Fig. 5.1
(a) Day 1 of PROSE treatment for persistent epithelial defect 8 months after acute Stevens-Johnson syndrome. (b) Day 1 of PROSE treatment for persistent epithelial defect 8 months after acute Stevens-Johnson syndrome. Blue light and fluorescein. (c) Day 6 of PROSE treatment for persistent epithelial defect 8 months after acute Stevens-Johnson syndrome. (d) Day 6 of PROSE treatment for persistent epithelial defect 8 months after acute Stevens-Johnson syndrome. Blue light and fluorescein. (e) Week 8 of PROSE treatment
Patients with both OSD and advanced glaucoma present a particular challenge. Filtering blebs or tube shunts are a relative contraindication to contact lens use because of risk of infection or erosion. The devices used in PROSE treatment can be modified for support of the ocular surface in the presence of advanced glaucoma (Tanhehco and Jacobs 2010).
5.3 Contact Lens for the Treatment of Corneal Ectasia
Corneal ectasia is a progressive thinning and steepening of the cornea that occurs pathologically or after corneal surgery. The corneal ectasias include keratoconus, keratoglobus, pellucid marginal degeneration, Terrien’s marginal degeneration, and post-LASIK ectasia. Keratoconus is the most common of the corneal ectasias and is estimated to have an incidence of the single most common corneal dystrophy or degeneration and affects 1 in 2000 Americans (NEI 2013). Typically, the vision deficits due to corneal ectasias can initially be treated with the use of glasses. However, as ectasia progresses, irregular astigmatism may not be corrected adequately with spectacles, requiring soft lenses then hard lenses for satisfactory vision. Some cases are characterized by scarring as well as thinning.
Contact lens failure and intolerance are accepted indications for corneal transplantation (Rabinowitz 1998) even if the cornea is clear. It is worth considering that the rate of postoperative contact lens wear for satisfactory visual rehabilitation after penetrating keratoplasty for keratoconus is 31, 43, and 47% (Silbiger et al. 1996; Brierly et al. 1996; Geerards et al. 2006; Jacobs and Rosenthal 2007; Tomalla and Canolati 2007). A longitudinal study of 1,004 eyes in 518 keratoconus patients over a 30-year period was conducted and found that contact lenses were a successful treatment option and postponed surgery in 99 % of fittings (Bilgin et al. 2009). Once a patient’s refractive need extends beyond what soft spherical, soft toric, or convention corneal RGP lenses can offer, “specialty lenses” become an option. Specialty lenses include soft lenses designed specifically for keratoconus and RGP corneal lenses designed specifically for keratoconus, piggyback systems, hybrid lenses, scleral lenses, and PROSE treatment. Specialty spherical or toric soft lenses with steeper base curves are a good option as keratoconus progresses to the point that spectacles or conventional contact lenses are inadequate. Specialty soft lenses provide a number of advantages in treating lower grade ectasia. They typically do not require adaptation on the patient’s part, and principles of fitting are similar to those for conventional soft lenses.
RGP corneal lenses are typically the next option for patients with corneal ectasia who cannot be adequately corrected with soft contact lenses or spectacles. RGP corneal lenses offer more complete neutralization of irregular astigmatism due to the fluid tear lake under the lens and rigid interface with the atmosphere. A corneal RGP has tendency to move to the steepest part of the cornea which, in ectasia, is typically inferior; this results in an intrapalpebral fit which is less mechanically stable than the preferred fit characterized by lid attachment (Fig. 5.2).
