Purpose
To compare visual and optical outcomes of pupil-centered vs vertex-centered ablation in patients undergoing laser-assisted in situ keratomileusis (LASIK) for hyperopia.
Design
Randomized, double-masked, prospective, single-center trial.
Methods
Setting: Institutional practice. Study population: Sixty eyes of 30 patients with low and moderate hyperopia. Intervention procedure: Eyes underwent LASIK (Allegretto excimer laser). In 30 eyes, the ablation was centered on the pupil, while in the 30 other eyes the ablation was centered on the corneal reflex. Main outcome measures: Primary outcome measure was the safety index. Main secondary outcome measures were efficacy index, manifest refraction, uncorrected visual acuity, best spectacle-corrected visual acuity (BCVA), and ocular high-order aberrations for a 6-mm pupil size.
Results
At 3 months postoperatively, the safety index was 0.99 ± 0.04 in the pupil-centered group and 0.99 ± 0.08 in the vertex-centered group ( P = .97). The efficacy index was also similar for both groups: 0.96 ± 0.05 in pupil-centered eyes and 0.93 ± 0.09 in vertex-centered eyes ( P = .31). Optical aberrations were similar for pupil-centered and vertex-centered eyes. Considering only eyes showing large pupil decentration, we found a tendency for better visual results in favor of pupil-centered eyes in terms of safety index and a slight but significant increase of coma in vertex-centered eyes.
Conclusion
LASIK is an effective procedure for treatment of hyperopia. Pupil-centered and vertex-centered treatments provide similar visual and optical outcomes. However, in eyes showing large temporal pupil decentration, pupil-centered ablation seemed to produce a lower amount of coma and, as a consequence, a reduced loss of BCVA compared with vertex-centered patients.
Despite generally satisfactory results of hyperopic laser-assisted in situ keratomileusis (LASIK), to optimize treatments we need to aim for the highest degree of accuracy and to improve several surgical parameters such as optical zone size and treatment centration. Ablation centration is one of the factors that may affect the amount and type of corneal aberrations induced by laser refractive surgery, concerning in particular eyes with large angle kappa, mostly hyperopic eyes.
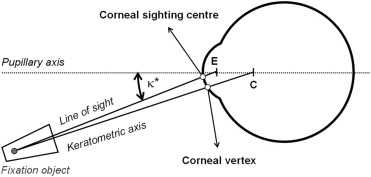
To clarify our terminology, we refer to the corneal sighting center (or visual center of the cornea) as the point where the line of sight, the line between the center of the observed entrance pupil and the object, intersects the cornea, and the corneal vertex as the point where the keratometric axis, the line between the corneal center of curvature and the object, intersects the cornea ( Figure 1 ).
There is no consensus as to whether to use the entrance pupil center or the corneal vertex as the ideal reference for hyperopic ablation centration. Both pupil-centered and vertex-centered ablations are common procedures for the correction of hyperopia.
The pupil is the aperture of the eye’s optical system, and centering on the pupil allows the whole system aperture to be covered with the ablation profile, which should improve the retinal image quality. Furthermore, centering on the pupil is the easiest way for an eye tracking system to work, even though under various illuminations, the pupil size fluctuates and modifies the pupil center position. There are also geometric concerns involving pupil-centered ablation ( Figure 2 ): pupil decentration is related to a tilted cornea and, in a pupil-centered ablation, the laser beam ablates corneal areas with various angles of incidence, which eventually leads to losses of energy in temporal and nasal corneal areas and, finally, to a poor corneal ablation profile.
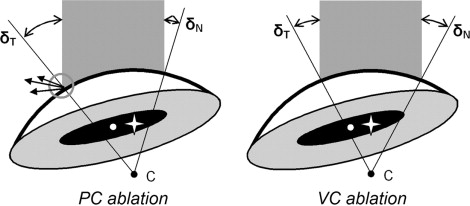
When centering on the vertex, the surgeon does not need to take into account the pupil diameter. After obtaining a good fixation of the eye, the vertex can be localized with great precision and reproducibility. During vertex-centered ablation, the impact of laser efficiency loss attributable to unequal reflections is reduced and the ablation profile is more accurate ( Figure 2 ).
While the ideal centration reference for hyperopic LASIK is still being debated, ablation centration continues to be of particular importance in eyes with large angle kappa. To date, we are unaware of previous prospective studies comparing pupil-centered vs vertex-centered ablations and defining which option offers better visual and optical outcomes. Therefore, we have performed a prospective, randomized double-masked study comparing the results of pupil-centered vs vertex-centered LASIK ablations performed on 2 similar hyperopic populations.
