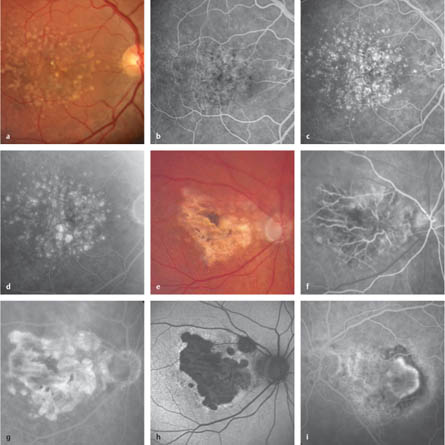
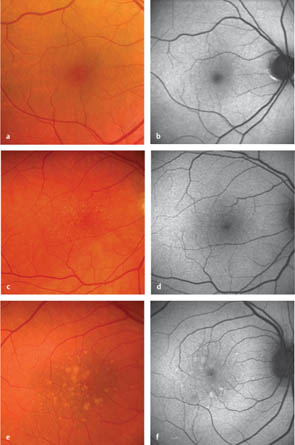
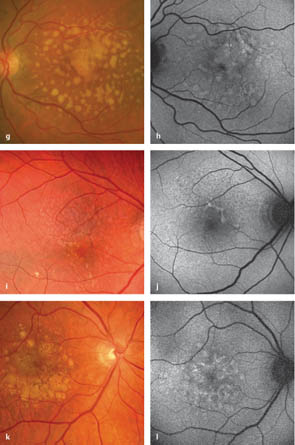
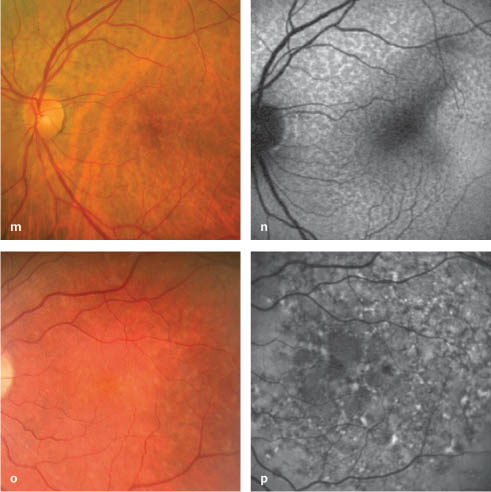
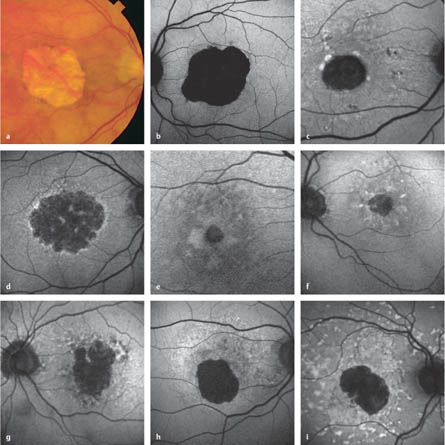
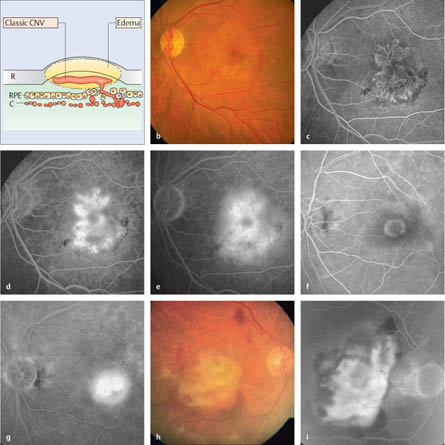
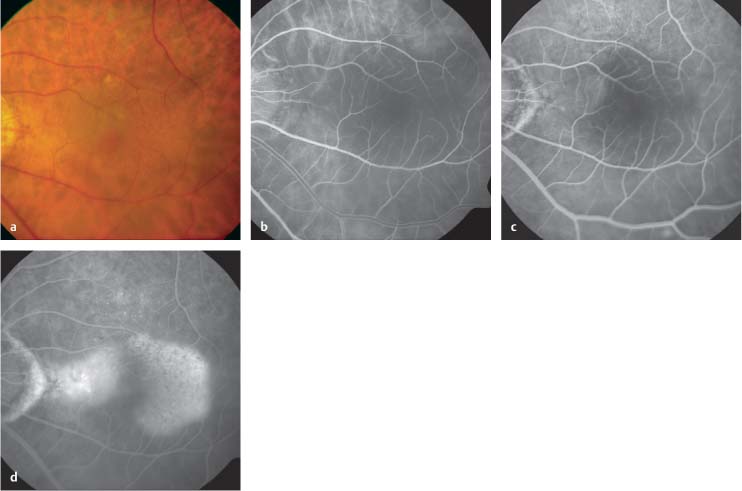
3.1 Classification of Age-Related Macular Disease Bird AC. Age-related macular disease. Br J Ophthalmol 1996;80:1–2. Bird AC, Bressler NM, Bressler SB, et al. An international classification and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemiological Study Group. Surv Ophthalmol 1995;39:367–74. Haines JL, Hauser MA, Schmidt S, et al. Complement factor H variant increases the risk of age-related macular degeneration. Science 2005;308:419–21. Klein R, Peto T, Bird A, Vannekirk MR. The epidemiology of age-related macular disease. Am J Ophthalmol 2004;137:486–95. Rivera A, Fisher SA, Fritsche LG, et al. Hypothetical LOC387715 is a second major susceptibility gene for age-related macular degeneration, contributing independently of complement factor H to disease risk. Hum Mol Genet 2005;14:3227–36. Thornton J, Edwards R, Mitchell P, et al. Smoking and age-related macular degeneration: a review of association. Eye 2005;19: 935–44. Fig. 3.1a–i Age-related macular disease (AMD) a Color photograph. Age-related maculopathy, with soft and hard drusen presenting as yellow–white subretinal deposits. b Early phase. Temporal to the fovea, the hard drusen can be distinguished as small, well-defined, hyperfluorescent lesions. c Late arteriovenous phase. The hard drusen have reached maximum hyperfluorescence and are clearly distinguishable. The soft drusen have become more visible, with less distinct borders. d Late phase. Hyperfluorescence in the area of the soft drusen persists without any leakage; the hyperfluorescence of the hard drusen is barely recognizable. e Color photograph. Geographic atrophy with satellite lesions and pigment clumping, as well as reactive changes in the retinal pigment epithelium. f Arterial phase. Early filling of the remaining large, deep choroid vessels can be seen as a result of a window defect arising from the loss of the retinal pigment epithelium and choriocapillaris. g Late phase. Increasing hyperfluorescence in the atrophic area can be seen, concealing the view of the large choroidal vessels. This area of hyperfluorescence has its origins in the hyperfluorescence of the sclera and the window defect as a result of the retinal pigment epithelium atrophy. No leakage is displayed. h Fundus autofluorescence. The regions with retinal pigment epithelium atrophy show an absence of autofluorescence. i Fluorescein angiography (in a different patient). Choroidal neovascularization (CNV) after photodynamic therapy. The CNV vessels show hyperfluorescence in the early stage of angiography. Age-Related Eye Disease Study Research Group. A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 2001;119:1417–36. Bindewald A, Bird AC, Dandekar SS. Classification of fundus autofluorescence patterns in early age-related macular disease. Invest Ophthalmol Vis Sci 2005, 46:3309–14. Einbock W, Moessner A, Schnurrbusch UE, Holz FG, Wolf S, FAM Study Group. Changes in fundus autofluorescence in patients with age-related maculopathy. Correlation to visual function: a prospective study. Graefes Arch Clin Exp Ophthalmol 2005;243: 300–5. Holz FG, Wolfensberger TJ, Piguet B, et al. Bilateral macular drusen in age-related macular degeneration: prognosis and risk factors. Ophthalmology 1994;101:1522–8. Hsu J, Maguire MG, Fine SL. Laser prophylaxis for age-related macular degeneration. Can J Ophthalmol 2005;40:320–31. Sarks JP, Sarks SH, Killingsworth MC. Evolution of soft drusen in age-related macular degeneration. Eye 1994;8:269–83. Fig. 3.2a–f Age-related maculopathy. Classification of fundus autofluorescence patterns in early age-related macular disease (reproduced with permission from Bindewald et al., Invest Ophthalmol Vis Sci 2005;46:3309–14) a, b Normal pattern. Homogeneous background fluorescence and a gradual decrease in the inner macula toward the fovea (b). Only small hard drusen are visible in the fundus photograph (a). c, d Minimal change pattern. Limited minimal increase or decrease in the intensity of the autofluorescence (d) due to multiple small hard drusen (c). e, f Focally increased pattern. Several well-defined spots with markedly increased autofluorescence (f) in an eye with multiple soft and hard drusen (e). Fig. 3.2g–l g, h Patchy pattern. Multiple large areas (> 200 μm in diameter) of increased autofluorescence (h), corresponding to large soft drusen