Stromal scarring
Corneal ectasia
Corneal dystrophy
Iatrogenic
Post-infectious
Keratoconus
Granular
Post-pterygium surgery
Trauma
Post-refractive surgery ectasia
Lattice
Post-ocular surface tumor excisions
Macular
7.3 Donor Tissue Selection
For DALK and sALK donor tissue can be lamellar/patch grade. It is important that tissue with good endothelial function is available in case the surgical procedure needs to be converted to a full-thickness procedure.
7.4 Anesthesia Planning
Anterior lamellar surgery can typically be performed under local anesthesia (peribulbar or retrobulbar block) using a long-acting drug under monitored care by the anesthesia service. In cases where the surgeon expects a longer surgical time, it is recommended to use a lid block. General anesthesia can be considered for cases not related to the surgical technique such as pediatric age group, deafness, mental retardation, claustrophobia, etc. If general anesthesia is going to be used, it is important that the anesthesiologist is aware that depending on the surgical technique, an intraocular air injection may be used and for this reason nitrous oxide should not be used.
7.5 Surgical Procedures
7.5.1 Superficial Anterior Lamellar Keratoplasty
When superficial anterior lamellar keratoplasty (sALK) is being considered, a complete ophthalmic evaluation is warranted with special attention to the degree of the anterior scar and the amount of regular versus irregular astigmatism. A rigid gas-permeable contact lens over-refraction is recommended. This will provide the surgeon with information that will determine if the vision loss is mostly related from the stromal opacity or is secondary to a high degree of astigmatism. sALK is often associated with postoperative astigmatism, and this should be explained to the patient.
There are many surgical techniques available for the removal of anterior stromal corneal pathology. The three most common are manual dissection, microkeratome-assisted ALK, and sutureless femtosecond laser-assisted anterior lamellar keratoplasty (FALK).
7.5.2 Manual Dissection
For doing a manually dissected sALK, a partial-thickness trephination is performed followed by a manual lamellar dissection with a sharp spatula or crescent blade. A donor graft is fashioned to fit the excised area and then sutured in placed. Due to the irregular interface obtained when this type of dissection is performed, the rate of interface haze is high, and for this reason this procedure is rarely utilized for optical purposes.
7.5.3 Microkeratome-Assisted Superficial ALK
This surgical technique is a type of ALK that utilizes the principles of LASIK surgery of using a microkeratome to create a smooth flap surface with the goal of minimizing interface haze. For this procedure the microkeratome is set to create a “free cap” that is usually about 130–160 μm in thickness for the treatment of anterior stromal opacities. For this reason, this technique is used for opacities located within the 150–200 μm of the anterior stroma. This technique was described by Busin (2006). The recipient eye is usually prepared using the 130 μm head of the microkeratome and with the ring set at 0 number (Busin 2006). The microkeratome is also used to cut the donor tissue using a whole globe or a donor graft mounted on an artificial anterior chamber. Since the donor tissue will be thin, it is recommended to mark the anterior surface of the cornea before performing the cut, to avoid losing proper orientation.
Once the donor tissue is obtained, this tissue is placed onto the recipient bed. Overlay sutures are recommended to secure the graft in place. The overlay suture technique involves passing the needle only at the host cornea and this way avoiding any distortion of the thin donor graft to minimize postoperative astigmatism. Another alternative is the use of a bandage contact lens. The report of the technique by Busin included a group of 20 patients with a minimum follow-up of a year and showed that all patients improved to a best-corrected visual acuity of at least 20/40. Postoperative astigmatism was less than 4 diopters.
Another advantage of this procedure is that the patients’ postoperative refractive outcome can be improved with the use of excimer laser stromal ablation. The flap can be lifted and the patients’ corneal stroma can be ablated for the desired correction. One of the drawbacks for this procedure is that just like in LASIK surgery, the epithelium can grow and cause epithelium ingrowth, and patients can have all the other known related LASIK corneal flap complications such as flap striae, interface debri, etc. (Karabela et al. 2014).
This technique has also been evaluated in patients with anterior stromal opacities after a penetrating keratoplasty. A report by Patel et al. demonstrated in 9 eyes of 8 consecutive patients that the procedure was safe and was effective. Eight of the nine patients recovered a vision of 20/40 or better within the first month of surgery. In one patient the vision remained unchanged (Patel et al. 2012).