Methods
Study Design and Patient Population
This randomized, double-masked study compared visual, refractive, and aberrometric outcomes of pupil-centered vs vertex-centered hyperopic LASIK. In this preliminary study, 30 patients were recruited prospectively from September 1, 2009 to December 31, 2009 in the Department of Ophthalmology, Purpan Hospital, Toulouse, France. Study inclusion criteria were: at least 40 years old, no previous corneal or intraocular surgery, cornea suitable for LASIK with central corneal pachymetry of at least 520 μm and normal corneal topographic pattern, and a best spectacle-corrected visual acuity (BCVA) better than 20/25. Exclusion criteria were: any abnormal ocular condition such as nuclear sclerosis of the lens or any history of eye disease, such as glaucoma or herpes keratitis. We also excluded patients with refractive astigmatism higher than 1.25 diopters (D). The 2 ablation methods were randomized with the use of a random-number table at the inclusion visit. Preoperative and postoperative data were collected in Purpan Hospital (Toulouse, France), and data analysis was performed in Purpan Hospital and in Universidad de Murcia (Murcia, Spain).
Surgical Technique
For all subjects, we planned monovision: the dominant eye was set for a full correction of refractive error, while the correction of the nondominant eye, determined using the “hole test,” was intended to reach a 0.75-D myopic refraction. Ablation profiles were based on the preoperative subjective and cycloplegic refraction.
For all patients, LASIK was performed under low illumination for both eyes in the same session, by a single surgeon (F.M.) using an Allegretto excimer laser (200 Hz; Alcon, Fort Worth, Texas, USA). The suction ring of the microkeratome was centered on the limbus. Flaps were created by using a One Use + large-cut microkeratome (Moria SA, Antony, France). After folding the corneal flap, the laser beam was focused according to the group of the eye. For the pupil-centered group, the laser beam was centered on the center of the pupil and the cartesian coordinates were dx laser = 0 and dy laser = 0, whereas for the vertex-centered group, the red light defining the laser ablation was placed directly on top of the green corneal reflex and the cartesian coordinates (dx laser and dy laser ) of the ablation were recorded. Once the laser beam was centered, the active Eye Tracker System was turned on, and the ablation was performed.
Patient Examinations
All patients had a full ophthalmologic examination prior to surgery including manifest refraction, cycloplegic refraction, slit-lamp microscopic evaluation of the anterior segment, dilated fundoscopy, and applanation tonometry. BCVA and uncorrected visual acuity (UCVA) were assessed with a standard Early Treatment Diabetic Retinopathy Study (ETDRS) chart. The preoperative examination also included corneal topography (TMS 4; Tomey GmbH, Erlangen, Germany), pupillometry (Colvard; Oasis Medical, Glendora, California, USA), aberrometry (Zywave; Technolas, München, Germany), contrast sensitivity (CVS-1000; Vector Vision, Greenville, Ohio, USA), and ultrasound pachymetry (Corneo-Gage Plus; Sonogage, Cleveland, Ohio, USA). The relative positions of pupil centers and corneal vertex were registered by means of topographic cartesian coordinates (dx topo and dy topo ). Ocular aberrations were measured at a 6-mm pupil size after pharmacologic dilation and estimated by using the entrance pupil center as reference.
Patients were examined postoperatively after 1 day, 1 week, 1 month, 3 months, and 6 months. The surgeon (F.M.) was not involved in postoperative data collection and analyses. At 1-day and 1-week time points after surgery, we only performed a biomicroscopic examination, including a complete record of potential complications such as interface fibrosis, epithelial ingrowth, folds, and opacities. Measurements of visual and optical outcomes were performed later, at 1-, 3-, and 6-month time points after surgery. Postoperative corneal topographies were performed between 1 and 3 months.
The overall impact on ocular aberrations of each of the 2 ablation procedures was analyzed by comparing the root mean square of the higher-order aberrations (RMSH) and the 2 aberrations that are commonly increased after hyperopic LASIK: coma and spherical aberration (SA). Postoperative ocular aberrations were obtained between 1 and 6 months after LASIK.
At 3 months postoperatively, patient satisfaction was obtained through a questionnaire. Patients were asked to report adverse events such as glare and halos, as well as the severity of the symptoms on a scale of 0 to 3 (0 none, 1 few, 2 moderate, 3 intense). All patients filled in this subjective questionnaire.