and/or hyperpigmentation (g). i, j Linear pattern. At least one linear area with markedly increased autofluorescence (j), corresponding to a hyperpigmented line (i). k, l Lace-like pattern. Multiple branching structures of increased autofluorescence (l), corresponding to hyperpigmentation or no visible abnormality on ophthalmoscopy (k). Fig. 3.2m–p m, n Reticular pattern. Multiple specific areas of decreased autofluorescence with brighter lines in between (n) may correspond to reticular drusen (m). o, p Speckled pattern. A variety of autofluorescence abnormalities (p), whereas the color photograph shows fewer pathological areas (o). Bellmann C, Jorzik J, Spital G, et al. Symmetry of bilateral lesions in geographic atrophy in patients with age-related macular degeneration. Arch Ophthalmol 2002;120:579–84. Bindewald A, Schmitz-Valckenberg S, Jorzik JJ, et al. Classification of abnormal fundus autofluorescence patterns in the junctional zone of geographic atrophy in patients with age-related macular degeneration. Br J Ophthalmol 2005;89:874–8. Cahill MT, Mruthyunjaya P, Bowes Rickman C, Toth CA. Recurrence of retinal pigment epithelial changes after macular translocation with 360 degrees peripheral retinectomy for geographic atrophy. Arch Ophthalmol 2005;123:935–8. Green WR, Enger C. Age-related macular degeneration histopathologic studies. The 1992 Lorenz E. Zimmerman Lecture. Ophthalmology 1993;100:1519–35. Schmitz-Falkenberg S, Bültmann S, Bindewald A, et al. Fundus autofluorescence and fundus perimetry in the junctional zone of geographic atrophy in patients with age-related macular degeneration. Invest Ophthalmol Vis Sci 2005;45:4470–6. Sunness JS. The natural history of geographic atrophy, the advanced atrophic form of age-related macular degeneration. Mol Vis 1999;5:25–9. Fig. 3.3a–i Geographic atrophy. Classification of abnormal fundus autofluorescence patterns in the junctional zone of geographic atrophy (Figs. 3.3b–I reproduced with permission from Bindewald et al., Br J Ophthalmol 2005;89:874–8) a Fluorescein angiography. Advanced geographic atrophy. The large choroid vessels are visible through the window defect in the retinal pigment epithelium. b Normal fundus autofluorescence in the junctional zone. c Multiple patches of markedly focal increased fundus autofluorescence. d A band of increased fundus autofluorescence surrounding the geographic atrophy. e Larger areas of patchy increased fundus autofluorescence outside the area of geographic atrophy. f Diffuse types of increased fundus autofluorescence in the junctional zone of geographic atrophy. Type A: reticular pattern with a preferred radial orientation. g Type B: increased fundus autofluorescence with short branching linear features. h Type C: diffusely increased fundus autofluorescence with a fine granular-like appearance surrounding the geographic atrophy. i Type D: diffusely increased fundus autofluorescence with a fine granular appearance surrounding the geographic atrophy, and peripheral elongated small lesions with increased fundus autofluorescence. Barbazetto I, Burdan A, Bressler NM, et al. Photodynamic therapy of subfoveal choroidal neovascularization with verteporfin: fluorescein angiographic guidelines for evaluation and treatment—TAP and VIP report no. 2. Arch Ophthalmol 2003;121:1253–68. Grossniklaus HE, Gass JD. Clinicopathologic correlations of surgically excised type 1 and type 2 submacular choroidal neovascular membranes. Am J Ophthalmol 1998;126:59–69. Krebs I, Binder S, Stolba U, et al. Optical coherence tomography guided retreatment of photodynamic therapy. Br J Ophthalmol 2005;89:1184–7. Lafaut BA. Clinicopathologic correlation of surgically removed submacular tissue. Bull Soc Belge Ophtalmol 2000; (278):49–53. Michel S, Wachtlin J, Gamulescu MA, et al. Comparison of early retreatment with the standard regimen in verteporfin therapy of neovascular age-related macular degeneration. Ophthalmology 2005;112:2070–5. Sarks SH. New vessel formation beneath the retinal pigment epithelium in senile eyes. Br J Ophthalmol 1973;57:951–65. Fig. 3.4a–i Classic choroidal neovascularization a Schematic representation of the position of a classic choroidal neovascularization between the neuroretina and the retinal pigment epithelium. R, retina; RPE, retinal pigment epithelium; C, choroid. b Color photograph. The choroidal neovascularization is difficult to identify, and has the appearance of a light gray coloring in the foveal area. Some blood and several drusen are also visible. c Early arteriovenous phase. The vessel network of the classic choroidal neovascularization appears