Purpose
To investigate the expression of the complement regulatory proteins CD46, CD55, and CD59 on peripheral leukocytes in neovascular age-related macular degeneration (AMD).
Design
Prospective, case-control study.
Methods
Thirty-five unrelated patients with neovascular AMD and 30 control individuals were included in this case-control study. All participants were subjected to a structured interview and detailed imaging (autofluorescence, digital funduscopy, spectral-domain optical coherence tomography, and fluorescein and indocyanine green angiography in patients suspected of having neovascular AMD) was performed. Fresh ethylenediamine-tetraacetic acid blood was obtained and stained with monoclonal antibodies. Using flow cytometry, the percentage of CD14 + monocytes, CD45 + lymphocytes, and CD45 + granulocytes positive for CD46, CD55, and CD59 was determined in patients with neovascular AMD and was compared with that of controls.
Results
We found that the expression of CD46 and CD59 was significantly lower on CD14 + monocytes in patients with neovascular AMD compared with controls ( P = .0070). A significantly lower expression of CD46 on lymphocytes was observed in patients with fibrosis compared with patients without fibrosis ( P = .010).
Conclusions
Our study suggests that neovascular AMD is associated with an inadequate regulation of the complement system, supporting current evidence on the role of complement dysregulation in the pathogenesis of AMD.
Age-related macular degeneration (AMD) represents a leading cause of visual impairment in persons older than 50 years. Vision may be unaffected in the early stages of the disease, which are characterized morphologically by the presence of drusen and changes in the retinal pigment epithelium (RPE). The vision-threatening manifestations of late AMD occur either as a result of choroidal neovascularization (CNV) with or without subretinal fibrosis or from geographic atrophy. Apart from aging and genetic factors, environmental factors, such as smoking, increase the risk of AMD developing. The underlying molecular mechanisms, however, remain incompletely understood. Over the past decade, increasing evidence has implicated inflammation as a contributor in AMD development. Studies of donor eyes with AMD, genetic associations, and plasma levels of complement proteins indicate that complement dysregulation indeed may be a key factor in the pathogenesis of AMD.
The complement system is essential in providing protection from infectious microorganisms through various mechanisms. To avoid collateral damage during a complement attack, autologous cells express a number of complement regulatory proteins (CRegs) on their surfaces. Three proteins of this kind expressed on most cells are CD46 (membrane cofactor protein), CD55 (decay accelerating factor), and CD59 (membrane inhibitor of reactive lysis). Although the differential expression of CRegs in the human eye and in drusen has been studied, very little is known about CRegs on blood cells in patients with AMD. Therefore, we sought to determine whether the expression of CD46, CD55, and CD59 on leukocytes differed in any way in patients with late neovascular AMD compared with controls. Furthermore, we wanted to examine if subretinal fibrosis in AMD was associated with an altered expression of these CRegs, which may provide insight into the pathophysiologic features of subretinal fibrosis. The aim of this study was to investigate the expression of CD46, CD55, and CD59 on leukocytes and to correlate their expression to retinal morphologic features.
Methods
Study Subjects
Sixty-five subjects attending our department of ophthalmology were included in this case-control study over a period of 6 months. Based on the Clinical Age-Related Maculopathy Grading System (CARMS) as proposed by Seddon and associates, subjects were grouped into CARMS grade 1 (no drusen or fewer than 10 small drusen without pigment abnormalities) or CARMS grade 5 (neovascular AMD, including nondrusenoid pigment epithelial detachments, serous retinal detachments, choroidal neovascular membrane with subretinal or sub-RPE hemorrhages or fibrosis). The latter group was subdivided further into patients with and without subretinal fibrosis. Subjects were excluded from the study if they had been diagnosed with inflammatory or autoimmune diseases or cancer, were receiving immune-modulating therapy for any reason, or had received intravitreal anti–vascular endothelial growth factor therapy with ranibizumab within the last 30 days. None of the patients had received or were receiving other forms of anti–vascular endothelial growth factor therapy, for example, bevacizumab.
Clinical Data
All participants underwent a structured interview regarding medical conditions, medication status, and lifestyle (eg, smoking habits), and height and body weight were measured. Subjects were grouped as having arterial hypertension and hyperlipidemia if they had been diagnosed with these conditions earlier or were undergoing treatment for these conditions. Visual acuity was measured according to the Early Treatment Diabetic Retinopathy Study. Depending on their smoking habits, subjects were grouped into current smokers, ever smokers (more than 100 cigarettes during their life), or never smokers. Those who reported quitting within the past year were considered as current smokers.