Outcome Measures and Statistical Analyses
The primary outcome measure was the safety. The safety was evaluated by the safety index and also by the changes in BCVA, expressed as percentage of eyes that have not lost any Snellen lines. The secondary outcome measures were the postoperative mean equivalent sphere (ES) and the aberrometric results. Other outcomes were the efficacy index; the predictability, as the percentage of eyes that were within ±0.50 D of the intended refraction; the contrast sensitivity; and the subjective quality of vision. Safety index was defined as the ratio of the mean postoperative BCVA to the mean preoperative BCVA, while efficacy index was defined as the ratio between the mean postoperative UCVA and the mean preoperative BCVA.
All statistical studies were carried out using the STATA-PC program version 10.0 for Windows PC (Stata Corporation, College Station, Texas, USA). The continuous variables were expressed as mean ± standard deviation. As data were not equally distributed, nonparametric methods were used to compare means for pupil-centered and vertex-centered groups (Mann-Whitney U test). The categorical data were expressed as percentages. As the expected effectives were limited, Fisher exact test was used to compare distribution in the pupil-centered and vertex-centered groups. A P value of less than .05 was considered statistically significant.
Results
Population and Procedure Characteristics
The study population included 30 subjects, 13 male and 17 female. Subjects were divided into 2 groups (n = 30 eyes each), according to surgery centration, either pupil-centered or vertex-centered, by a double-masked randomization method. All patients included completed the study ( Supplemental Figure , available at AJO.com ). Principal features of the 2 groups are summarized in Table 1 . There were no statistically significant differences in the baseline ophthalmic characteristics of both groups. Concerning eyes set for distance vision, in the pupil-centered group the preoperative mean ES was +2.29 ± 0.62 D, while in the vertex-centered group the preoperative mean ES was +2.65 ± 0.80 D ( P = .36). Eyes selected for near vision showed a preoperative mean ES of +2.24 ± 0.64 D in the pupil-centered group and +2.73 ± 0.79 D in the vertex-centered group ( P = .12).
| Pupil-Centered Group | Vertex-Centered Group | P Value a | |
|---|---|---|---|
| Age (years) | 53.4 ± 4.9 | 49.3 ± 9.9 | .98 |
| Pupil size a (mm) | 5.30 ± 0.66 | 5.34 ± 0.94 | .54 |
| Spherical equivalent (D) | 2.26 ± 0.62 | 2.69 ± 0.81 | .15 |
| Cylinder (D) | −0.33 ± 0.4 | −0.41 ± 0.3 | .35 |
For the vertex-centered group, the relative positions of the corneal reflex compared to the center of the entrance pupil (dx laser = 0.25 ± 0.11 mm and dy laser = 0.10 ± 0.08) were similar to the preoperative topographic cartesian coordinates of the corneal vertex compared to the center of the entrance pupil (dx topo = 0.25 ± 0.10 mm and dy topo = 0.07 ± 0.05) ( P = .91 and P = .33). Thus, first Purkinje image coordinates of the laser matched with the preoperative topographical vertex coordinates.
All the postoperative analyses were performed on the 30 subjects except for aberrometric measurements. Of the initially considered 30 eyes for each group, we excluded from ocular aberration comparison 6 eyes from the pupil-centered group and 3 from the vertex-centered group. In these eyes, the pupil size was smaller than the previously determined 6 mm.
Visual Outcomes
At 3 months after LASIK, we found no loss on Snellen BCVA in 28 of 30 eyes (93.3%) in the pupil-centered group and in 25 of 30 eyes (83.3%) in the vertex-centered group. This difference was not significant.
Concerning the safety index, we found no differences ( P = .97) between pupil-centered (0.99 ± 0.04) and vertex-centered groups (0.99 ± 0.08). For most subjects, BCVA was similar to preoperative values. For the pupil-centered group, 2 eyes lost 2 lines of BCVA. For the vertex-centered group, 2 eyes lost 1 line of BCVA and 3 other eyes lost 2 lines of BCVA. A gain of 2 lines of BCVA was found for 1 eye of the vertex-centered group. Safety index results at 6 months after surgery were similar. As shown in Table 2 , safety index seemed to be different considering pupil position. In eyes with small lateral pupil decentration (dx <0.25 mm), we found a slightly lower safety index in the pupil-centered group (n = 20 eyes; 0.98 ± 0.06) than in the vertex-centered group (n = 10 eyes; 1.02 ± 0.06), while for the eyes with large pupil decentration (dx ≥0.25 mm), we found a slightly higher safety index in the pupil-centered group (n = 10 eyes; 1.0 ± 0.0) than in the vertex-centered group (n = 20 eyes; 0.97 ± 0.09). However, these values were not statistically significant ( P = .10 and P = .18 respectively).