7.5.4 Sutureless Femtosecond Laser-Assisted Anterior Lamellar Keratoplasty
The unique capability of the femtosecond laser (FS laser) to photo-disrupt tissue with minimal collateral tissue damage has revolutionized the corneal surgical field. Since the FDA approved the FS laser for lamellar use in 2000, its use has widely spread and is now routine for surgical procedures such as LASIK flap creations, penetrating keratoplasty, and endothelial keratoplasty (Shousha and Yoo 2010).
The use of the FS laser for SALK is not an exception. It has been demonstrated that the FS laser can precisely cut the anterior stroma and these cuts are highly reproducible. One of the theoretical benefits of the use of FS laser for a lamellar cut is that this laser can precisely do a vertical cut at the graft-host junction, compared with the horizontal cut of the microkeratome.
In 2008, Yoo et al. introduced a new concept of sutureless superficial anterior lamellar surgery using the FS laser called femtosecond laser-assisted sutureless anterior lamellar keratoplasty (FALK) (Yoo et al. 2008). This technique can be performed under topical anesthesia and can be performed at a refractive surgery suite. For this surgery the patients’ anterior corneal opacity depth is imaged and measured using ocular coherence tomography (OCT). The donor graft is obtained using a donor whole globe or a donor graft mounted on an artificial chamber maintainer. The corneal epithelium is removed before the flap is cut. The donor graft is cut with the femtosecond laser. The donor thickness is set to 20 % more from the measurement obtained with the OCT (to adjust for tissue edema). A spiral method is used. The diameter is determined by the patient’s needs and the surgeon’s surgical plan. The recipient cornea is created using similar settings except that it is 0.1 mm smaller in diameter than the donor graft. The host cornea is removed and then replaced by the donor graft. It is recommended to mark the anterior surface of the corneal graft for proper orientation. The graft is observed for 5–10 min to allow donor tissue to dehydrate for a better fit. Then bandage contact lens is placed (Fig. 7.1). The range of energy needed for the side cuts and the spiral cuts is adjusted according to the density of the corneal scar. Higher spiral energy and lower tangent and radial spot separation for denser scars are required. Since the amount of posterior corneal stroma needed to preserve corneal tectonic stability has not been studied, Yoo et al. recommend a LASIK 250 μm residual bed safety margin concept.
Fig. 7.1
Major steps of the sutureless femtosecond laser-assisted anterior lamellar keratoplasty. (Top left) Manual removal of the epithelium from donor whole globe. (Top right) Creation of flap with femtosecond laser. (Middle left) Manual separation of the flap. (Middle right) Flap removal after femtosecond laser cutting on the host cornea. (Bottom left) Placement of donor flap over the host cornea. (Bottom right) Placement of bandage contact lens after a 5 min wait period and speculum removal (Courtesy of Florence Cabot, Mohammed Abou Shousha, and Sonia H. Yoo, Bascom Palmer Eye Institute)
Yoo et al. reported that with a mean follow-up of 12.7 months, the mean difference between preoperative and postoperative BCVA was a gain of 3.8 lines. No graft rejections, infections, or epithelial ingrowth was reported (Fig. 7.2). Shousha et al. then later reported the long-term results of FALK. The report included 13 consecutive patients with a follow-up range of 12–69 months. The study concluded that FALK improves the BCVA of patients with anterior corneal pathology with rapid visual rehabilitation and no significant induced astigmatism (Shousha et al. 2011).