as an early, well-defined and demarcated hyperfluorescence. It also features several small areas of hypofluorescence resulting from blockage of fluorescence from hemorrhage and hard drusen. d Late arteriovenous phase. There is a marked increase in hyper-fluorescence in the area of the choroidal neovascularization. e Late phase. Leakage from the choroidal neovascularization. Fluorescein is flowing out of the vessels, and the area of increasing leakage extends beyond the vessel network that was visible in the early phase. f Early arteriovenous phase. Another example of a classic choroidal neovascularization, consisting of a well-demarcated, homogeneous early hyperfluorescence. However, the vessel loops are not identifiable. g Late phase. Clear leakage from the choroidal neovascularization is seen. h Color photograph. The late stage of untreated exudative age-related macular degeneration. An extended disciform scar has formed, with subretinal fibrosis and hemorrhage. i Late phase. Leakage and staining in the area of the extended fibrosis. This angiogram is not necessary, as the diagnosis could have been established clinically and angiography has no implications for treatment. Two types of occult CNV are differentiated angiographically in the Macular Photocoagulation Study (MPS) classification: – Fibrovascular pigment epithelial detachment is the most common form of occult CNV. – An irregular elevation of the RPE can be found (stereoscopic fluorescein angiography). – In the first few minutes, an inhomogeneous, irregular, increasing hyperfluorescence (“stippled” hyper-fluorescence) develops. Subsequently, an increase of hyperfluorescence can be observed (in 5th to 10th minutes). – A notch on the edge of an RPE detachment is not a criterion for an occult CNV according to the MPS criteria. However, it does often correlate with the location of an occult CNV. – This type is diagnosed more rarely (partly because of the milder loss of visual acuity, with less exudation) and is more often overlooked as a component of the lesion. There is no RPE detachment. – No fluorescein angiographic correlation in the early phase is seen with the late hyperfluorescence. – An irregular, inhomogeneous hyperfluorescence can be seen that increases during the late phase of the angiogram. – It is often difficult to differentiate between these types of CNV on the basis of an irregular late hyper-fluorescence observed around the CNV lesion after photodynamic therapy (PDT). Additional terminology used in the analysis of CNVs includes the following terms (MPS group and participants in the Verteporfin Round Table): Barbazetto I, Burdan A, Bressler NM, et al. Photodynamic therapy of subfoveal choroidal neovascularization with verteporfin: fluorescein angiographic guidelines for evaluation and treatment—TAP and VIP report no. 2. Arch Ophthalmol 2003;121:1253–68. Bressler NM, Frost LA, Bressler SB, Murphy RP, Fine SL. Natural course of poorly defined choroidal neovascularization associated with macular degeneration. Arch Ophthalmol 1988;106:1537–42. Freund KB, Yannuzzi LA, Sorenson JA. Age-related macular degeneration and choroidal neovascularization. Am J Ophthalmol 1993;115:786–91. Fig. 3.5a–d Occult choroidal neovascularization, type 1 (fibrovascular pigment epithelial detachment) a Color photograph. A flat pigment epithelial detachment is visible in the area of the macula. b Early arteriovenous phase. An area of hypofluorescence corresponding to the clinically detected fibrovascular pigment epithelial detachment is visible. In contrast to classic choroidal neovascularization, early well-defined hypofluorescence is not seen. c
Definitions and Classification
 Different terms are used to identify subgroups of patients with age-related macular disease.
Different terms are used to identify subgroups of patients with age-related macular disease.
 Age-related macular disease can be subdivided into early and late stages. The early stages present with development of drusen and hyperpigmentation or hypopigmentation of the retinal pigment epithelium. Late stages with severe visual loss include the development of choroidal neovascularization (CNV), pigment epithelial detachment, subretinal hemorrhage, or geographic atrophy.
Age-related macular disease can be subdivided into early and late stages. The early stages present with development of drusen and hyperpigmentation or hypopigmentation of the retinal pigment epithelium. Late stages with severe visual loss include the development of choroidal neovascularization (CNV), pigment epithelial detachment, subretinal hemorrhage, or geographic atrophy.