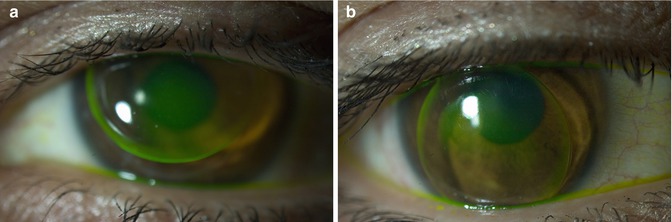
Fig. 5.2
(a) RGP corneal lens with optimal fit: “lid attachment”. (b) RGP corneal lens with adequate fit: “intra-palpebral”
Piggyback systems are an option to increase mechanical stability and comfort of a corneal RGP lens. A piggyback system involves wearing an RGP corneal lens over a soft lens (Fig. 5.3) and can be useful in cases of RGP lens intolerance in corneal ectasia (O’Donnell and Maldonado-Codina 2004). Eyes wearing hybrid systems should be monitored closely for signs of hypoxia, which is a risk when total lens thickness is high.
Fig. 5.3
Piggyback lens system in patient with keratoconus and history of Stevens-Johnson syndrome
Hybrid lenses are lenses of two different materials, assembled concentrically; these lenses have a hard center and soft periphery. The peripheral portion is sometimes referred to as the skirt. Hybrid lenses represent an attempt to combine the optical advantages of a hard lens with the comfort advantages of a soft lens. Hybrid is a lens made of two materials, whereas a piggyback system consists of two lenses, one placed over the other on the yes. Problems with early hybrids included tendency toward hypoxia and neovascularization due to low-Dk materials and tendency to develop suction and adherence under the central optic portion. The lenses tended to suffer under handling with disintegration at the junction between materials.
Larger diameter RGP lenses, including corneoscleral, semi-sclera, mini-scleral, and scleral lenses, offer increased stability with equally excellent optics in comparison to corneal RGP lenses. The increased stability related to the larger diameter can increase comfort and reduce lens awareness, as well as reduce likelihood of “popping” lenses, that is, losing lenses during wear.
5.4 Recent Advances: Corneal Ectasia
5.4.1 Soft Lens
In the last several years, specialty soft lenses of SiHy material have been introduced with reports of better comfort and increased tolerance compared to RGP lenses in the early stages of keratoconus (Ozkurt et al. 2012). The newer lenses of higher Dk material would presumably reduce the likelihood of hypoxic complications seen with hydrogel lenses in which a tight fit might have been accepted for mechanical stability and comfort on that basis. Soft specialty lenses are generally available at lower cost than other specialty lenses. Ultimately as ectasia progresses, soft lenses may not be adequate to neutralize irregular astigmatism as they essentially drape over rather than neutralize any local steepening.
5.4.2 Rigid Gas-Permeable Corneal Lenses
Inferior steepening and absolute steepening of >52 D are predictors of less stable fit. Faced with a choice between a tight fit with apical bearing or a loose fit which is unstable and can result in lost lenses, there are many patients who are maintained in tight fit till scarring occurs, at which time keratoplasty is required. In the last decade, many options including introduction of higher Dk RGP materials and increased appreciation of back surface toric designs have allowed for increased mechanical stability without excessive bearing apically on the flatter meridian.
5.4.3 Piggyback Systems
Modern piggyback systems use a high-Dk silicone hydrogel lens underneath the RGP lens in an attempt to overcome past issues with hypoxia related to the total thickness of the system. The overall Dk of the piggyback system varies with the Dk thickness of both lenses. Recent report suggests that negative-powered soft lenses may be optically for use in piggyback systems because of reduced aberrations related to local flattening (Romero-Jimenez et al. 2013).
5.4.4 Hybrid Lenses
Hybrid lenses technology has advanced to incorporate higher Dk materials in both the rigid center and the hydrogel skirt. There are new specialty designs to accommodate apical cones and corneas with reverse geometry (central flattening) after cornea transplant or refractive surgery. Earlier problems with hybrid lenses have been addressed with the newer designs and materials of the last decade, with two studies finding 79.5 and 86 % success rates in patients with moderate or advanced disease (Nau 2008; Abdalla et al. 2010). A study from the Cornea Service at Wills Eye Institute administered the Contact Lens Impact on Quality of Life Questionnaire (CLIQ) on 71 consecutive patients who wore soft toric, RGP, or hybrid lenses in at least one eye with keratoconus and found that there was no difference in quality of life among the three groups (Erdurmus et al. 2009). There is an argument that the reason for the slow acceptance of modern hybrid lenses is the relatively high cost compared to RGP corneal or soft lenses and the assertion that they do not improve visual acuity or comfort when compared to RGP corneal contact lenses (Romero-Jimenez et al. 2010).