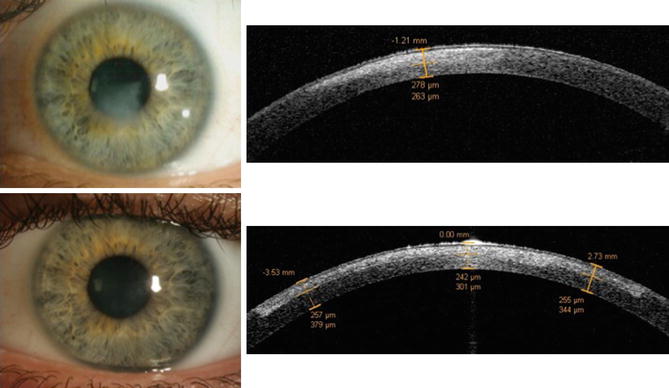
Fig. 7.2
(Top) Preoperative sutureless femtosecond laser-assisted anterior lamellar keratoplasty slit lamp photo and anterior segment optical coherence tomography showing superficial corneal scar. (Bottom left) Postoperative slit lamp photo showing the scar resolution. (Bottom right) Anterior segment optical coherence tomography showing the lamellar bed and overlying graft (Courtesy of Florence Cabot, Mohammed Abou Shousha, and Sonia H. Yoo. Bascom Palmer Eye Institute)
7.6 Deep Anterior Lamellar Keratoplasty
DALK is used for opacities or stromal diseases located deep in the stroma. Otherwise, indications for this procedure are similar to those described for other ALK. During the preoperative evaluation, Descemet’s membrane needs to be carefully evaluated to be sure that this layer has not been violated. Preoperative OCT can help assess the cornea and, for instance, identify the involvement of Descemet’s membrane with scar (Fogla 2013). The most recent DALK techniques further improve on the superficial counterpart in that they achieve visual outcomes comparable to PKP in addition to higher survival of the endothelium and the graft (Borderie et al. 2012; Funnell et al. 2006; Shimazaki et al. 2002; Watson et al. 2004). However, because deeper dissection is involved, there is a higher chance to rupture Descemet’s membrane. PKP quality donor cornea thereby must be available should it be needed.
The most common techniques for performing DALK are manual dissection (open dissection) (Anwar 1972), Melles technique (closed dissection) (Melles et al. 1999, 2000), Anwar’s big-bubble technique (Anwar and Teichmann 2002a), and femtosecond laser-assisted technique (Farid and Steinert 2009; Price et al. 2009; Suwan-Apichon et al. 2006)—in addition to modifications of those techniques (Chamberlain and Cabezas 2011; Ramamurthi and Ramaesh 2011; Sharma et al. 2010).
7.6.1 Manual Dissection
The manual dissection approach is similar to manual dissection described above for sALK. It carries the same drawbacks of unreliable depth and irregular surface causing astigmatism and interface haze, respectively. Also, the depth of the stromal dissection and Descemet’s membrane is difficult to visualize, which increases the risk of perforation or incomplete stromal removal. Techniques like hydrodelamination, intrastromal air injection, and viscoelastic dissection (Maurino et al. 2002) have been developed to improve visualization, decrease operative time, and decrease the risk of perforation.
7.6.2 Melles Technique
The Melles technique was first described by Melles et al. in 1999 (Melles et al. 1999). In this technique aqueous is exchanged by air through a self-sealing limbal side port using a blunt cannula. This creates a mirrorlike air to the endothelium interface that serves as a reference plane for subsequent dissection. A dissection blade is introduced tip down creating a darker band between the blade tip and interface representing the stroma. Dissection is done vertically through this stroma until the interface is reached. The blade is then positioned parallel to the posterior surface, and a deep stromal pocket is created across the cornea. The pocket is then filled with viscoelastic fluid to allow separation of the posterior side, protecting it from perforation during subsequent trephination. Remaining, unincised stromal attachments are cut with curved microscissors, and the anterior corneal lamella is removed. Perforation was reported in 1 out of the 7 (14.3 %) cases in the original article. In terms of outcomes, all eyes maintained structural integrity with minimal interface scarring. The best-corrected visual acuity ranged from 0.25 to 1.0, and the astigmatic error ranged from 1 to 3.5 with no evidence of epithelial or stromal edema over a mean +/− SD follow-up period of 4.9 ± 2.9 months.
7.6.3 Anwar’s Big-Bubble Technique
The Anwar big-bubble technique is a popular technique where air is injected in a certain way to aid in the separation of Descemet’s membrane from the stroma before excising the stroma (Anwar and Teichmann 2002a). In contrast to earlier methods using air to aid dissection where air injection precedes trephination (Archila 1984; Chau et al. 1992), Anwar and Teichmann’s technique starts by performing a partial-thickness trephination. A needle is then inserted into the paracentral corneal stroma and air is injected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


