(1)
St. Johns, FL, USA
(2)
Helen Keller Foundation for Research and Education, International Society of Ocular Trauma, Birmingham, AL, USA
(3)
Consultant and Vitreoretinal Surgeon, Milos Eye Hospital, Belgrade, Serbia
(4)
Consultant and Vitreoretinal Surgeon, Zagórskiego Eye Hospital, Cracow, Poland
39.1 Paracentesis
An often-utilized procedure, paracentesis is not complicated or difficult, but keeping a few fundamental rules in mind makes the surgeon’s job easier and more effective.
Choose the location carefully.
For intracameral manipulations, an entry point in the superotemporal quadrant is the most convenient. The infusion (AC maintainer) is best placed at an inferotemporal location (see below).
Fig. 39.1
The effect of the blade’s shape on the creation of a paracentesis. (a) The MVR blade with its known dimensions is used to create the paracentesis. The internal opening of the tunnel has the same width as the external one, matching the largest diameter of the blade. (b) Using the 15° blade, the external opening of the tunnel is wider than the internal one (this is never needed in clinical practice; the opposite, however, rather often is), and neither is precisely known – it depends on how deep the surgeon penetrates into the AC with the blade. (c) If manipulations that take place far from the site and on both sides of the paracentesis, the surgeon can turn the MVR blade in the frontal plane in both directions, and widen the internal opening of the tunnel. This way the manipulations are easily performed without distorting the cornea, without the need to widen the external tunnel opening. I an imaginary line extended as if it were circle, along the path of the internal course of the tunnel ending; L limbus, the entry point for the tunnel; W the wound created by the blade (b)
Pearl
Do not grab the conjunctiva with forceps as you try to fix the eye to make the paracentesis. The conjunctiva is mobile; the grab will not result in a secure fixation; the tissue can also tear or bleed. Support the nasal side of the eye with your index finger (see Fig. 39.2), or use a pressure plate or corneal fixation ring.

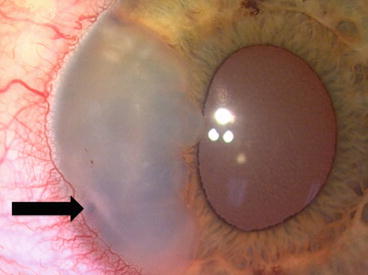
Fig. 39.2
Use of the surgeon’s finger as a surgical tool. The globe can be secured against movement by the surgeon’s finger during the creation of a paracentesis. The wound is made on the temporal side with an MVR blade held rather flat; the tool itself is supported by the surgeon’s thumb, index and middle fingers. The ring and little fingers are pressed against the middle finger but also rest on the patient’s forehead. The surgeon’s other index finger secures the globe’s position; the rest of his fingers of this hand are also pressed against the patient’s forehead to prevent even the slightest movement of eye or tool
Fig. 39.3
Epithelial cyst in the AC. This patient presented with a “cosmetic” problem that greatly bothered him. The cyst was easily removed en block, using forceps. The arrow points to a small wooden IOFB that, the patient later recalled, he had suffered over 20 years earlier. There was no corneal entry site: the object penetrated through the limbus, transplanting viable stem cells inside the eye