 The early stages have been termed age-related maculopathy (ARM) in contrast to the late stages, which are known as age-related macular degeneration (AMD or ARMD). The acronyms AMD and ARMD are used for both age-related macular disease and for age-related macular degeneration.
The early stages have been termed age-related maculopathy (ARM) in contrast to the late stages, which are known as age-related macular degeneration (AMD or ARMD). The acronyms AMD and ARMD are used for both age-related macular disease and for age-related macular degeneration.
 The late stages have also often been subdivided into a nonexudative or “dry” form, corresponding to geographic atrophy, and an exudative or “wet” form, including CNV, pigment epithelial detachment, and associated subretinal hemorrhage.
The late stages have also often been subdivided into a nonexudative or “dry” form, corresponding to geographic atrophy, and an exudative or “wet” form, including CNV, pigment epithelial detachment, and associated subretinal hemorrhage.
 Drusen as a major indicator of age-related macular disease have been subdivided into well-defined “hard” drusen and less distinct “soft” drusen, which are distinguished by size.
Drusen as a major indicator of age-related macular disease have been subdivided into well-defined “hard” drusen and less distinct “soft” drusen, which are distinguished by size.
 CNVs are differentiated into classic or occult, on the basis of the fluorescein-angiographic findings in the early phases of the angiogram.
CNVs are differentiated into classic or occult, on the basis of the fluorescein-angiographic findings in the early phases of the angiogram.
Epidemiology, Pathophysiology, and Clinical Presentation
 Age-related macular disease is the most prevalent form of macular disease in the elderly and is the leading cause of blindness in people over the age of 50 in industrialized countries.
Age-related macular disease is the most prevalent form of macular disease in the elderly and is the leading cause of blindness in people over the age of 50 in industrialized countries.
 The incidence and prevalence of different stages of age-related macular disease have been established in large population-based studies conducted in the USA, the Netherlands, and Australia.
The incidence and prevalence of different stages of age-related macular disease have been established in large population-based studies conducted in the USA, the Netherlands, and Australia.
 In large epidemiological studies, the prevalence of age-related macular degeneration is reported to range from approximately 0.2% in patients aged 55–64 up to 11% in those over 85. Age-related maculopathy is 4–10 times more common, depending on age.
In large epidemiological studies, the prevalence of age-related macular degeneration is reported to range from approximately 0.2% in patients aged 55–64 up to 11% in those over 85. Age-related maculopathy is 4–10 times more common, depending on age.
 Visual loss develops in the late stages in approximately 85% of nonexudative lesions and 15% of exudative lesions.
Visual loss develops in the late stages in approximately 85% of nonexudative lesions and 15% of exudative lesions.
 Risk factors consistently found in these studies are increasing age, a positive family history, and smoking—the latter being the only risk factor capable of being influenced. The potential influence of other factors such as nutrition or cataract surgery is a matter of debate.
Risk factors consistently found in these studies are increasing age, a positive family history, and smoking—the latter being the only risk factor capable of being influenced. The potential influence of other factors such as nutrition or cataract surgery is a matter of debate.
 Genetic predisposition has been suspected on the basis of family and twin studies. Recently, polymorphisms in the CHF gene and the LOC387715 gene have been identified that are associated with an increased risk of age-related macular disease.
Genetic predisposition has been suspected on the basis of family and twin studies. Recently, polymorphisms in the CHF gene and the LOC387715 gene have been identified that are associated with an increased risk of age-related macular disease.
 The pathophysiology has not yet been completely clarified. A multifactorial process influenced by aging leads to dysfunction of the functional complex of photo-receptors, retinal pigment epithelium, and Bruch membrane.
The pathophysiology has not yet been completely clarified. A multifactorial process influenced by aging leads to dysfunction of the functional complex of photo-receptors, retinal pigment epithelium, and Bruch membrane.
 The classic symptoms are deterioration in visual acuity and metamorphopsia.
The classic symptoms are deterioration in visual acuity and metamorphopsia.
 The process leads to an extensive central scotoma and the development of paracentral fixation. Reading and recognition of faces are no longer possible.
The process leads to an extensive central scotoma and the development of paracentral fixation. Reading and recognition of faces are no longer possible.
 If only one eye is affected, the healthy eye will compensate for the deficiency in the diseased eye, so that the condition in the affected eye is often only discovered incidentally.
If only one eye is affected, the healthy eye will compensate for the deficiency in the diseased eye, so that the condition in the affected eye is often only discovered incidentally.
 The decline of visual function takes place significantly more quickly in exudative age-related macular degeneration than in the nonexudative form.
The decline of visual function takes place significantly more quickly in exudative age-related macular degeneration than in the nonexudative form.
 Peripheral vision is usually preserved, and spatial orientation is also possible in the late phases of the disease.
Peripheral vision is usually preserved, and spatial orientation is also possible in the late phases of the disease.
 About 30% of patients with advanced AMD suffer depression, an aspect that is commonly underestimated.
About 30% of patients with advanced AMD suffer depression, an aspect that is commonly underestimated.
Diagnosis and Treatment
 The diagnosis is established by ophthalmoscopy. Fluorescein angiography makes it possible to differentiate most forms of age-related macular disease and is mandatory for many treatment decisions. Fundus autofluorescence, optical coherence tomography, and indocyanine angiography provide additional information for subclassifying the disease, taking decisions regarding treatment, and establishing the follow-up procedures required.
The diagnosis is established by ophthalmoscopy. Fluorescein angiography makes it possible to differentiate most forms of age-related macular disease and is mandatory for many treatment decisions. Fundus autofluorescence, optical coherence tomography, and indocyanine angiography provide additional information for subclassifying the disease, taking decisions regarding treatment, and establishing the follow-up procedures required.
 Amsler grid tests can be used for self-screening.
Amsler grid tests can be used for self-screening.
 Treatment options are stage-dependent and include substitution of nutrients, laser coagulation, photodynamic therapy, macular surgery, intravitreal injection of drugs, and low-vision aids.
Treatment options are stage-dependent and include substitution of nutrients, laser coagulation, photodynamic therapy, macular surgery, intravitreal injection of drugs, and low-vision aids.