Retinal Imaging
The retinal diagnosis was made by ophthalmoscopic fundus examination, digital fundus photography (Carl Zeiss, Jena, Germany), autofluorescence imaging (Scanning Laser Ophthalmoscopy, Heidelberg Engineering, Heidelberg, Germany), spectral-domain optical coherence tomography, and indocyanine green imaging (Spectralis HRA-OCT, Heidelberg Engineering, Heidelberg, Germany). Both eyes were examined, and if the CARMS score differed in the 2 eyes, the higher CARMS score (5 being the highest) was chosen. The presence or absence of subretinal fibrosis was assessed in patients with neovascular AMD. Fluorescein angiography was performed after blood sampling to avoid interference in patients suspected of having neovascular AMD. The control group (CARMS 1) consisted of biologically unrelated relatives or patients attending our clinic with a diagnosis other than AMD (eg, cataract).
Leukocyte Preparation and Flow Cytometry
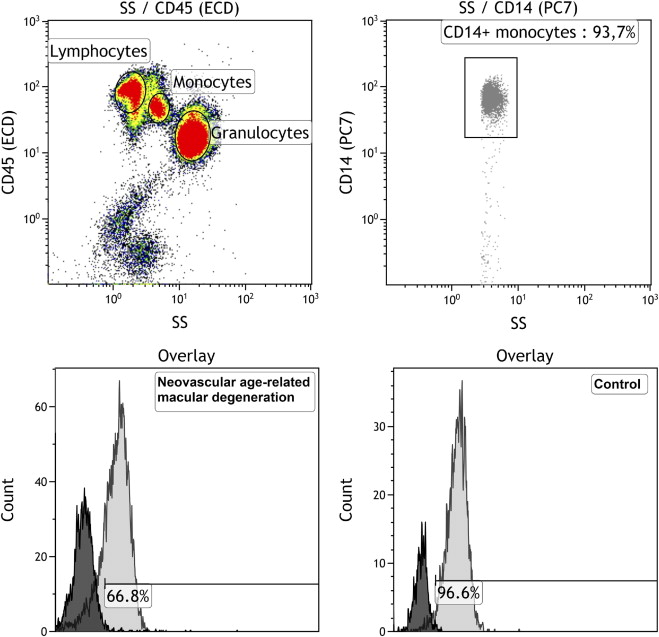
Venous blood samples (3 mL) were obtained from the subjects in tubes containing ethylenediamine-tetraacetic acid anticoagulant, and preparation for flow cytometric analysis was begun within 4 hours after phlebotomy. The volume of blood used for each subject was equivalent to 5 × 10 5 cells and was determined on a prior white blood cell count in a hematology instrument (Sysmex XE-5000 Hematology Analyzer; Sysmex, Kobe, Japan). Red blood cell lysis was performed by adding 10% red blood cell lysis buffer (Nordic Biosite AB, Täby, Sweden) to the whole blood sample for 10 minutes in the dark. The cells were washed 3 times and each time were centrifuged for 5 minutes at 500 g , and finally were resuspended in isotonic buffer (IsoFlow Sheath Fluid; Beckman Coulter, Brea, California, USA). The following specific monoclonal antibodies were added: fluorescein isothiocyanate (FITC)-CD46 (immunoglobulin G2a (IgG2a), clone E4.3; BD Pharmingen, Franklin Lakes, New Jersey, USA), CD59-phycoerythrin (PE) (IgG2a, clone p282 (H19); BD Pharmingen), CD45-electron coupled dye (ECD) (immunoglobulin G1 (IgG1), clone J33; Beckman Coulter), CD55-phycoerythrin-cyanine dye 5 (PE-Cy5) (IgG2a, clone IA10; BD Pharmingen), and phycoerythrin-cyanine dye 7 (PE-Cy7)-CD14 (IgG2a, clone RM052; Beckman Coulter). Corresponding negative isotype controls for IgG2a (FITC, PE, PE-CY5) were used and set at 1%. After incubation at room temperature in the dark, the cells were washed and resuspended in 0.5 mL isotonic buffer. The stained cells (n = 100 000) were analyzed using flow cytometry (FC 500; Beckman Coulter). A side-scatter-CD45 plot was used to gate lymphocytes, monocytes, and granulocytes, and CD14 was used to gate monocytes. Kaluza software version 1.1.11052.10190 (Beckman Coulter) was used to determine the percentage of leukocytes expressing CD46, CD55, and CD59 ( Figure ).
