Fig. 5.1
Schematic diagram of gas exchange through capillaries in the mucosa lining mastoid air cells
The main cause of adhesive otitis media and cholesteatoma is considered to be the disruption of pressure control in the middle ear cavity. When a new mastoid cavity is formed by tympanoplasty for intractable otitis media, there is no proper gas exchange function that conventional mastoid air cells have. Thus, the results are poor in many cases.
In this study, we created artificial pneumatic air cells and regenerated mastoid air cells using in situ tissue engineering techniques to develop a treatment for intractable otitis media. In situ tissue engineering is a concept based on regenerative medicine. We report here the results.
5.2 Materials and Methods
5.2.1 Materials
Hydroxyapatite was used as a framework for artificial pneumatic bone. This material had a honeycomb-like structure and a high macropore ratio of 90 %, and was composed mainly of calcium phosphate. Its surface was coated with 1 % collagen derived from porcine skin to produce a basic framework for mastoid air cell regeneration. Collagen (Nippon Meat Packers, Inc. Tsukuba, Japan) was extracted using pepsin treatment from porcine skin, and antigens were removed. Its composition was 70–80 % type I collagen and 20–30 % type III collagen (Fig. 5.2a, b). Collagen used in this study had been subjected to viral inactivation and safety tests and approved in March 2002 by the Ethics Committee of Kyoto University Graduate School and Faculty of Medicine. Hydroxyapatite (Pentax, Asahi Optical Co., Ltd. Tokyo, Japan) was the same material used in conventional otologic surgery.
Fig. 5.2
(a) Hydroxyapatite coated with collagen. (b) Scanning electron micrograph of hydroxyapatite coated with collagen. This hydroxyapatite has a high pore ratio. However, each column of hydroxyapatite has no pore and the structure is very dense
5.2.2 Patients
The subjects of this study were 18 patients with severe chronic otitis media (eight men and ten women; mean age: 54.3 years). There were ten patients with cholesteatoma, five patients with cholesteatoma and adhesive otitis media, and three patients with chronic suppurative otitis media. One-stage surgery was performed in one patient (a 5-year-old girl with chronic suppurative otitis media). All other patients received a two-stage surgery. Only patients who received thorough explanation of the content and goals of this study and who provided consent (or whose family provided consent) were selected for the study.
5.2.3 Surgery
5.2.3.1 First Stage of the Surgery
The treatment in the tympanic cavity is the same as in a conventional surgery.
Opening of Mastoid Cavity and Treatment of Cortical Bone
Conventional mastoidectomy was performed in five patients (group I). In 13 other patients (group II), the cortical bone was removed when the mastoid cavity was opened and the cortical bone was harvested as a bony wall. This bony wall was placed back into its original location after treatment in the mastoid cavity was complete, and reconstruction of the cortical bone wall was performed (Fig. 5.3a, b).
Fig. 5.3
(a) Harvesting of cortical bone during antrotomy (first stage of tympanoplasty). For opening the mastoid cavity, a bur was used to make a groove and a flat chisel was used to harvest the cortical bone wall. White arrow: posterior wall of the external auditory meatus, white dotted line: temporal line, asterisk: cortical bone wall. (b) Reconstruction of cortical bone wall during antrotomy (first stage of tympanoplasty). White arrow: posterior wall of the external auditory meatus, white dotted line: temporal line, asterisk: cortical bone wall, white arrow head: drainage tube
The posterior wall of the external auditory meatus was preserved as is in 4 patients with cholesteatoma and three patients with chronic suppurative otitis media (i.e., closed method). In the remaining patients, the posterior wall was temporarily opened and subsequently reconstructed (canal wall down and canal wall reconstruction). The reconstructive material for the posterior wall was a bone pate – a mixture of fragments of autologous cortical bone, bone dust collected when the mastoid cavity was opened, and fibrin glue (Bolheal, Fujisawa Pharmaceutical Co., Ltd. Osaka, Japan).
Implantation of Artificial Pneumatic Bone
In the first stage of tympanoplasty, the artificial pneumatic bone was implanted into the opened mastoid cavity (Fig. 5.4). The artificial pneumatic bone was affixed with fibrin glue. A large silicon sheet recommended by Takahashi et al. was placed, extending from the lumen of the tympanic cavity to the mastoid antrum. [10]. Adhesion of the reconstructed tympanic membrane and the promontory was prevented, and a ventilation pathway was established between the Eustachian tube and the mastoid cavity. In addition, a drain tube of 2–3 mm in diameter was placed to control the pressure in the mastoid cavity and was removed 2–3 weeks after the surgery.