 Affected patients and family members at risk should be advised to stop smoking.
Affected patients and family members at risk should be advised to stop smoking.
References
3.2 Age-Related Maculopathy
Epidemiology, Pathophysiology, and Clinical Presentation
 Age-related maculopathy (ARM) is the precursor of age-related macular degeneration (AMD). It is important to identify patients with ARM in order to start prophylactic treatment when appropriate and to inform patients about the symptoms of advanced AMD in order to start treatment as early as possible.
Age-related maculopathy (ARM) is the precursor of age-related macular degeneration (AMD). It is important to identify patients with ARM in order to start prophylactic treatment when appropriate and to inform patients about the symptoms of advanced AMD in order to start treatment as early as possible.
 Drusen are accumulations of protein and lipid-containing amorphous material between the retinal pigment epithelium (RPE) and Bruch membrane.
Drusen are accumulations of protein and lipid-containing amorphous material between the retinal pigment epithelium (RPE) and Bruch membrane.
 On ophthalmoscopy, drusen are visualized as small yellow or white subretinal lesions. A distinction is made between hard and soft varieties of drusen, and mixed forms can also appear. Soft drusen are larger than 65 μm (half the diameter of a vein at the edge of the papilla), and hard drusen are smaller.
On ophthalmoscopy, drusen are visualized as small yellow or white subretinal lesions. A distinction is made between hard and soft varieties of drusen, and mixed forms can also appear. Soft drusen are larger than 65 μm (half the diameter of a vein at the edge of the papilla), and hard drusen are smaller.
 Hard drusen are round, with clearly defined borders; soft drusen are larger, with poorly defined borders, and are partially confluent (medium-sized soft drusen 65–124 μm, large soft drusen > 125 μm).
Hard drusen are round, with clearly defined borders; soft drusen are larger, with poorly defined borders, and are partially confluent (medium-sized soft drusen 65–124 μm, large soft drusen > 125 μm).
 The presence of soft, large, and confluent drusen is regarded as a risk factor for progression of the disease. They are sometimes (but not always) associated with impaired vision.
The presence of soft, large, and confluent drusen is regarded as a risk factor for progression of the disease. They are sometimes (but not always) associated with impaired vision.
 Hyperpigmentation or hypopigmentation of the retinal pigment epithelium may be present, with variable expression.
Hyperpigmentation or hypopigmentation of the retinal pigment epithelium may be present, with variable expression.
Fundus Autofluorescence
 Fundus autofluorescence is a noninvasive method for monitoring progression in age-related maculopathy.
Fundus autofluorescence is a noninvasive method for monitoring progression in age-related maculopathy.
 Not all drusen are visible with fundus autofluorescence.
Not all drusen are visible with fundus autofluorescence.
 Different patterns have recently been classified: normal fundus autofluorescence and increased autofluorescence, with the following patterns: minimal change, focally increased, patchy, linear, lace-like, reticular, and speckled.
Different patterns have recently been classified: normal fundus autofluorescence and increased autofluorescence, with the following patterns: minimal change, focally increased, patchy, linear, lace-like, reticular, and speckled.
Fluorescein Angiography
 On fluorescein angiography, drusen can appear either as hyperfluorescent or hypofluorescent.
On fluorescein angiography, drusen can appear either as hyperfluorescent or hypofluorescent.
 In the early phase of angiography, hard drusen are already visible as hyperfluorescent structures, while in the late phase they tend to show weaker hyperfluorescence.
In the early phase of angiography, hard drusen are already visible as hyperfluorescent structures, while in the late phase they tend to show weaker hyperfluorescence.
 Soft drusen accumulate fluorescein more slowly during the course of the angiography. The hyperfluorescence is not as clear, but continues to be present for a longer period in comparison with hard drusen.
Soft drusen accumulate fluorescein more slowly during the course of the angiography. The hyperfluorescence is not as clear, but continues to be present for a longer period in comparison with hard drusen.
 The distinction between confluent soft drusen and a small choroidal neovascularization (CNV) or RPE detachment can be difficult to establish, due to the slow increase in hyperfluorescence.
The distinction between confluent soft drusen and a small choroidal neovascularization (CNV) or RPE detachment can be difficult to establish, due to the slow increase in hyperfluorescence.
Diagnosis and Treatment
 The diagnosis can usually be established by binocular ophthalmoscopy. Fundus autofluorescence allows easy monitoring of disease progression. Fluorescein angiography is important in some cases for differentiating between CNV and RPE detachment.
The diagnosis can usually be established by binocular ophthalmoscopy. Fundus autofluorescence allows easy monitoring of disease progression. Fluorescein angiography is important in some cases for differentiating between CNV and RPE detachment.
 Providing the patient with information about the symptoms and use of the self-testing Amsler grid are important measures for early detection of the development of exudative AMD and assessing the risk of loss of visual acuity. These are prerequisites for the earliest possible therapy.
Providing the patient with information about the symptoms and use of the self-testing Amsler grid are important measures for early detection of the development of exudative AMD and assessing the risk of loss of visual acuity. These are prerequisites for the earliest possible therapy.
 Prophylactic laser coagulation is not a safe treatment option and is associated with a risk of secondary CNV.
Prophylactic laser coagulation is not a safe treatment option and is associated with a risk of secondary CNV.
 At present, prophylactic treatment with a specific combination of vitamins and nutrient supplements has only been found to be beneficial in relation to disease progression in a subgroup of ARM patients with mediumsized drusen (65–124 μm) and at least one large one (> 125 μm) (ARED study).
At present, prophylactic treatment with a specific combination of vitamins and nutrient supplements has only been found to be beneficial in relation to disease progression in a subgroup of ARM patients with mediumsized drusen (65–124 μm) and at least one large one (> 125 μm) (ARED study).
 For family members of patients with ARM or AMD who are over the age of 50, a fundus examination is advisable.
For family members of patients with ARM or AMD who are over the age of 50, a fundus examination is advisable.
