma, many do not receive treatment. An analysis of US Medicare claims data from 1992 to 2002 found that an average of 27.4% of beneficiaries with diagnosed POAG did not receive related medical or surgical therapy in a given year.
In summary, glaucoma is a major worldwide epidemiologic challenge; an estimated 3% of the global population over 40 years of age currently have glaucoma, the majority of whom are undiagnosed. The number of cases will rise as the population ages.
Economics of Glaucoma
The prevalence of glaucoma contributes to significant costs that are both direct and indirect. Direct medical costs include ocular hypotensive medication(s), physician and hospital visits, and glaucoma-related procedures while direct nonmedical costs include transportation, government purchase programs, guide dogs, and nursing home care. Indirect costs reflect lost productivity, such as days missed from work, and can include the productivity costs borne by caregivers such as family members and friends.
Direct cost estimates for the approximately 2 million US citizens and 300 000 Australian citizens with glaucoma are $2.9 billion and AUS$144.2 million, respectively. However, these figures likely underestimate the true societal costs if all were to be treated, since about half of patients with glaucoma are unaware. A Markov model populated with data based on US Medicare claims data from 1999 to 2005 15 estimated the incremental costs of a case of POAG from the payor’s perspective, including both direct and indirect medical costs. The average lifetime cost of medical treatment in the glaucoma cohort was $1688 greater than in the control cohort without glaucoma over their expected lifetime (mean = 12.3 years). Although the difference between the POAG and control cohorts was not statistically significant, the authors estimated the average annual incremental cost to Medicare attributable to POAG to be approximately $137 per patient per year.
The financial burden of glaucoma increases as disease severity increases ( Figure 4 ) . A US study found a 4-fold increase in direct ophthalmology-related costs as severity increased from asymptomatic ocular hypertension/earliest glaucoma (stage 0) through advanced glaucoma (stage 3) to end-stage glaucoma/blindness (stage 5): average direct costs per patient per year were $623, $1915, and $2511, respectively. The majority of costs were medication-related at all severity stages. A similar trend was seen in Europe, where direct costs of treatment increased by approximately €86 for each incremental increase in glaucoma stage, ranging from €455 per person-year (stage 0) to €969 per person-year (stage 4). Medication costs ranged from 42% to 56% of direct costs at each disease stage. A retrospective medical chart review in the United States (1990 to 2002; n = 151) and Europe (1995 to 2003; n = 194) found that increased annual costs were associated with higher initial IOP level, higher baseline glaucoma stage, use of ocular hypotensive medication, and glaucoma-related surgery.