Corneal complications even with the newest designs have been reported (Fernandez-Velazquez 2011), with clinical experience suggesting that these lenses can develop suction and adherence that may not be detected in the initial fitting process.
5.4.5 RGP Mini-scleral and Scleral Lens
Mini-scleral lenses are reported as a good option for visual rehabilitation after placement of intrastromal corneal ring segments (Karlgard et al. 2004). Any of these larger RGP lenses would have the advantage over corneal RGP lenses in that bearing on the thin cornea directly over the segment is less likely. A reported complication of mini-scleral contact lens wear is nonulcerative keratitis perhaps related to compression from peripheral seal or lens hygiene or care product (Bruce and Nguyen 2013). Advances in lens design and manufacture to incorporate back-surface toricity allowing for alignment with toric sclerae increase the likelihood of success with large diameter RGP lenses (Visser et al. 2006; Baran et al. 2012).
5.4.6 PROSE Treatment
PROSE treatment is an effective option for the treatment of corneal ectasia and astigmatism. As described previously, the devices used in PROSE treatment are made of highly gas-permeable material; the fit is typically characterized by fluid ventilation, minimal movement, and no contact with the cornea (Fig. 5.4a, b). The latter features account for the excellent optics and comfort achieved in PROSE treatment for patients with corneal ectasia. A study of patients who were referred having failed contact lens rehabilitation found mean change of −0.54 logMAR (approximately 5 lines improvement) in visual acuity compared to habitual correction and mean of 20 points improvement in visual function in the NEI VFQ-25 questionnaire (Stason et al. 2010). A study of a subsequent cohort confirmed this level of impact on both acuity and visual function and reported that 78/89(88 %) eyes that were fitted with devices were still wearing the PROSE devices and had a mean improvement in VFQ-25 scores of 27.6 (P < 0.001) on a 100-point scale after 6 months. Eyes that had undergone previous penetrating keratoplasty were included in the analysis, with similar results. 93.1 % of eyes achieved a visual acuity of 20/40 or better (Baran et al. 2012). There was not one candidate eye that could not be fitted, despite including patients who had failed previous attempts at contact lens treatment using advance technologies such as specialty corneal lenses, hybrid lenses, piggyback systems, and even scleral lenses (Table 5.1) (Baran et al. 2012).
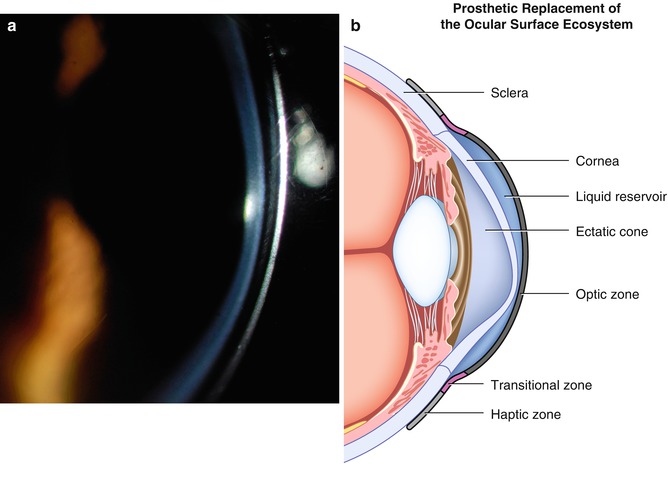
Fig. 5.4
(a) Slit lamp image of PROSE treatment. Note fluid-filled space behind back surface of prosthetic device and front surface of cornea. (b) Corresponding schematic diagram of PROSE device in cross-section over ectatic cornea
Table 5.1
Contact lens history in patients referred for PROSE treatment
90 % of patients had tried contact lenses |
75 % of patients had tried rigid gas-permeable lenses |
22 % of patients had tried piggyback lenses |
17 % of patients had tried hybrid lenses |
Recent reports reveal that PROSE treatment can serve as platform for the correction of higher order aberrations. There are reports of reduction of HOAs across all diagnosis (Gumus et al. 2010) and of improvement of low-contrast vision in keratoconus with PROSE treatment (Hussoin et al. 2012) using aspheric optics. Because stability of fit and capacity for precise registration on the eye, devices used in PROSE treatment are a suitable platform for custom HOA correction in corneal ectasia (Sabesan et al. 2013).