References
3.3 Geographic Atrophy
Epidemiology, Pathophysiology, and Clinical Presentation
 Nonexudative or atrophic age-related macular degeneration (“dry AMD”) is one of the two advanced, end-stage types of AMD.
Nonexudative or atrophic age-related macular degeneration (“dry AMD”) is one of the two advanced, end-stage types of AMD.
 It mainly involves extended areas with atrophy of the photoreceptors, the retinal pigment epithelium (RPE), and the choriocapillaris, forming a geographic atrophy. Drusen may be present on the edge of the lesion.
It mainly involves extended areas with atrophy of the photoreceptors, the retinal pigment epithelium (RPE), and the choriocapillaris, forming a geographic atrophy. Drusen may be present on the edge of the lesion.
 Loss of visual acuity is subtle; individual atrophic areas can, over time, enlarge and become confluent. In bilateral cases, the shape and size of the affected areas are often symmetrical.
Loss of visual acuity is subtle; individual atrophic areas can, over time, enlarge and become confluent. In bilateral cases, the shape and size of the affected areas are often symmetrical.
 Approximately 20% of severe visual loss in AMD is caused by geographic atrophy.
Approximately 20% of severe visual loss in AMD is caused by geographic atrophy.
Fundus Autofluorescence
 The advantages of fundus autofluorescence in comparison with fluorescein angiography are its ability to depict the area surrounding the atrophic zone and its reduced invasiveness for follow-up examinations.
The advantages of fundus autofluorescence in comparison with fluorescein angiography are its ability to depict the area surrounding the atrophic zone and its reduced invasiveness for follow-up examinations.
 Fundus autofluorescence makes it possible to depict the atrophic area. Within the atrophic lesion, absence of autofluorescence indicates the loss of RPE and associated lipofuscin. Different, recently classified patterns of abnormal fundus autofluorescence in the junctional zone in geographic atrophy make it possible to draw conclusions regarding the subsequent progression.
Fundus autofluorescence makes it possible to depict the atrophic area. Within the atrophic lesion, absence of autofluorescence indicates the loss of RPE and associated lipofuscin. Different, recently classified patterns of abnormal fundus autofluorescence in the junctional zone in geographic atrophy make it possible to draw conclusions regarding the subsequent progression.
 The junctional zone may show either normal autofluorescence, focally increased autofluorescence, a band of increased autofluorescence, patchy increased autofluorescence, or four types of diffusely increased autofluorescence: reticular, branching, fine granular, and fine granular with peripheral punctate spots.
The junctional zone may show either normal autofluorescence, focally increased autofluorescence, a band of increased autofluorescence, patchy increased autofluorescence, or four types of diffusely increased autofluorescence: reticular, branching, fine granular, and fine granular with peripheral punctate spots.
Fluorescein Angiography
 Fluorescein angiography characteristically shows an extended window defect in the area of the atrophy; as a result, a bright hyperfluorescence arises, caused by the abnormally visible choroidal vessel and the fluorescence of the sclera.
Fluorescein angiography characteristically shows an extended window defect in the area of the atrophy; as a result, a bright hyperfluorescence arises, caused by the abnormally visible choroidal vessel and the fluorescence of the sclera.
 Characteristically, this does not result in visible leakage at the border of the hyperfluorescence. In some cases, the window defect may be confused with choroidal neovascularization or a RPE detachment (see also section 3.1).
Characteristically, this does not result in visible leakage at the border of the hyperfluorescence. In some cases, the window defect may be confused with choroidal neovascularization or a RPE detachment (see also section 3.1).
Diagnosis and Treatment
 The diagnosis is established clinically, and in some cases angiographically. Fundus autofluorescence examinations allow early detection and assessment of the course of the disease.
The diagnosis is established clinically, and in some cases angiographically. Fundus autofluorescence examinations allow early detection and assessment of the course of the disease.
 The different patterns of fundus autofluorescence may be associated with different risks of enlargement of the lesion. Preliminary results show that no alterations in the fundus autofluorescence, or only minimal ones, are associated with a lower risk of progression, while increased autofluorescence in the junctional zone indicates areas of progressive RPE loss. Areas of increased autofluorescence are also associated with increased functional loss.
The different patterns of fundus autofluorescence may be associated with different risks of enlargement of the lesion. Preliminary results show that no alterations in the fundus autofluorescence, or only minimal ones, are associated with a lower risk of progression, while increased autofluorescence in the junctional zone indicates areas of progressive RPE loss. Areas of increased autofluorescence are also associated with increased functional loss.
 There are at present no treatment options. Macular translocation is followed by development of geographic atrophy in the new location of the macula. Transplantation of RPE tissue from other areas under the macula is currently being investigated.
There are at present no treatment options. Macular translocation is followed by development of geographic atrophy in the new location of the macula. Transplantation of RPE tissue from other areas under the macula is currently being investigated.
 Counseling for visual impairment is advisable, and low-vision aids should be prescribed.
Counseling for visual impairment is advisable, and low-vision aids should be prescribed.
References
3.4 Classic Choroidal Neovascularization
Epidemiology, Pathophysiology, and Clinical Presentation
 Classic and occult choroidal neovascularization (CNV) have to be distinguished. They can also appear in combined forms; depending on the relative size of the classic part, the condition is described as predominant or minimal classic CNV. Classic CNVs are considerably less frequent than the occult or mixed forms. The common definition in use today is based on the Macular Photo-coagulation Study (MPS).
Classic and occult choroidal neovascularization (CNV) have to be distinguished. They can also appear in combined forms; depending on the relative size of the classic part, the condition is described as predominant or minimal classic CNV. Classic CNVs are considerably less frequent than the occult or mixed forms. The common definition in use today is based on the Macular Photo-coagulation Study (MPS).
 The diagnosis of a classic CNV requires an angiography. The definition is clinically important, for the choice of therapy. A classic CNV can occur in exudative age-related macular degeneration (AMD), but also secondary to other chorioretinal diseases.