Statistical Analysis
Statistical analysis was performed using the statistical package for the social sciences, Windows version 20 (SPSS Inc, Armonk, New York, USA). Because the data were not normally distributed, the results are expressed in median ± interquartile range. The comparison of the percentage of positive cells for a specific marker between groups was assessed by the Mann–Whitney U test, and the effect of possibly confounding variables (arterial hypertension, hyperlipidemia, body mass index) was tested using multiple regression analysis. The significance level was set to 0.0071 after Bonferroni correction for multiple comparisons (7 tests were performed; 0.05/7 = 0.0071). Because the patients with AMD were somewhat older than the controls (median, 76 years vs. 73 years), the Spearman rank correlation was performed to see if any differences noted between the groups could be attributed to age differences.
Results
The study population included 35 patients with neovascular AMD (CARMS grade 5) and 30 age-matched control individuals (CARMS grade 1; Table 1 ). In the AMD group, 24 (73%) patients had some degree of subretinal fibrosis. The neovascular AMD group consisted of 20 females and 15 males with a median age of 76 years (range, 63 to 89 years). The control group consisted of 14 females and 16 males with a mean age of 73 years (range, 60 to 86 years). The percentage of never smokers and ever smokers was similar in both groups; however, there were 10 (29%) active smokers in the neovascular AMD group compared with no active smokers in the control group. The body mass index was similar in both groups. In the neovascular AMD group, 23 (66%) subjects had arterial hypertension and 13 (37%) had hyperlipidemia, compared with 13 (43%) and 5 (17%) in the control group, respectively ( Table 1 ).
| Neovascular Age-Related Macular Degeneration (n = 35) | Controls (n = 30) | P Value | |
|---|---|---|---|
| Median age (range), y | 76 (63 to 89) | 73 (60 to 86) | .05 |
| Smoking history, n (%) | |||
| Never smoker | 13 (37%) | 16 (53%) | .20 |
| Ever smoker | 12 (34%) | 14 (47%) | .32 |
| Active smoker | 10 (29%) | 0 | < .001 |
| Gender, n (%) | |||
| Male | 16 (46%) | 16 (53%) | .55 |
| Female | 19 (54%) | 14 (47%) | .55 |
| Risk factors | |||
| Arterial hypertension, n (%) | 23 (66%) | 13 (43%) | .07 |
| Hyperlipidemia, n (%) | 13 (37%) | 5 (17%) | .07 |
| Body mass index (range), kg/m 2 | 26.8 (20.4 to 41.3) | 27.7 (20.8 to 38.7) | .43 |
Subjects with neovascular AMD had significantly lower expression of CD46 ( P = .0070, Mann–Whitney U test) and CD59 ( P = .0070, Mann–Whitney U test) on CD14 + monocytes as compared with control subjects without AMD ( Table 2 ). There was a tendency toward lower expression of CD59 on lymphocytes ( P = .071). The median expression of CD55 on monocytes and granulocytes was 100% in all subjects and hence was excluded from analysis. CD55 expression on lymphocytes did not differ in the 2 groups ( Table 2 ). The differences in expression on leukocytes were not related to the absolute leukocyte count ( Table 2 ). The intergroup variation in expression of CD46 and CD59 was not attributable to age differences between the groups ( P = .19 and ρ = 0.16, P = .21 and ρ = 0.16, Spearman rank correlation).
| Neovascular Age-Related Macular Degeneration | Controls | P Value | |
|---|---|---|---|
| CD46 | |||
| CD14 + monocytes (%) | 67 a (40 to 92); 0.39 | 90 (62 to 99); 0.46 | .0070 |
| CD45 + lymphocytes (%) | 58 (36 to 73); 0.94 | 68 (36 to 82); 0.97 | .31 |
| CD45 + granulocytes (%) | 99 (92 to 100); 4.51 | 99 (92 to 100); 3.44 | .66 |
| CD55 | |||
| CD45 + lymphocytes (%) | 66 (55 to 73); 1.10 | 61 (5 to 78); 0.96 | .35 |
| CD59 | |||
| CD14 + monocytes (%) | 29 a (9 to 88); 0.21 | 77.5 (51 to 98); 0.40 | .0070 |
| CD45 + lymphocyte (%) | 38 (3 to 67); 0.61 | 61 (5 to 78); 0.77 | .07 |
| CD45 + granulocytes (%) | 72 (12 to 95); 0.72 | 84 (9 to 99); 2.13 | .35 |
In the neovascular AMD group, patients with subretinal fibrosis had significantly lower expression of CD46 on lymphocytes as compared with patients with neovascular AMD without subretinal fibrosis ( P = .01; Table 3 ). Thus, we tested the expression of CD46 on CD14 + monocytes and granulocytes, but found no association with fibrosis, although there was a tendency toward lower expression of CD46 on CD14 + monocytes ( Table 3 ).