| Dx <0.25 mm | Dx ≥0.25 mm | |
|---|---|---|
| Efficacy index a | ||
| Pupil-centered group | 0.95 ± 0.05 | 0.98 ± 0.05 |
| Vertex-centered group | 0.98 ± 0.04 | 0.89 ± 0.10 |
| P value c | .21 | .08 |
| Safety index b | ||
| Pupil-centered group | 0.98 ± 0.06 | 1.0 ± 0.0 |
| Vertex-centered group | 1.02 ± 0.06 | 0.97 ± 0.09 |
| P value c | .10 | .18 |
a Mean postoperative uncorrected visual acuity/mean preoperative best spectacle-corrected visual acuity.
b Mean postoperative best spectacle-corrected visual acuity/mean preoperative best spectacle-corrected visual acuity.
Considering only the eyes set for near vision ( Figure 3 , Top), 5 of 15 pupil-centered eyes (33.3%) and 6 of 15 vertex-centered eyes (40.0%) achieved a distance UCVA of 20/20 or better, while 11 of 15 pupil-centered eyes (73.3%) and 10 of 15 vertex-centered eyes (66.7%) showed a UCVA of 20/32 or better. Considering the eyes set for distance vision ( Figure 3 , Bottom), 8 of 15 eyes (53.3%) in the pupil-centered group and 9 of 15 eyes (60.0%) in the vertex-centered group achieved a UCVA of 20/20 or better, while the amount of eyes that reached a UCVA of at least 20/25 were 15 of 15 (100%) pupil-centered eyes and 14 of 15 (93.3%) vertex-centered eyes respectively. Considering distance and near eyes, there were no statistically significant differences between the 2 groups for distance UCVA. Nevertheless, cumulative histograms shown in Figure 3 suggest that UCVA was slightly better in the pupil-centered group for both near and distance eyes.
Considering only the eyes set for distance vision, efficacy index in pupil-centered (n = 15 eyes; 0.96 ± 0.05) and vertex-centered (n = 15 eyes; 0.93 ± 0.09) groups showed no statistically significant differences ( P = .31). As shown in Table 2 , eyes with small lateral pupil decentration (dx <0.25 mm) showed an efficacy index slightly smaller in the pupil-centered group than in the vertex-centered group (respectively 0.95 ± 0.05 vs 0.98 ± 0.04; P = .21), and eyes with higher lateral pupil decentration (dx ≥0.25 mm) showed an efficacy index higher in the pupil-centered group (0.98 ± 0.05) than in the vertex-centered group (0.89 ± 0.10) ( P = .08).
Refractive Outcomes
Centering the hyperopic ablation on either the entrance pupil or the corneal vertex did not change average refractive outcomes, as most of the eyes treated using both techniques showed little or no refractive error. One month after LASIK, the average ES was +0.03 ± 0.25 D for the pupil-centered group and +0.00 ± 0.49 D for the vertex-centered group in eyes selected for distance vision ( P = 1). The average ES was -0.55 ± 1.01 D in the pupil-centered group and -0.62 ± 0.55 D in the vertex-centered group for the eyes set for near vision ( P = .74). At 3 months, results remained similar for both groups. The average ES was +0.04 ± 0.44 D in the pupil-centered group and +0.00 ± 0.38 D in the vertex-centered group for eyes set for distance vision ( P = 1). The average ES was -0.36 ± 0.56 D in the pupil-centered group and -0.53 ± 0.63 D in the vertex-centered group for eyes set for near vision ( P = .90). In scattergrams of attempted vs achieved spherical equivalent changes, pupil-centered and vertex-centered ablations showed similar patterns of refractive changes ( Figure 4 ).
At 3 months after the operation, 22 of 30 eyes (73.3%) of the pupil-centered group and 20 of 30 eyes (66.7%) of the vertex-centered group were within ±0.5 D of the intended refraction. As shown in Figure 5 , within eyes treated for hyperopia lower than +3 D, 14 of 18 eyes (77.8%) in the pupil-centered group and 10 of 15 eyes (66.7%) in the vertex-centered group were within ±0.5 D from the attempted correction ( Figure 5 , Top). Total eyes with preoperative hyperopia equal to or higher than +3 D that were within ±0.5 D from the attempted correction were 8 of 12 (66.7%) in the pupil-centered group and 10 of 15 (66.7%) in the vertex-centered group ( Figure 5 , Bottom). The differences in refractive outcomes between the 2 groups were not significant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