The diagnosis of a classic CNV requires an angiography. The definition is clinically important, for the choice of therapy. A classic CNV can occur in exudative age-related macular degeneration (AMD), but also secondary to other chorioretinal diseases.
 In addition to actual CNVs, exudative lesions can contain other components, such as fibrosed tissue, hemorrhage, pigmentation, or other features that may obscure the boundaries of the CNV. The term “lesion” can be defined as the entirety of the clinically and angio-graphically detectable changes, including all of the above-mentioned changes. The distinction between classic and occult and the estimation of size relate to the whole lesion (see also sections 3.7 and 3.13).
In addition to actual CNVs, exudative lesions can contain other components, such as fibrosed tissue, hemorrhage, pigmentation, or other features that may obscure the boundaries of the CNV. The term “lesion” can be defined as the entirety of the clinically and angio-graphically detectable changes, including all of the above-mentioned changes. The distinction between classic and occult and the estimation of size relate to the whole lesion (see also sections 3.7 and 3.13).
 A classic CNV is defined as a clearly visible and well-demarcated hyperfluorescence in the early phase, with increasing leakage in the late phase of the angiography.
A classic CNV is defined as a clearly visible and well-demarcated hyperfluorescence in the early phase, with increasing leakage in the late phase of the angiography.
 Newly formed fibrovascular networks which grow out of the choriocapillaris through Bruch membrane between the retina and the retinal pigment epithelium (RPE) are the basis for this angiographic picture. In angiography, classic CNVs are therefore better defined than occult CNVs, which principally proliferate under the RPE.
Newly formed fibrovascular networks which grow out of the choriocapillaris through Bruch membrane between the retina and the retinal pigment epithelium (RPE) are the basis for this angiographic picture. In angiography, classic CNVs are therefore better defined than occult CNVs, which principally proliferate under the RPE.
 The initial symptoms of classic CNV are metamorphopsia, deterioration in visual acuity, and central visual field defects.
The initial symptoms of classic CNV are metamorphopsia, deterioration in visual acuity, and central visual field defects.
 Ophthalmoscopic signs of CNV are grayish-white sub-retinal changes together with retinal edema, hard exudations, and subretinal and intraretinal hemorrhage. If the condition is not treated, progression with enlargement of the lesion and subsequent loss of photoreceptors will usually follow.
Ophthalmoscopic signs of CNV are grayish-white sub-retinal changes together with retinal edema, hard exudations, and subretinal and intraretinal hemorrhage. If the condition is not treated, progression with enlargement of the lesion and subsequent loss of photoreceptors will usually follow.
 The final stage is a subretinal fibrosis or disciform scar.
The final stage is a subretinal fibrosis or disciform scar.
Fluorescein Angiography
 An early bright, well-demarcated hyperfluorescence that is caused by vascular proliferations between the RPE and the neuroretina is typical for a classic CNV.
An early bright, well-demarcated hyperfluorescence that is caused by vascular proliferations between the RPE and the neuroretina is typical for a classic CNV.
 CNVs appear either as a network with clearly definable vessels or as a homogeneous structure. A small hypo-fluorescent edge is often visible. Evidence of a clearly defined vascular network is not mandatory for the diagnosis of a classic CNV.
CNVs appear either as a network with clearly definable vessels or as a homogeneous structure. A small hypo-fluorescent edge is often visible. Evidence of a clearly defined vascular network is not mandatory for the diagnosis of a classic CNV.
 In the late phase increasing hyperfluorescence with clear leakage is visible, caused by the outflow of dye from the permeable vessels of the CNV.
In the late phase increasing hyperfluorescence with clear leakage is visible, caused by the outflow of dye from the permeable vessels of the CNV.
 Leakage means that the intensity of the hyperfluorescence in the late phase increases and extends beyond the borders of the CNV visible in the early phase.
Leakage means that the intensity of the hyperfluorescence in the late phase increases and extends beyond the borders of the CNV visible in the early phase.
Diagnosis and Treatment
 A purely clinical distinction between classic and occult CNV is not possible, fluorescein angiography is essential for confirmation and differentiation.
A purely clinical distinction between classic and occult CNV is not possible, fluorescein angiography is essential for confirmation and differentiation.
 Angiography is not usually required if exudative changes cannot be clinically detected, if there is extensive hemorrhage, or if a disciform scar can be seen in the advanced form of the disease. In these situations no treatment options exist and the diagnosis can be established without angiography.
Angiography is not usually required if exudative changes cannot be clinically detected, if there is extensive hemorrhage, or if a disciform scar can be seen in the advanced form of the disease. In these situations no treatment options exist and the diagnosis can be established without angiography.
 Further categorization of CNVs is based on their position in relation to the center of the fovea (see section 3.7). Treatment recommendations are based on these classifications.
Further categorization of CNVs is based on their position in relation to the center of the fovea (see section 3.7). Treatment recommendations are based on these classifications.
 In subfoveally predominant classic CNVs, photodynamic therapy is the treatment of choice, based on the findings of the Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) study and Verteporfin in Photodynamic Therapy (VIP) study. In the Macular Photocoagulation Study, the use of argon laser coagulation is reserved for juxtafoveal and extrafoveal classic CNVs (see section 3.12).
In subfoveally predominant classic CNVs, photodynamic therapy is the treatment of choice, based on the findings of the Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) study and Verteporfin in Photodynamic Therapy (VIP) study. In the Macular Photocoagulation Study, the use of argon laser coagulation is reserved for juxtafoveal and extrafoveal classic CNVs (see section 3.12).
 New treatment procedures include intravitreal or subscleral application of agents inhibiting angiogenesis and a combination of photodynamic therapy with either intravitreal application of triamcinolone or angiogenesis-inhibiting agents. The indications for combination treatment and the optimal choice of drug for specific CNV locations or sizes are currently being investigated in detail.