The advances in PROSE treatment have caused a paradigm shift in the management of corneal ectasia, because a PROSE device can accommodate any corneal shape. PROSE treatment is now widely available across the United States. PROSE treatment is a practical alternative to penetrating keratoplasty for eyes with advanced disease considered to be “contact lens intolerant.” Furthermore, “axial opacity” is not sufficient indication for keratoplasty unless vision has been assessed wearing a mechanically stable contact lens or PROSE device.
5.5 Future Innovations
Innovation in contact lens holds promise for treatment of disease in the decade ahead.
Soft hydrogels which can be configured as contact lenses have been investigated as a drug delivery system for antimicrobials in the treatment of ocular surface disease, vision defects, infections, chronic dry eye, and allergies. The advantage of using soft hydrogels over aqueous or oily solutions for drug delivery is that soft hydrogels have been reported to allow for controlled delivery on the ocular surface for 3 days (Kakisu et al. 2013), 2 weeks (Glisoni et al. 2013), and up to 30 days (Lu et al. 2013), whereas topical solutions provide bioavailability over a range of minutes to hours (Glisoni et al. 2013). Contact lenses may be used as a vehicle to deliver and transplant corneal stem cells for ocular surface reconstruction (Di Girolamo et al. 2009).
The field of contact lens fitting is also an area of innovation, particularly for the purpose of fitting large-diameter lenses, in which optical imaging of the cornea may not be sufficient for deriving parameters for fit over the sclera. Three-dimensional imaging of the ocular surface holds promise for image-guided fitting and image-guided lens design. High-resolution image-guided fitting might replace the time and resource consuming trial lens method, especially for scleral lenses and PROSE treatment. The two competing technologies that are working toward this goal are optical coherence tomography (OCT) and laser-guided fitting. Recent reports suggest that OCT technology can be used to guide customization in PROSE treatment (Le et al. 2012) and to increase likelihood of initial lens success in the design of mini-scleral lenses (Gemoules 2008).
Finally, the suitability of devices used in PROSE treatment for the customized correction of HOAs in corneal ectasia (Sabesan et al. 2013) holds promise for other applications specialized optics for presbyopia that might offer increased depth of focus and custom correction of HOAs to achieve “super-vision” for specific applications.
5.6 Conclusions
Contact lenses, specialty lenses, and PROSE treatment play a vital role in the treatment of ocular surface disease and corneal ectasia. It is expected that emerging contact lens technology will continue to offer alternatives to current medical and surgical options for complex corneal disease. Clinicians will serve their patients well to be familiar with the full range of therapeutic contact lens options for the treatment of OSD and ectasia.
Compliance with Ethical Requirements
Author Deborah S. Jacobs is a full-time salaried employee 501(c)3 of Boston Foundation for Sight. Author Joshua Agranat is a medical student at Boston University School of Medicine. Neither author has proprietary or financial interest in any contact lens or prosthetic device.
Informed consent and animal studies disclosures are not applicable to this review.
References
Abdalla YF, Elsahn AF, Hammersmith KM, Cohen EJ. SynergEyes lenses for keratoconus. Cornea. 2010;29:5–8.PubMedCrossRef
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