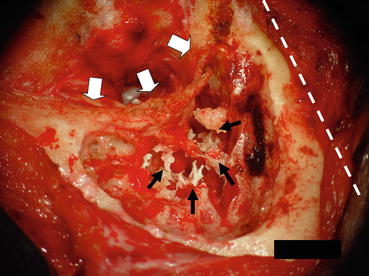
Fig. 5.4
(a) Implanted artificial pneumatic bone (first stage of tympanoplasty). At the first stage of tympanoplasty, finely crushed hydroxyapatite was implanted in the opened mastoid cavity. This hydroxyapatite surface was coated with collagen as in Fig. 5.2. White arrow: posterior wall of the external auditory meatus, white dotted line: temporal line, black arrow: implanted artificial pneumatic bone
5.2.3.2 Second Stage of the Surgery
The second-stage surgery was performed approximately 9 months (mean) after the completion of the first-stage surgery. In the second stage, the mastoid cavity was reopened. Observations were made on the presence or absence of fluid accumulation, invasion of granulation tissue and connective tissue into the cavity, formation of mucosa in the surroundings of the artificial pneumatic bone, and capillary angiogenesis. Subsequently, removal of granulation tissue, connective tissue, and fluid was performed, if present. If the honeycomb-like structure was formed (even partially), then granulation tissue, connective tissue, and fluid were removed while preserving the formed structure. Opening of the mastoid cavity and reconstruction of the cortical bone were performed using the same method as in the first-stage surgery.
5.2.4 Assessment
Postoperative high-resolution CT scans were used to assess the formation of pneumatic space in the mastoid cavity and the regeneration of the honeycomb-like structure. CT scans were taken three times: before the first surgery and before and after the second-stage surgery. In each patient, the final assessment was made using the last CT images taken. The follow-up period was 9–24 months after the second-stage surgery. (The follow-up period was 12 months after surgery for one patient who did not undergo the second-stage surgery.)
5.3 Results
5.3.1 Regeneration of Cortical Bone
In the second-stage surgery, the posterior meatal wall and cortical bone reconstructed in the first-stage surgery were observed to be almost completely regenerated in all patients (Fig. 5.5).
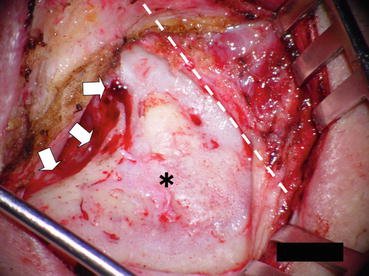
Fig. 5.5
Regenerated cortical bone wall (second stage of tympanoplasty). The findings at the second-stage surgery showed that the cortical bone wall was completely regenerated in the opened mastoid antrum. White arrow: posterior wall of the external auditory meatus, white dotted line: temporal line, asterisk: cortical bone wall
5.3.2 Regeneration of Mastoid Air Cells
In 3 of 17 patients at the second-stage surgery, regeneration of mastoid air cell structure and regeneration of mucosa, including capillaries, were observed such as shown in Figs. 5.6a, b. However, 14 patients had soft tissue or accumulation of effusion in the opened mastoid cavity. In most patients, there was a membrane-like matter that blocked the communication between the mastoid antrum and the tympanic cavity in the surrounding of the attic ad antrum, and accumulation of effusion was observed in the mastoid antrum. There was recurrence of cholesteatoma in the attic in one patient. Fourteen of the eighteen patients (77.8 %) showed at least partial aeration from the attic to the mastoid cavity at the final assessment. Ten of the eighteen patients (55.6 %) showed regeneration of the honeycomb-like structure on CT imaging. The remaining four patients showed aeration mainly in the attic. However, there was opacity of soft tissue (and/or fluid) in the surroundings of the artificial pneumatic bone, and a honeycomb-like structure was not formed. In addition, four patients without any aeration showed opacity of soft tissue (and/or fluid) that filled the entire mastoid cavity. Figure 5.7a, b shows images before and after surgery in a patient with regeneration of mastoid air cells.
Get Clinical Tree app for offline access
Fig. 5.6
(a) Regenerated mastoid air cells (second stage of tympanoplasty). Mastoid air cell structures were formed in the reopened mastoid cavity. (b) Regenerated mastoid air cells (second stage of tympanoplasty). This photo is a high magnification image of (a), showing formation of mucosa with capillaries in the surrounding of the artificial pneumatic bone. White arrows: posterior wall of the external auditory meatus, white dotted line:




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