New treatment procedures include intravitreal or subscleral application of agents inhibiting angiogenesis and a combination of photodynamic therapy with either intravitreal application of triamcinolone or angiogenesis-inhibiting agents. The indications for combination treatment and the optimal choice of drug for specific CNV locations or sizes are currently being investigated in detail.
 Optical coherence tomography appears to helpful for treatment control and planning of repeat treatment.
Optical coherence tomography appears to helpful for treatment control and planning of repeat treatment.
References
3.5 Occult Choroidal Neovascularization
Epidemiology, Pathophysiology, and Clinical Presentation
 Occult choroidal neovascularization (CNV) represents a subgroup of neovascular age-related macular degeneration (AMD) and encompasses approximately 80% of all newly diagnosed cases of CNV. Occult CNV is more common in Caucasians and has no gender preference.
Occult choroidal neovascularization (CNV) represents a subgroup of neovascular age-related macular degeneration (AMD) and encompasses approximately 80% of all newly diagnosed cases of CNV. Occult CNV is more common in Caucasians and has no gender preference.
 In occult CNV, neovascular vessels from the choroidal capillaries penetrate the Bruch membrane below the retinal pigment epithelium (RPE). Invasion under the retina is also possible when the disease progresses.
In occult CNV, neovascular vessels from the choroidal capillaries penetrate the Bruch membrane below the retinal pigment epithelium (RPE). Invasion under the retina is also possible when the disease progresses.
 A slow gradual decrease in visual acuity is characteristic of occult CNV (classic CNV is more aggressive).
A slow gradual decrease in visual acuity is characteristic of occult CNV (classic CNV is more aggressive).
Fluorescein Angiography
 Type 1 (fibrovascular pigment epithelial detachment):
Type 1 (fibrovascular pigment epithelial detachment):
 Type 2 (late leakage of undetermined source):
Type 2 (late leakage of undetermined source):
 Neovascular lesion: the area of the classic and occult choroidal neovascularization.
Neovascular lesion: the area of the classic and occult choroidal neovascularization.
 Lesion: the whole area of the neovascular lesion and the components of the lesion (e. g., adjacent blood).
Lesion: the whole area of the neovascular lesion and the components of the lesion (e. g., adjacent blood).
 Lesion components: refers to the CNV and the fundus pathologies at the border of the neovascular lesion that obscure the exact borders of the CNV (e. g., pigment, hemorrhage, serous RPE detachment).
Lesion components: refers to the CNV and the fundus pathologies at the border of the neovascular lesion that obscure the exact borders of the CNV (e. g., pigment, hemorrhage, serous RPE detachment).
 Blocked hyperfluorescence: hypofluorescence caused by blockage on the edge of a neovascular lesion in the absence of a hemorrhage (arising from subretinal fibrin, pigment or subretinal fibrosis). It is classified as a part of the neovascular lesion.
Blocked hyperfluorescence: hypofluorescence caused by blockage on the edge of a neovascular lesion in the absence of a hemorrhage (arising from subretinal fibrin, pigment or subretinal fibrosis). It is classified as a part of the neovascular lesion.
 Predominantly classic or minimally classic CNV: the classic part of the CNV in relation to the neovascular lesion is either more or less than 50%.
Predominantly classic or minimally classic CNV: the classic part of the CNV in relation to the neovascular lesion is either more or less than 50%.
Diagnosis and Treatment
 Diagnosis is based on the stereoscopic fluorescein-angiographic classification established by the Macular Photocoagulation Study (MPS).
Diagnosis is based on the stereoscopic fluorescein-angiographic classification established by the Macular Photocoagulation Study (MPS).
 It consists of a subretinal fluid or fibrovascular pigment epithelial detachment. Reliable and objective analysis of an occult CNV is only possible using stereoscopic fluorescein angiography.
It consists of a subretinal fluid or fibrovascular pigment epithelial detachment. Reliable and objective analysis of an occult CNV is only possible using stereoscopic fluorescein angiography.
 Laser coagulation of occult membranes leads to a more unfavorable outcome than the natural course.
Laser coagulation of occult membranes leads to a more unfavorable outcome than the natural course.
 In a subgroup of patients with occult CNVs, photodynamic therapy (PDT) appears to have an advantage over untreated control groups (CNV in less than four disk areas, vision 20/50 or less, recent disease progression). However, in occult CNVs with pigment epithelial detachment, there is a risk of pigment epithelial tears (see section 3.8) with a consequent marked reduction in visual acuity.
In a subgroup of patients with occult CNVs, photodynamic therapy (PDT) appears to have an advantage over untreated control groups (CNV in less than four disk areas, vision 20/50 or less, recent disease progression). However, in occult CNVs with pigment epithelial detachment, there is a risk of pigment epithelial tears (see section 3.8) with a consequent marked reduction in visual acuity.
 Recently the intravitreal application of Anti-VEGF-agents has shown beneficial effects in selected cases of occult CNV. With the increasing availability of new therapeutic agents (see section 3.14) in the near future the therapy of occult CNV may change rapidly.
Recently the intravitreal application of Anti-VEGF-agents has shown beneficial effects in selected cases of occult CNV. With the increasing availability of new therapeutic agents (see section 3.14) in the near future the therapy of occult CNV may change rapidly.
 There is currently a lack of established research results for other experimental treatment options (e. g., transpupillary thermo therapy, indocyanine green-guided laser coagulation, feeder vessel occlusion, periocular and intraocular steroid injections, macular surgery).
There is currently a lack of established research results for other experimental treatment options (e. g., transpupillary thermo therapy, indocyanine green-guided laser coagulation, feeder vessel occlusion, periocular and intraocular steroid injections, macular surgery).
 A transition between an occult CNV and minimally classic or predominantly classic CNV is possible (50% in 1 year). Despite slowly progressive reductions in visual acuity, therefore, regular examinations with fluorescein angiography are warranted.
A transition between an occult CNV and minimally classic or predominantly classic CNV is possible (50% in 1 year). Despite slowly progressive reductions in visual acuity, therefore, regular examinations with fluorescein angiography are warranted.
References
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


